Embed Size (px)
Citation preview
An Exciting Journey: Four Phases to Population Health
Management Maturity
American healthcare system is undergoing change at an unprecedented pace.
New care models are directed at preventive care, proactive chronic disease care, and utilization management and are being implemented in conjunction with payment models that incorporate financial risk-taking and incentive management.

Emerging provider-driven, practice-based population health management (PHM) programs open up exciting opportunities that build on the physician-patient relationship and demand accountability for outcomes.
PHM is not a new concept.
Predominantly driven by payers, it has been practiced piece-meal over the last 20 years, with generally unsatisfactory results as measured by healthcare costs.
In most cases, payer-driven PHM programs consciously avoid the physician role due to conflicting incentives—the more services clinicians provide, the higher their payment.
Four-Phase Model
Despite their promise, provider-led PHM programs do not just form overnight.
Medical Groups must transition from the traditional siloed payer-driven PHM program to a provider-driven model that is patient-centric and payer-agnostic.
As organizations make this journey, they will travel through four phases of maturity (Figure 1):
The Pilot
Care Program Development
Physician-Driven Services
True Patient Engagement
Increasing financial returns from shared savings, performance-based, or risk-based rewards follow each phase.
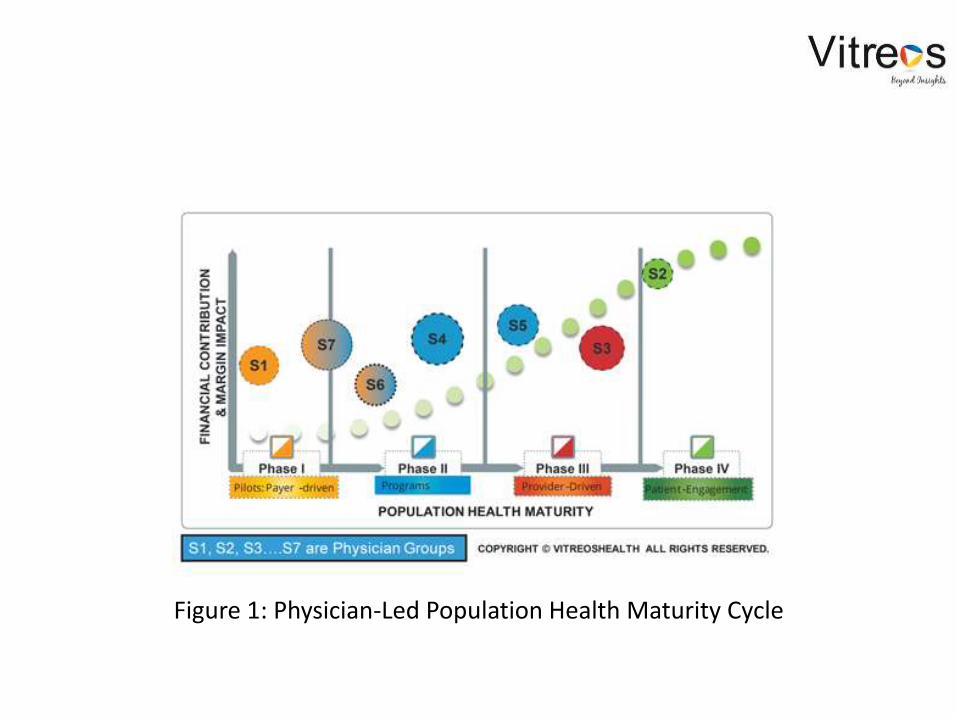
Figure 1: Physician-Led Population Health Maturity Cycle
Each phase has its own challenges across multiple dimensions—leadership, care management processes, information technology (IT)/data analytics, physician alignment, and patient engagement.
These challenges change as groups progress through the four phases of PHM maturity.
