Embed Size (px)
Citation preview
Driving Change
Located South East of Melbourne
Peninsula Health

An Overview of Peninsula Health
• Frankston & Mornington Peninsula’s public hospital & health care service
• Operating revenue of $450million
• >900 beds and growing
• Serves a population of 295,000 plus holiday visitors
• 4900 staff and over 800 volunteers
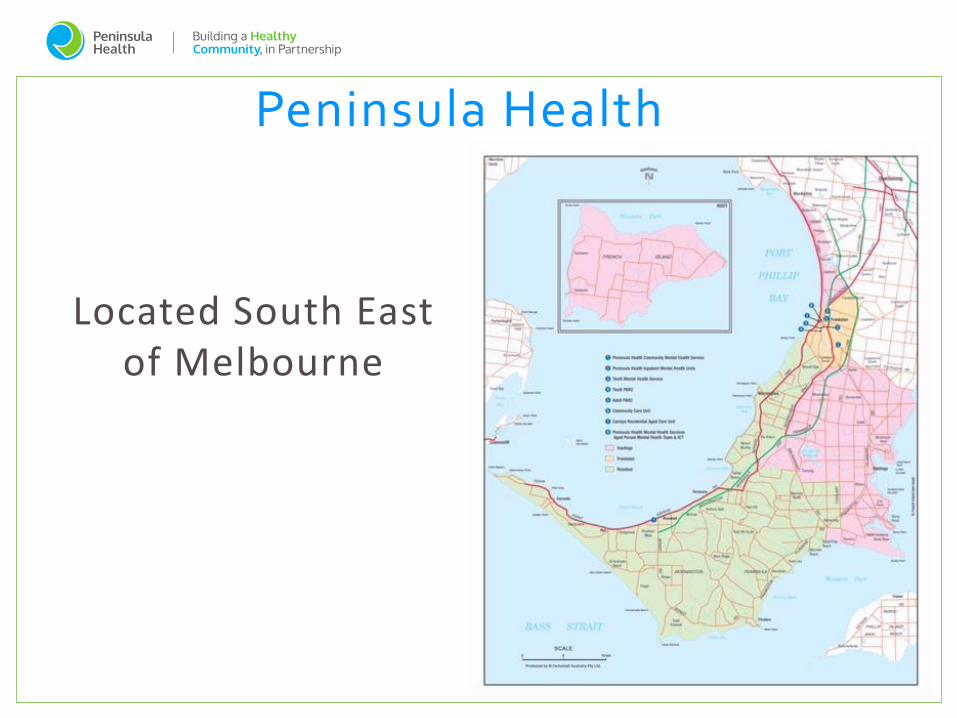
• Providing services across 13 major sites
• All services except major Trauma, Neurosurgery, Ophthalmology, Cardiac Surgery
Services across the Southern Peninsula
Board of Directors
Chief ExecutiveMs. Sue Williams
Executive Directors
A/Prof Jan ChildChief Operating Officer
RoMANCCC
Mr. Brendon
GardnerChief Operating Officer
Frankston Hospital
Dr. Fergus KerrExecutive Director
Medical Services
Mr. Simon Brewin Executive Director
Planning &
Infrastructure
Professional Issues
Medical Susannah Ahern
Nursing Jan Child
Allied Health Jan Child
Legal David Goldberg
Mr. David
AndersonExecutive Director
Finance
Ms. Kelly GilliesExecutive Director
Human Resources
Public Relations Andrew Heslop
1. Person centred care is at the core of what we do.
2. Service Planning - to deliver timely and appropriate care.
3. Partnering to support the health and wellbeing of our community.
4. Our Workforce - Attracting, retaining and developing high quality staff and volunteers.
