Embed Size (px)
Citation preview

Exotropia
Pediatric Ophthalmology
LSU Medical Center in Shreveport

Cause of Exotropia
• In most cases cause is unknown• Theories
– Excess divergence– Deficient convergence– Anatomic factors
• Familial tendency present• Refractive errors
– Average for age unless sensory due to marked anisometropia

Classification According to Fusion Status
• Exophoria: X
• Intermittent Exotropia: X (T)
• Exotropia: XT
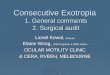
Classification According to AC/A
Deviation AC/A Example
Convergence Insufficiency
Low X= 0, X’= 12, orX(T)= 20, XT’=40
Basic Normal XT= XT’= 20
Divergence Excess
High XT= 35, XT’=10
Exotropia: Clinical Types
1. Congenital
2. Sensory
3. Typical Childhood, or intermittent exotropia
4. Convergence Insufficiency
5. Consecutive
Secondary Exotropia
• Confusing term but still used at times• May mean occurs following surgery for ET, or• May mean sensory exotropia due to an
underlying condition, e.g., anisometropic amblyopia, retinoblastoma, cataract
• Better to use either consecutive or sensory rather than secondary to describe exotropia

Pseudoexotropia: often due to large angle kappa (e.g. ROP)

Pseudoexotropia

Pseudoexotropia

Pseudoexotropia: Apert syndrome

Congenital Exotropia
• Rare• Constant Exotropia• Large angle• Often associated with other neurologic defects• Only treatment is surgical

Sensory Exotropia
• Poor vision in one eye leads to exotropia• Sensory esotropia or exotropia may occur• Causes
– Marked anisometropia• E.g., unilateral high myopia
• Retinoblastoma (22% present with strabismus)• Unilateral cataract

Sensory Exotropia: Treatment
1. Treat underlying cause if possible• E.g. remove cataract, treat amblyopia
1. Surgery for exotropia • Fusional outlook variable• Small XT often best left alone
Convergence Insufficiency: Two Subtypes
1. Ex= 0, Exophoria or Exotropia at near• Low AC/A ratio• Remote NPC• Poor fusional convergence amplitudes• Usually responds to convergence exercises
• Website: “ Computer Orthoptics (HTS)” exercises online or in office vision therapy combined with home therapy
• May treat with base in prism• Usually do poorly with surgery

Convergence Insufficiency: Second Subtype
• XT at distance, larger XT at near– Deficient accommodative convergence– Very low AC/A ratio– Poor response to convergence exercises– Often undercorrected with recess LR OU– Treatment: unilateral recess/resect or recess/tuck

Typical Childhood Exotropiaor Intermittent Exotropia
• Onset 6 months to 6 years of age• Average refractive errors• Deviation usually noted first with distance vision• Often normal sensory pattern when eyes aligned• Many progress through different phases• Some remain stable and do not progress

Progression of Exotropia
• Phoria→ Tropia
• Distance deviation> Near deviation
• Progression more rapid under age 6, but progression in adulthood common also(may present with diplopia)

Typical Childhood ExotropiaPhase 0
• X but no XT and no X (T)
• Usually no symptoms
• No suppression