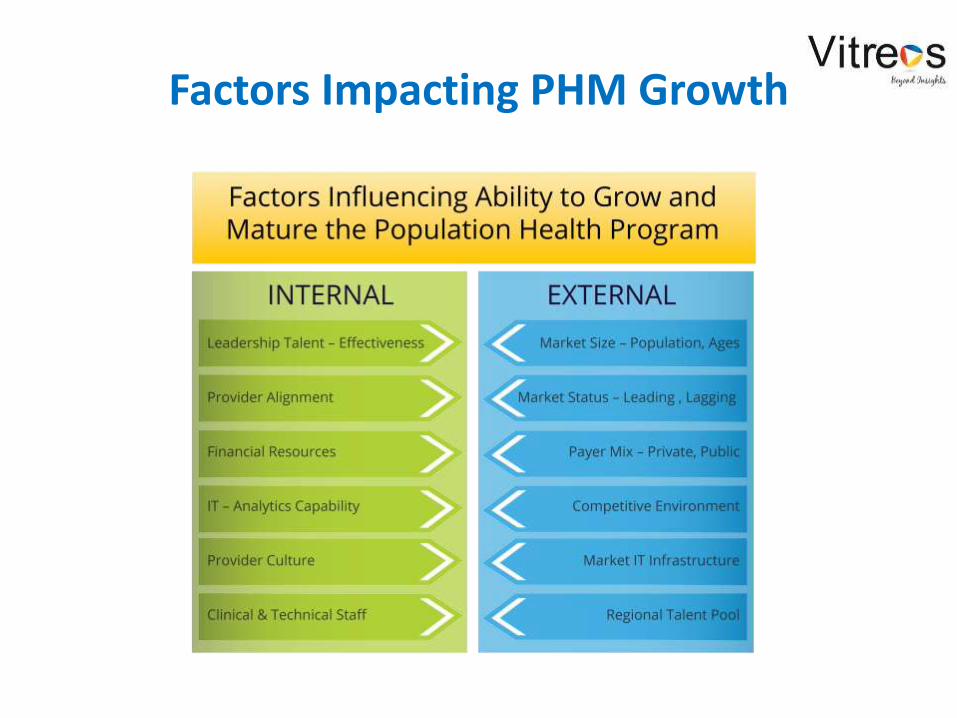
Factors Impacting PHM Growth
Phase 1: The Pilot
The pilot is when an organization will apply to become an accountable care organization (ACO) with the Centers for Medicaid & Medicare Services (CMS)or a patient-centered medical home (PCMH) with commercial payers and negotiate its first risk-based or pay-for-performance contract.
In the pilot phase, the organization assesses its capabilities and the potential benefits of developing a PHM program.
Based on the findings of the readiness assessment, an organization could start on the path to a PHM program as an ACO or PCMH with one payer for a small population of 10,000 to 15,000 members.
Leadership:Executive leadership (e.g., CEO, president) sets the priority by communicating a vision of the PHM program for the organization.
Care Management Processes: In Phase 1, most of the PHM processes are driven by the payer. The payer will want to dictate quality performance reporting needs, patient care protocols, and provider incentives.
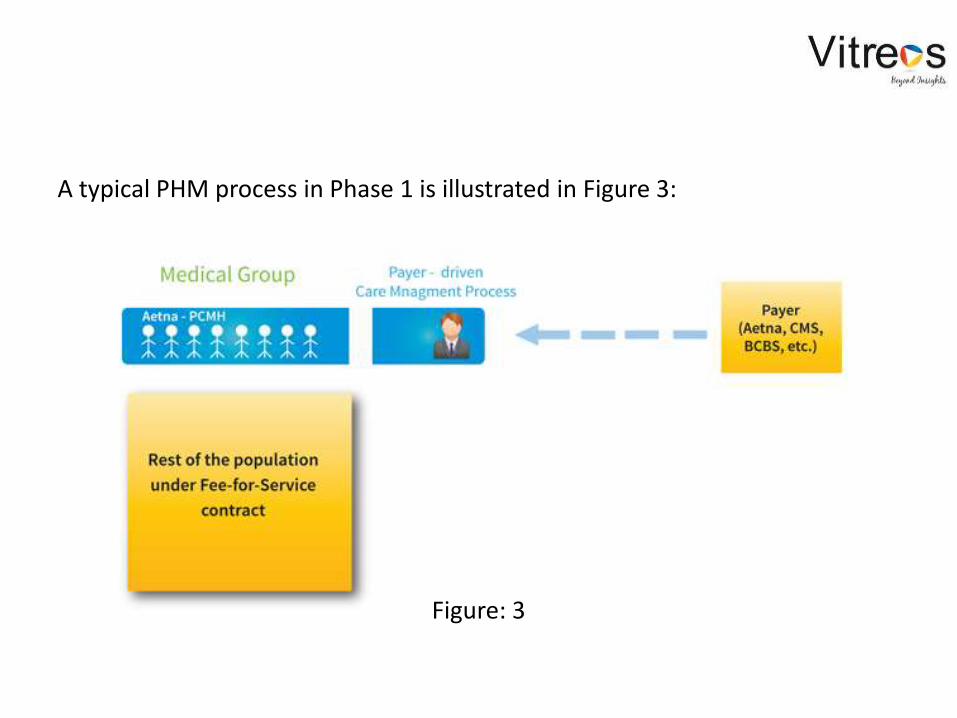
A typical PHM process in Phase 1 is illustrated in Figure 3:
Figure: 3
IT/Data Analytics:During Phase 1, technology requirements for the new care processes are identified and a roadmap for future infrastructure and applications needs is developed. The priority at this stage is to get the pilot program rolling with minimal investment.