5. Safety and Quality - We prioritise patient safety in everything we do.
6. Learning, teaching and research.
7. Strengthen our sustainability to support core activities.

Most Disadvantaged
Frankston North
Rosebud West
Hastings
Rosebud
Tootgarook
Frankston
Most Advantaged
Portsea
Arthurs Seat
Mt Eliza
Merricks North
Red Hill South
Mt Martha
Extremes of Wealth and Poverty
Frankston North ranked as the 7th most disadvantaged area in Victoria
Frankston and the Mornington Peninsula measure notably worse on a number of health inequality indicators compared to the Victorian Average
• High Smoking rates 17.4% - FCC, Vic average 15.5%• High Dementia rates • High #’s Early school leavers FCC 36.8%; State 27.9%• High #’s Single Parent Families • Lower breastfeeding rates 30% - FCC, State 39% • High numbers of teenage pregnancies FCC - 16.4/1000, State 10.6/1000 • Low Health literacy -57% population below optimal• High Unemployment - Frankston 6.5% :State 5%• High Rates Child Protection Orders and family violence (3rd highest in state)• Higher Crime rates Frankston (above state average for all offences except burglary,
robbery and road fatalities)• High gambling machine losses• Higher rates of disengagement from education and employment for Frankston
youth (15-24) FCC 14.8% ; State 10.7%
Our Community
Made improvements prior with some changes but with the opening of a new block. 2 wards, a new Emergency Department. Opportune time to review our models of care.