Typical Childhood ExotropiaPhase 1
• X (T) present, Ex’ = 0
• Mostly controlled
• Symptoms often present– Diplopia: may close one eye– Noted by peers
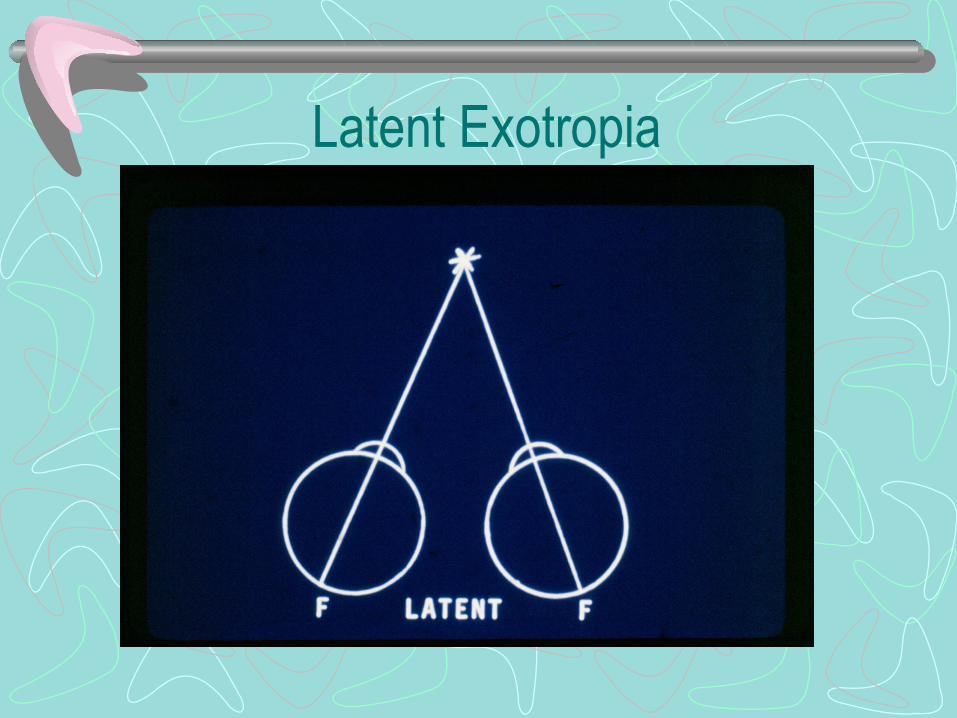
Latent Exotropia
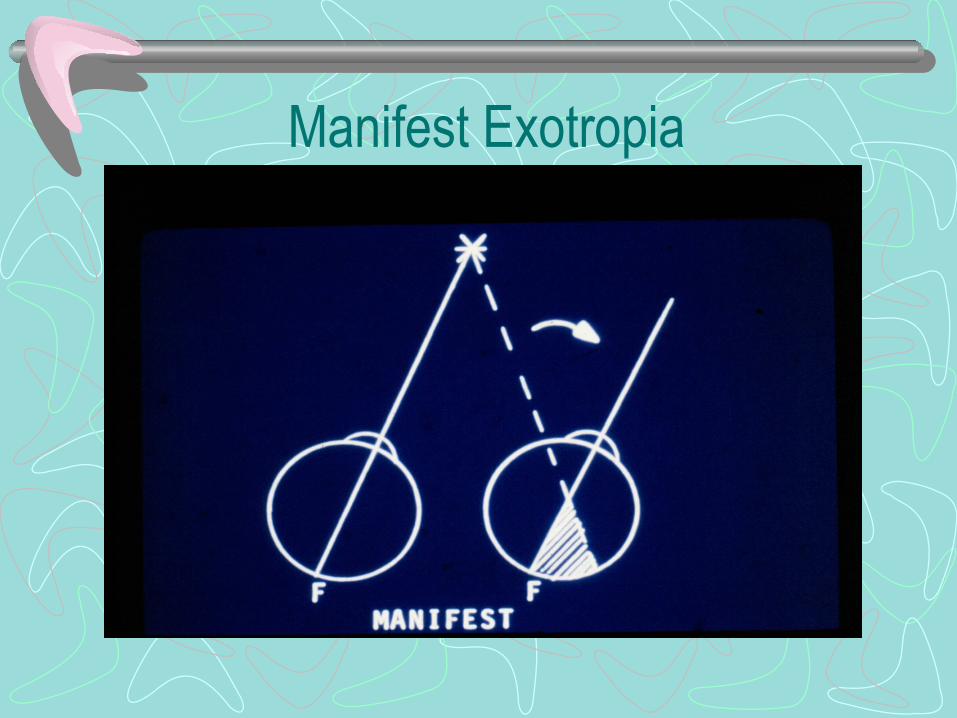
Manifest Exotropia

Exotropia: Area of Temporal Retina Suppressed

Binocular Perimetry In Exotropia: Nasal Scotoma

Alternating Scotoma in Alternating Exotropia

Typical Childhood ExotropiaPhase 2
• XT constant at distance, X’ or X(T)’• Deviation noticeable• Fewer symptoms: suppression usually present• Divergence excess pattern ( or pseudo-
divergence excess) common

Typical Childhood ExotropiaPhase 3
• XT constant at distance and near• Noticeable• Usually no diplopia present• Amblyopia may be present