Physician Alignment:On the clinical side, most of the challenges in the pilot will stem from attempting to garner physician alignment.
Physicians are asked to focus more on preventive care and use clinic visits as opportunities for proactive chronic care management in order to identify and address any gaps-in-care. Initially, most of these processes will be ad hoc, episodic, and not systematically followed across the provider network.
Patient Engagement:Patient engagement in Phase 1 is very basic and also driven by payers. Most of the proactive patient involvement relates to educating patients about managing their chronic diseases.
Challenges/Recommendations:
The “consultant trap”
IT stickiness
Naysayers
Divided attention
Phase 2: Care Program Development
After experiencing financial benefits from the initial pilot, the organization gears itself for Phase 2 of the maturity cycle of the PHM initiative.
This preparation is reflected in increased budgets for staffing, care management processes, and technology, whose scale-up costs are estimated from the pilot phase.
To be successful in phase 2, an organization must undertake more risk-based contracts and manage a larger population under different payment models—PCMH, ACO, shared services, bundled payments, etc.
Leadership:Phase 2 requires a strong PHM leadership to maintain focus on the long term. Providers will create a management level position.
Providers will also start developing their own standardized care managementprocess based on their experiences during the pilot phase.
Care Management Processes:Phase 2 starts with most of the care management processes still driven by the payer. Each payer will want to dictate its own quality performance reporting needs, patient care protocols, and incentives. In most cases, the payer provides the resources for the dedicated care coordination services; care coordinators may operate within provider facilities, but will still be under the payer’s payroll.
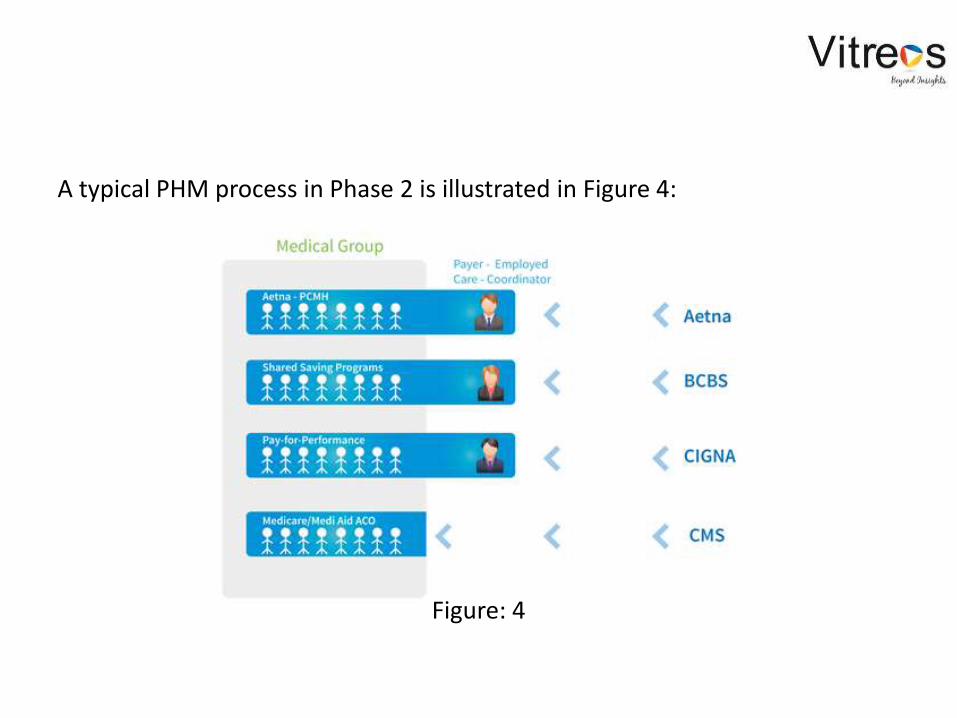
A typical PHM process in Phase 2 is illustrated in Figure 4:
Figure: 4
IT/Data Analytics:Goals within IT move from basic quality reporting to population analytics capabilities to identify gaps in care, risk stratify populations, determine which physician patient populations are meeting quality and cost targets, and report outcome measures.