Review via the lens of a patient’s journey

Frankston Hospital Stage 3
92 new acute beds
New Emergency Department
Why Change?
The need for change
Poor patient flow is associated with
- poor patient outcome
- decreased patient satisfaction
- decreased staff satisfaction
Time based targets are a surrogate marker to these which are our primary outcomes
Our Challenges
Environment
EDIS
Principles of Care
Building our Priorities
Principles
Models of Care
Collaboration
IT Enablers
Data
Right Treatment by the
Right Team at the
Right Time
Our Change Principles
Patient Centered Care - Patients are our focus. What would we want
our patients to experience?
Patient Care is a Continuum and not done in “silos”.
The Right Environment
Emergency - The role of the ED - Resuscitate, Risk Stratify, Treat.
Patients who no longer need ED treatment need to have a timely
decision and disposition plan
Acute Assessment and Admission Unit - Care is clinically handed
over. Majority of our ward admissions are via this path.
Emergency Short Stay Unit - Optimising utilisation
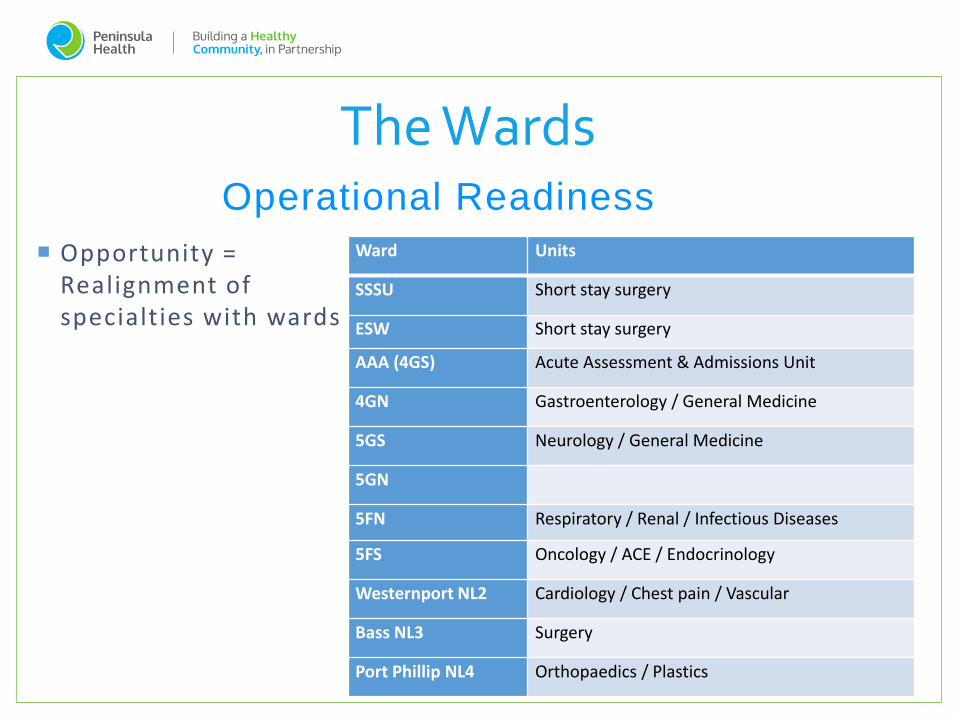
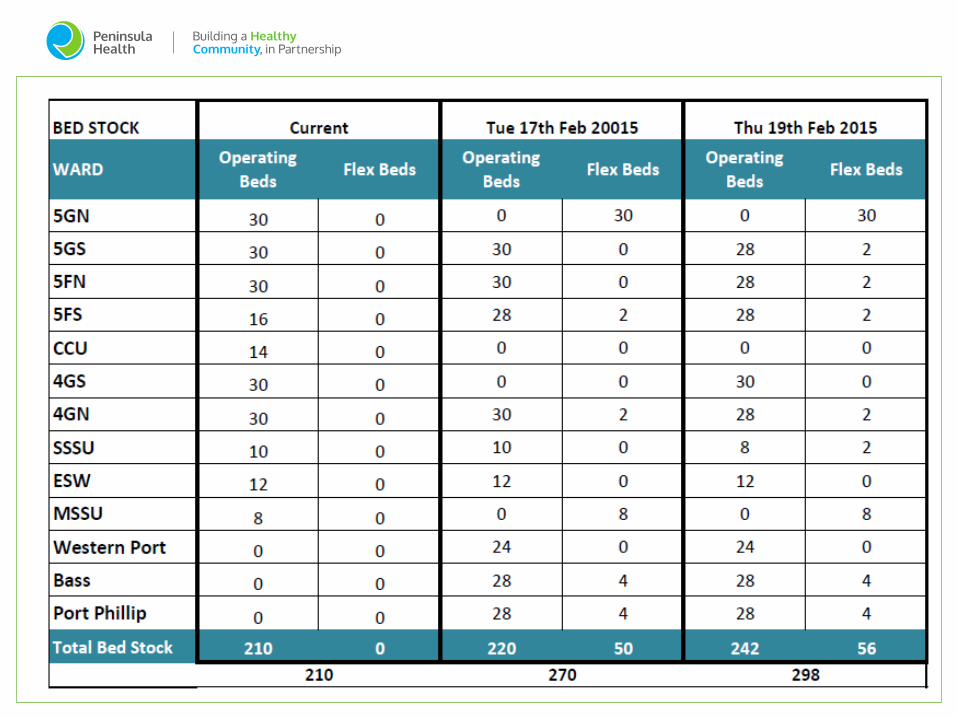
The WardsOperational Readiness
Ward Units
SSSU Short stay surgery
ESW Short stay surgery
AAA (4GS) Acute Assessment & Admissions Unit
4GN Gastroenterology / General Medicine