Physician Alignment:Phase 2 starts the shift from anecdotal-driven to data-driven performance management. Organizations use the data to identify disparities of care costs and outcomes at the physician level. Performance metrics are outcomes based (e.g., ER visits, hospitalizations, re-admissions, utilization, etc.).
Patient Engagement:In Phase 2, the trust between the physician and patient is leveraged to implement PHM programs more effectively. Providers start identifying population cohorts—high cost, high risk, high utilizers, etc. Patient engagement is proactive, involving outreach programs and physician visits to ensure care compliance and medication adherence.
The end of Phase 2 is where power starts shifting to the provider; the provider knows what actions need to be taken to start driving the PHM process, but also recognizes the organization’s gaps in capabilities and need to build internal competencies to start taking control of the process.

Challenges/Recommendations:
Clinical integration chaos
Over investing in IT
Limited resources
Data disorder
Phase 3: Physician-Driven Services
The key in Phase 3 is designing and incorporating PHM processes with physician-led, practice-based care management processes.
Phase 3 puts even greater focus on provider accountability as most of the PHM processes are now driven by provider organization resources.
Managing populations starts to become payer-agnostic.
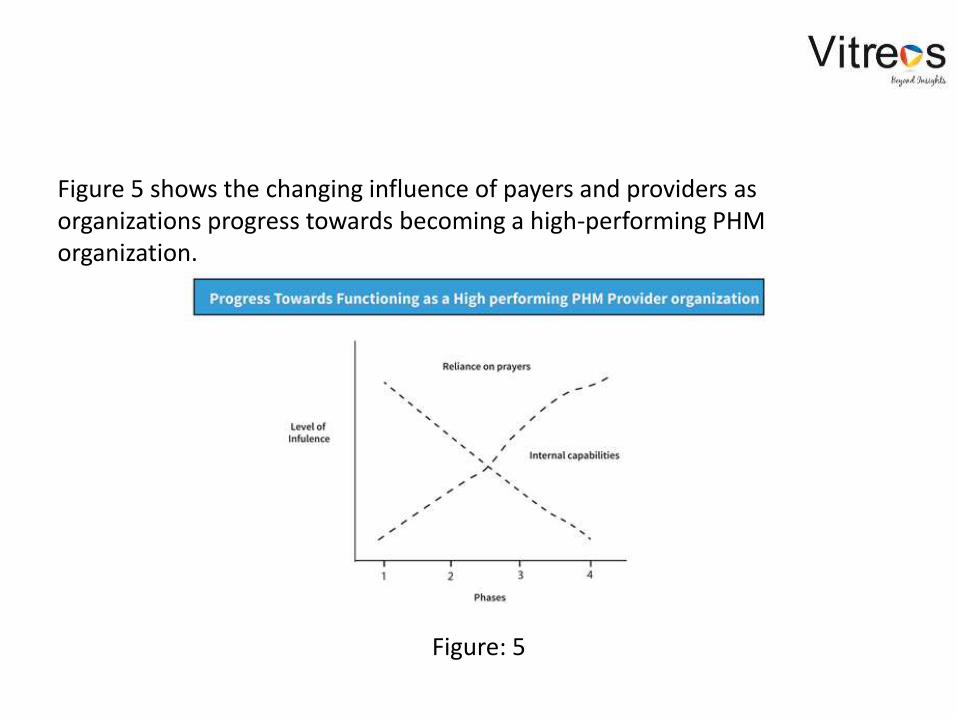
Figure 5 shows the changing influence of payers and providers as organizations progress towards becoming a high-performing PHM organization.