5GS Neurology / General Medicine
5GN
5FN Respiratory / Renal / Infectious Diseases
5FS Oncology / ACE / Endocrinology
Westernport NL2 Cardiology / Chest pain / Vascular
Bass NL3 Surgery
Port Phillip NL4 Orthopaedics / Plastics
Opportunity = Realignment of specialties with wards
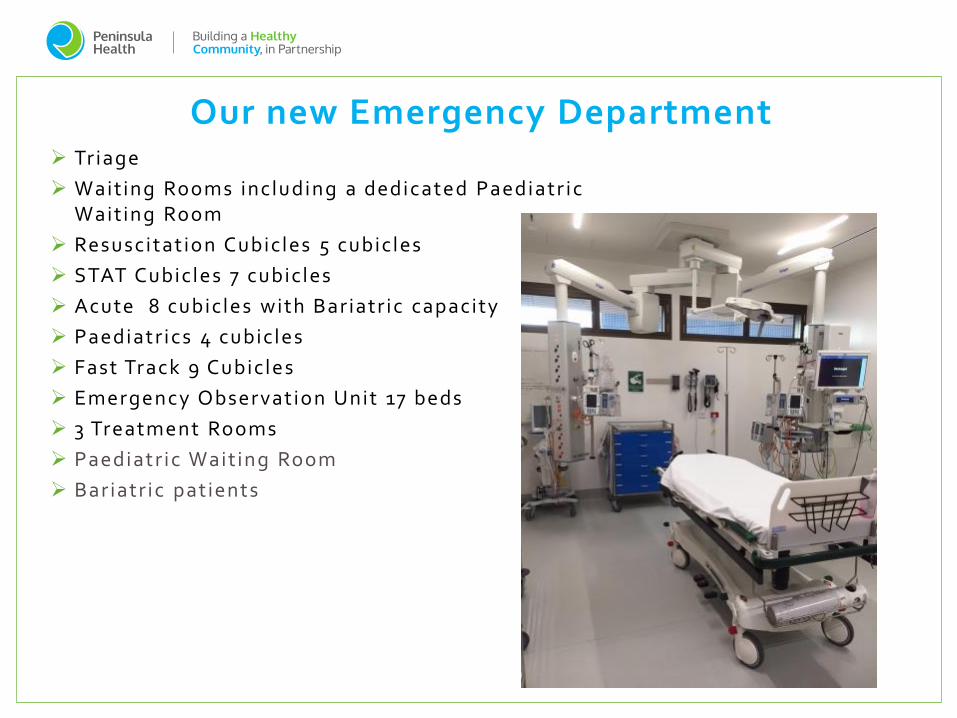
Triage
Waiting Rooms including a dedicated Paediatr ic Waiting Room
Resuscitat ion Cubicles 5 cubicles
STAT Cubicles 7 cubicles
Acute 8 cubicles with Bariatr ic capacity
Paediatr ics 4 cubicles
Fast Track 9 Cubicles
Emergency Observation Unit 17 beds
3 Treatment Rooms
Paediatr ic Waiting Room
Bariatr ic patients
Our new Emergency Department
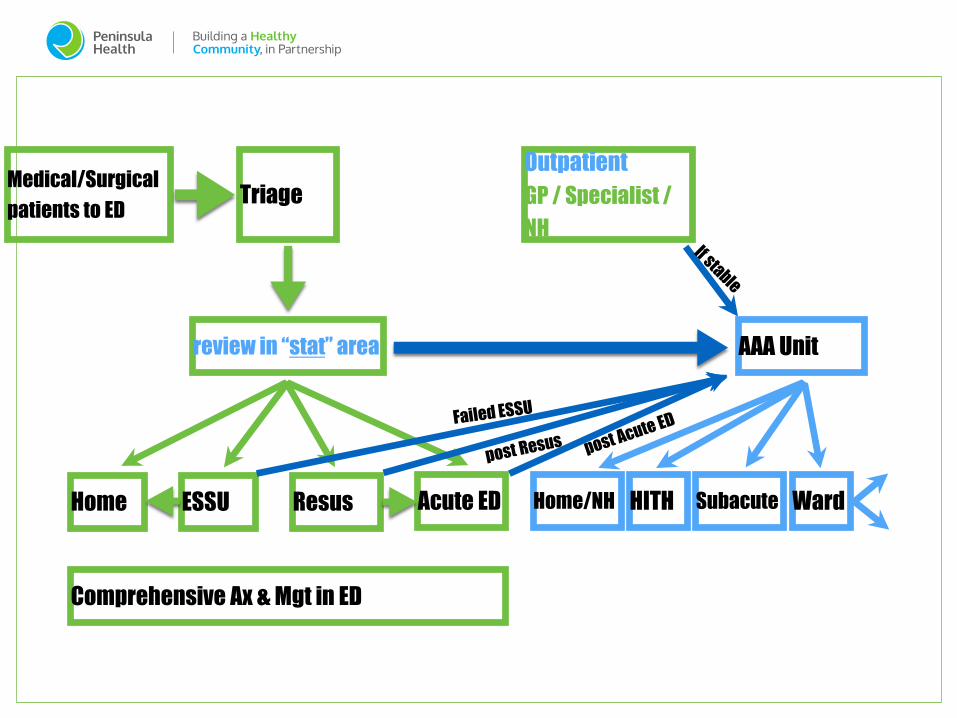
Medical/Surgical
patients to EDTriage
review in “stat” area
Home ESSU Resus Acute ED
Comprehensive Ax & Mgt in ED
AAA Unit
Home/NH HITH Subacute Ward
Outpatient
GP / Specialist /
NH
Emergency Department Information System (EDIS)
Investment into a new EDIS
Aim for a complete paperless system
User friendly interphase with robust database backend
Integration within health system
PH ED – One of the EDs which have gone almost completely electronic.
Implementation – Project development with end user customisation, Training, Launch, Ongoing training.
Implementation better than expected. Anticipated inefficiencies on launch settled very quickly.
EDIS
Need. Staff were wanting something new.