Figure: 5
Leadership:The priority of executive leadership is to transition from developing to operationalizing PHM processes.
Care Management Processes:By Phase 3, the provider organization has more than 30 percent of business under risk-based contracts; PHM care processes are also extended to the practice’s entire population with the mindset that all patients are under “pay-for-performance” contracts.
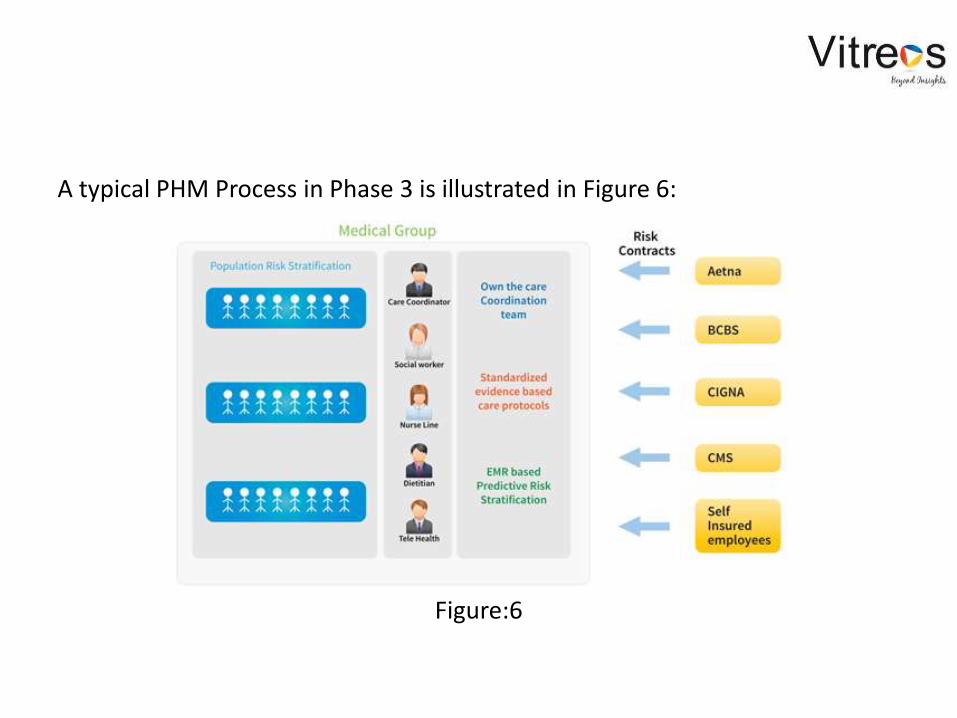
A typical PHM Process in Phase 3 is illustrated in Figure 6:
Figure:6
The provider organization now employs their own care coordination team led by physician leadership, establishes the standardized evidence-based care protocols, and starts leveraging the EHR data for predictive modeling and risk stratification.
For the first time, the providers are able to marry clinical data from the EHRs with claims data and demographics to get a 360 degree view of the patient’s risk. Providers now understand clinical and non-clinical risk factors by patient and which factors can be controlled and which cannot.
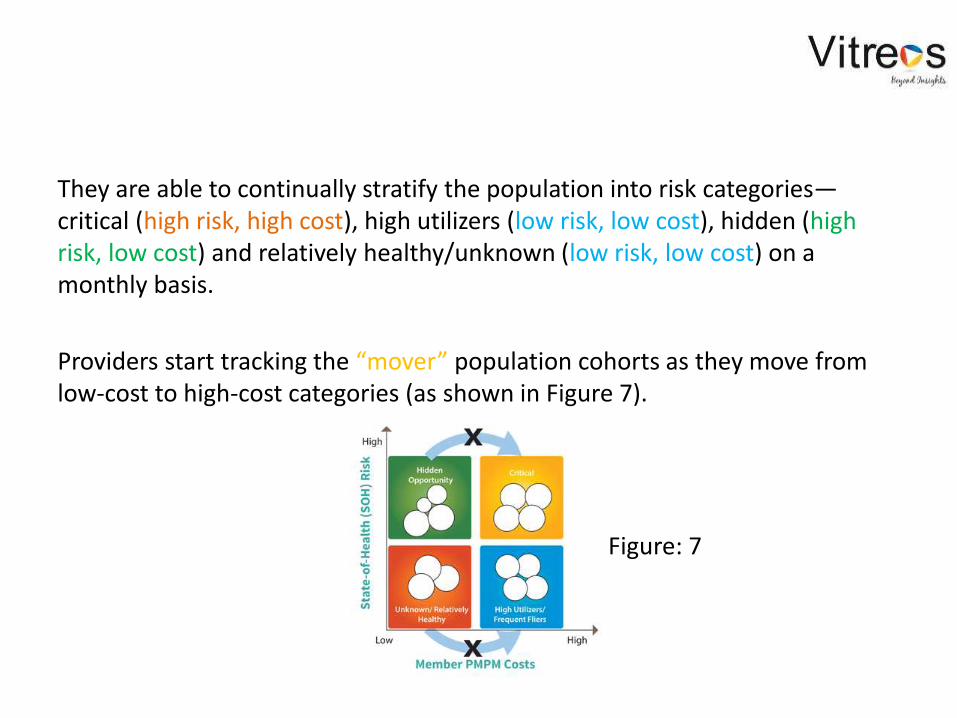
They are able to continually stratify the population into risk categories—critical (high risk, high cost), high utilizers (low risk, low cost), hidden (high risk, low cost) and relatively healthy/unknown (low risk, low cost) on a monthly basis.
Providers start tracking the “mover” population cohorts as they move from low-cost to high-cost categories (as shown in Figure 7).
Figure: 7
IT/Data Analytics:Required infrastructure in Phase 3 includes an internal data warehouse to collect data from disparate sources—EHR, payer claims, practice management system, health risk assessments etc. Tools must also include flexible quality reporting engines to enable reporting of different measures for different risk programs.
Physician Alignment:In Phase 3, physician alignment is completed. There is transparency of performance data by physician, facility, program, and patient cohort.

Patient Engagement:Every patient encounter is leveraged to address the care gaps identified by the analytics and seamlessly reported to the physician at point of care through the EHR. Each patient is treated with the same care protocols irrespective of the health plan.
The physician and care management teams work as a team and are evaluated by their PHM metrics.
Challenges/Recommendations:
Information technology trap
Non-champions
Shifting accountability
Phase 4: Patient Engagement
In Phase 4, PHM becomes the normal course of business.
The patient is now treated truly as a “healthcare consumer” and patient engagement becomes a round-the-clock effort.
Patient care becomes integrated care, with hospitals, physician groups, skilled nursing facilities, and community health services all working together to provide a continuum of care.
Leadership:Leadership requirements in Phase 4 are totally different from requirements in Phase 1. Every discussion and decision about care is data driven.
Strategic leadership skills include the ability to work in collaborations with other providers in the integrated network and learning to manage partner assets (e.g., imaging/diagnostic equipment) without owning them.
Care Management Processes:Irrespective of the payer and risk contract, the business of care is driven by a systematic process that can be broken down into these steps:
Analyze the total population and micro-segment it into cohorts based on
clinical and non-clinical risks.
Identify the drivers of each risk and whether they are controllable or
non-controllable in the short or long term.
Design optimal care management programs with both provider-driven
and patient engagement components
Prioritize the care programs based on costs, complexity to execute,
available competencies, and time to realize value. Execute the programs
by aligning the incentives for caregivers and patients
Track ongoing performance to measure program effectiveness, provider
performance, and patient adherence. Tweak the programs to fix any
gaps.
Report the performance in terms of the impact and trends on outcomes
(hospitalizations, re-admissions, ER visits) and per member per month
costs.

The PHM process become very sophisticated with a closed-loop continuum of care as shown in Figure 8.