Generational
Benefits
Transparency/ Reduction of duplication
IT Enablers
Emergency Department Information
System
Touch On Touch Off Capability
Emergency Dashboard
Data Reports
Data Driven Change
Data – friend of foe
KPIs
Accountability
Clinician’s take on data. Perceived to always be negative. Evidence based medicine.
Data skeptics – Data needs to be accurate but also need to understand what data is being used for.
Data rich
Systems in place to be able to capture and extract data
Needs to be easy on front face but be robust in the back end
DATA

Elite Sports
Personal Dashboards
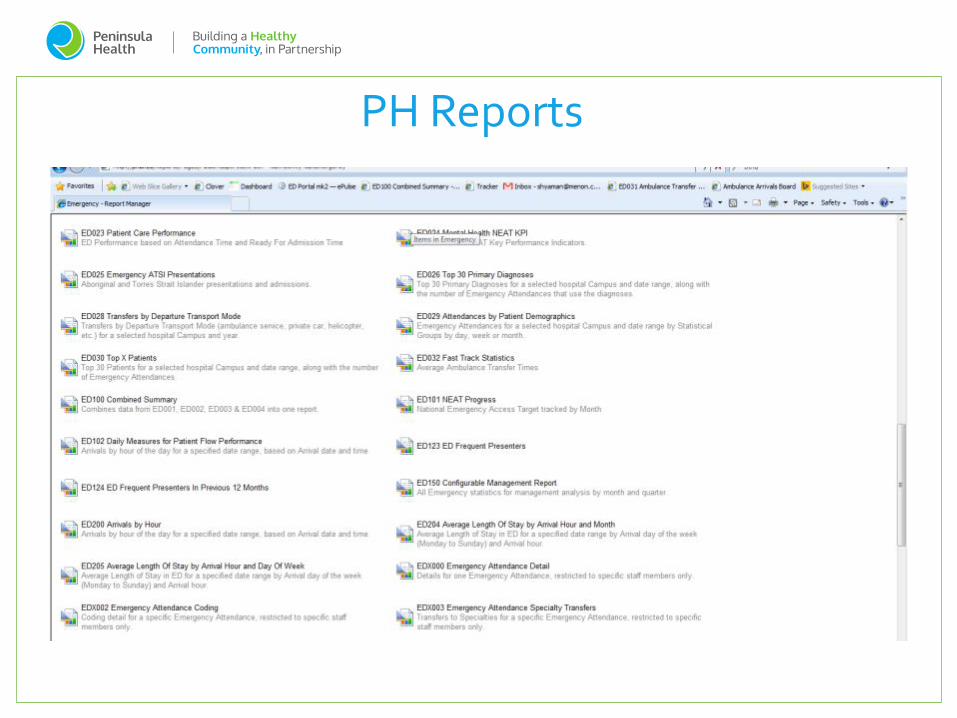
PH Reports
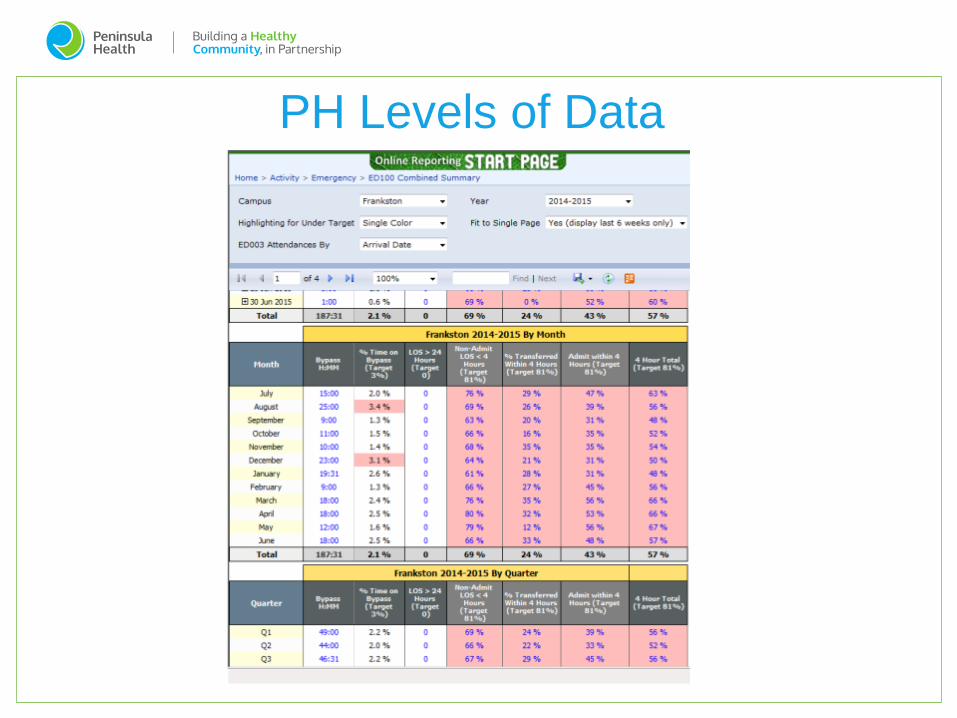
PH Levels of Data
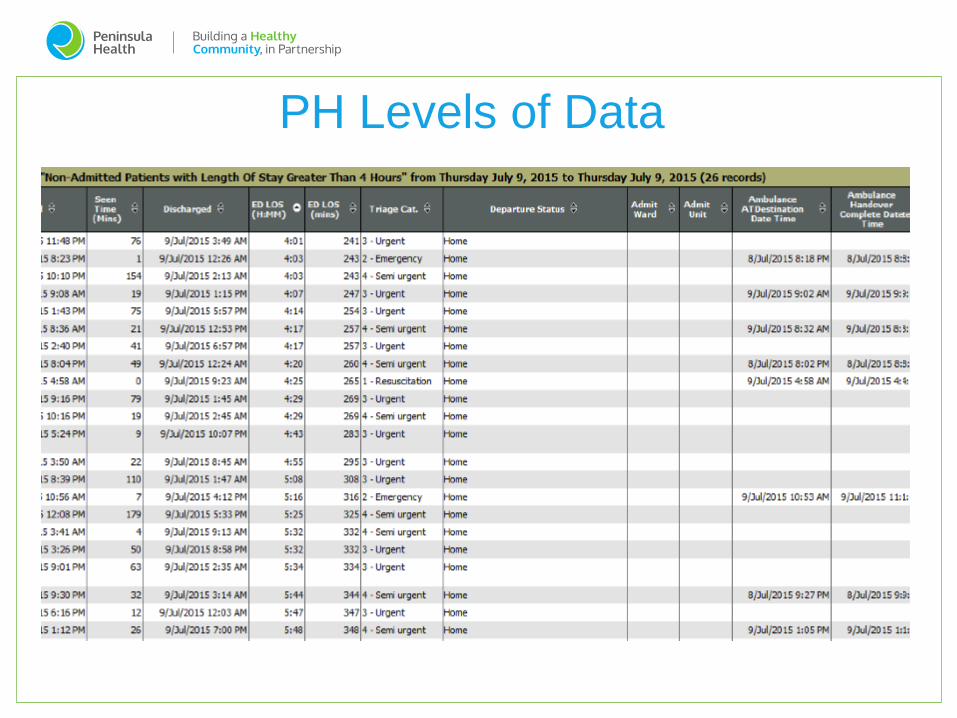
PH Levels of Data
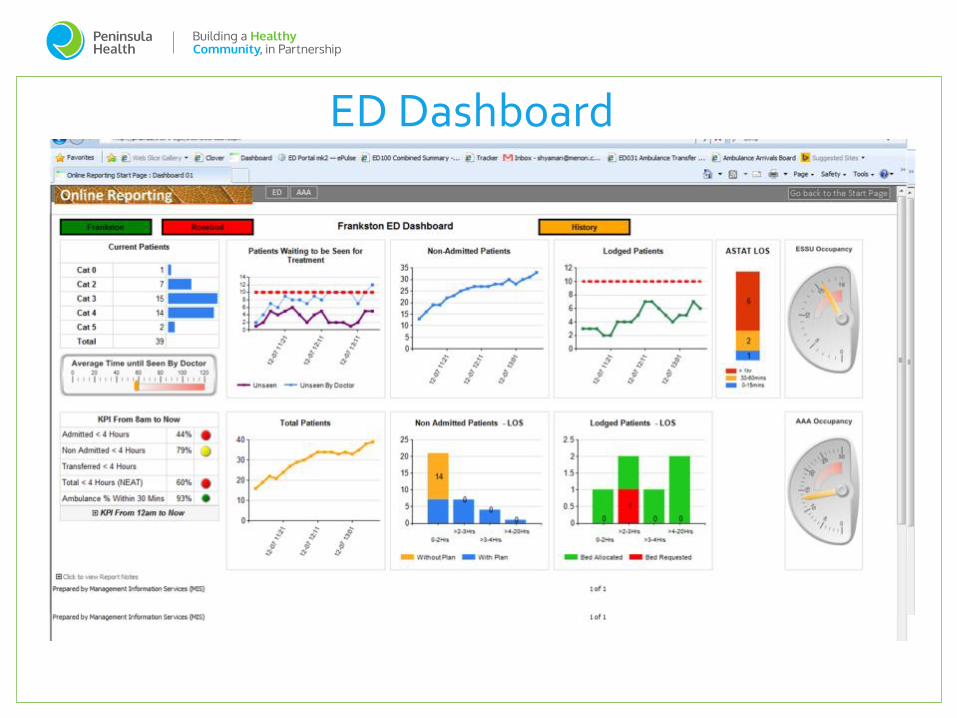
ED Dashboard
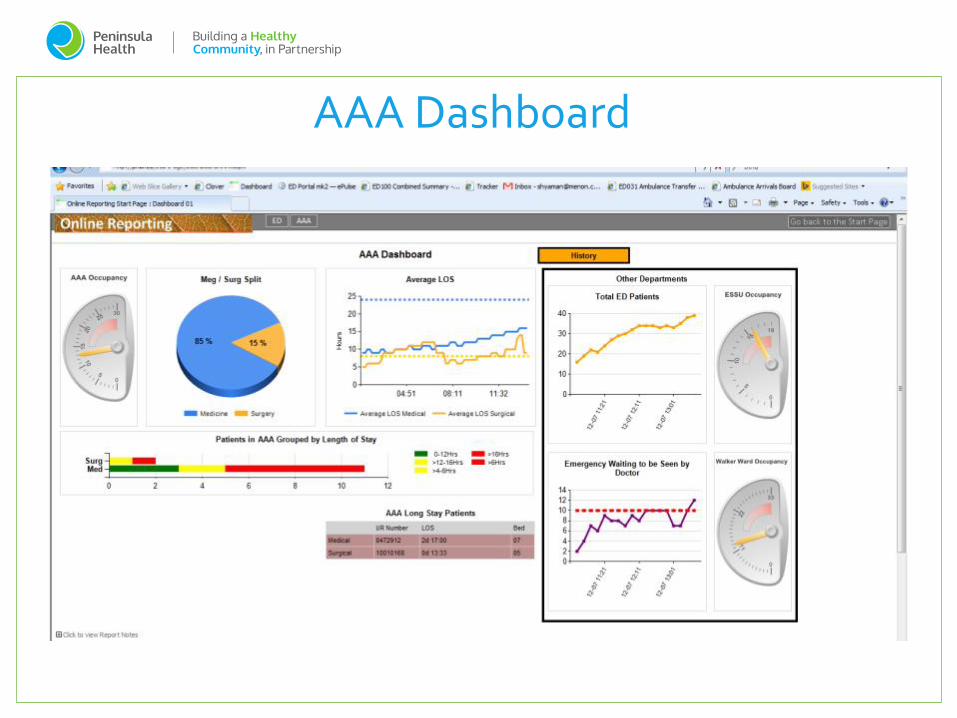
AAA Dashboard

What works
Engaged Health Service - uniform goal
Trust
Communication
Information
Old “habits”- Keeping to our principles
Consistency
Surge
Demand
Challenges
Key is the team to accept the need for change.... It
needs to come back to patient care.
Keep reviewing process. Change will always need to
occur as our circumstances will change, we need to be
flexible but wary of change fatigue .
Use opportunities for timing of change where possible
Data is your friend.
Displayed data needs to be customized and be
meaningful to the team who is looking at it
Key Learnings
Board of Peninsula Health
Chief Executive Officer, Ms Sue Will iams
Chief Operating Officers
Executive Support
MIS and HIS Team
Staff of Peninsula Health
Consumers
Acknowledgements