Figure: 8
IT/Data Analytics:An organization in Phase 4 is in the race to become a “world-class” healthcare leader. Technology and data provide the foundation for how care management is designed and delivered.
Physician Alignment:On the clinical side, care management functions are decentralized to physician clinics to increase access. Leadership needs to focus on keeping physicians engaged and ensure there is minimal performance burn out.
Patient Engagement:Patients start operating as active healthcare consumers by becoming more involved in their own health decisions and understanding their risks and how they can engage with providers.
Health plans have significant incentives and disincentives for patients to adhere to best practices and keep healthy.
Challenges/Recommendations:
Failure at the top
Data security
IT systems integration

Population health management that keeps the population healthy and lowers healthcare costs is a journey.
The time it takes an organization to move from one phase to the next depends on leadership will and commitment, organization willingness to change, financial resources, external market demands, and flawless execution.
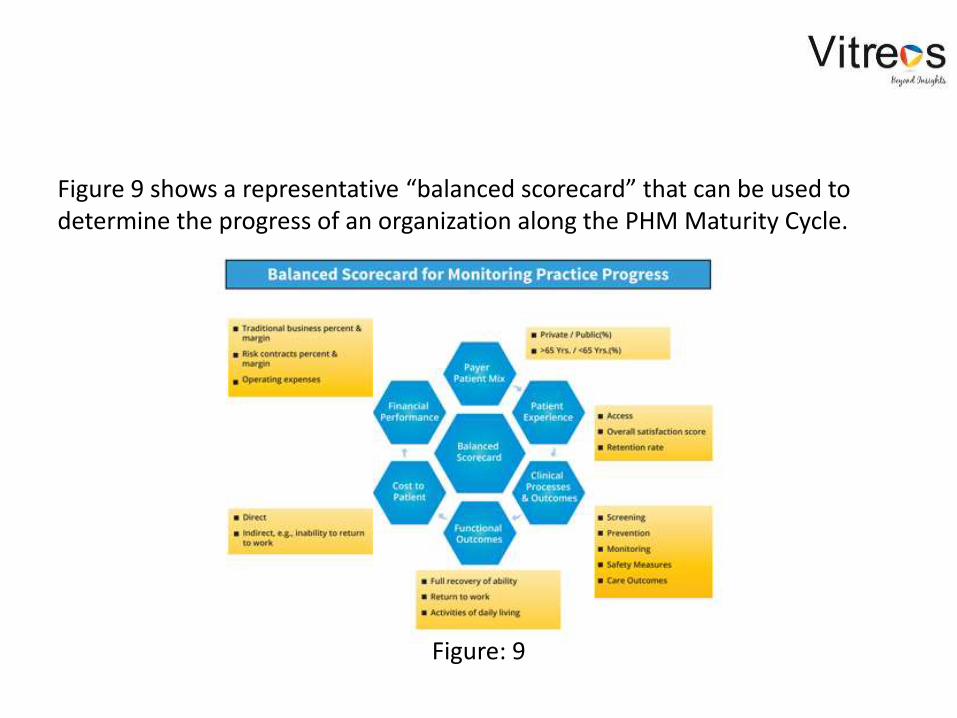
Figure 9 shows a representative “balanced scorecard” that can be used to determine the progress of an organization along the PHM Maturity Cycle.
Figure: 9
For the organization to inculcate the values and vision of the retooled care delivery system, the CEO and senior executives must embrace the new model of care early on.
The velocity of change will differentiate the winners from the losers in the race for market leadership in the changing healthcare delivery ecosystem.
Authors: Dr. Michael (Mike) Deegan, Clinical Professor for Healthcare Leadership
and & Innovation in the Naveen Jindal School of Management at The University of Texas at Dallas.
Karen Kennedy, CEO of Kangent Consulting, Inc. Former CAO of Medical Clinic of North Texas (1999 -2012).
Jay Reddy, Founder & CEO of VitreosHealth, a leader in predictive population analytics.
Read full article here:http://www.vitreoshealth.com/index.php/population-health-management-maturity
For any query please contact Sandeep Misra at [email protected]





