Clinical Course of Typical Childhood Exotropia
Phase Deviation at distance
Deviation at near
Diplopia Suppression
0 X X’ _ _
1 X(T) X’ + _
2 XT X(T)’ or X’ _ +
3 XT XT’ _ +
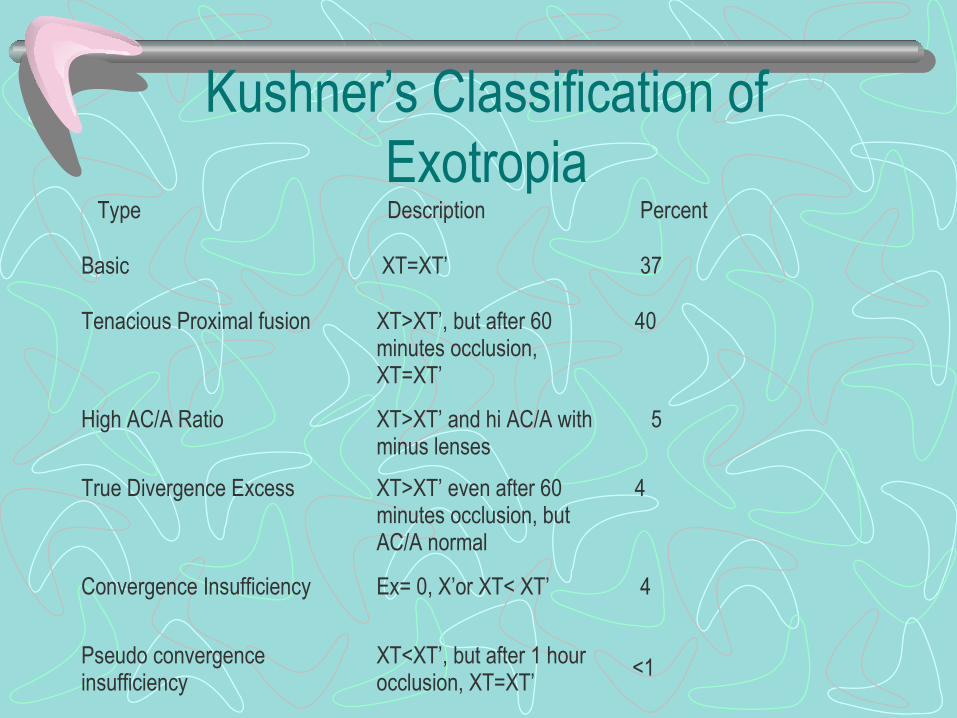
Kushner’s Classification of Exotropia
Type Description Percent
Basic XT=XT’ 37
Tenacious Proximal fusion XT>XT’, but after 60 minutes occlusion, XT=XT’
40
High AC/A Ratio XT>XT’ and hi AC/A with minus lenses
5
True Divergence Excess XT>XT’ even after 60 minutes occlusion, but AC/A normal
4
Convergence Insufficiency Ex= 0, X’or XT< XT’ 4
Pseudo convergence insufficiency
XT<XT’, but after 1 hour occlusion, XT=XT’
<1

Non Surgical Treatment of Exotropia
1. Maximize vision– Glasses especially for myopia– Treat amblyopia
1. Minus lenses2. Base in prism with or without minus lenses3. Orthoptics
• Mainly useful for convergence insufficiency with Ex=0, X’ or X(T)’
5. Part time patching: may improve control

Prisms for Exotropia
• Base In Prisms useful in– Small angle exotropia– For reading with convergence insufficiency
• Base out Prisms:– Temporary treatment of esotropia after exotropia
surgery

Non Surgical Treatment of XT
• 7 y/o: VA OD 20/80, OS 20/80• X (T) = 30• Refraction: OD –1.50 20/20• OS –1.50 20/20• Rx: glasses• Six weeks later Ex=0 with glasses
Surgical Treatment of Exotropia
• Rarely if ever improves (4% in one study)• Natural course
– Neonatal exotropia often improves spontaneously– Some infantile exotropia remains intermittent– Other cases become constant exotropia– Most progress to some degree
Surgical Treatment of Exotropia
• Maximize vision first• Phase 0: X, no XT
– No treatment needed
Surgical Treatment of Exotropia
• Phase 1: X(T), Ex’=0• Watch if:
– Infrequent deviation– No symptoms: peers or patient
• Operate if:– Deviation frequent– Progressive deviation– Symptomatic
Surgical Treatment of Exotropia
• Phase 2: XT at distance, X’ or X(T)’ near– Surgery recommended without delay– Patient in danger of losing binocular vision
• Phase 3: XT far, XT’ near– Surgery for social reasons if desired– Small chance of improving binocularity

Surgery for Exotropia
• Children under age 5– 18 diopters or less: can recess one lateral rectus– Over 20 diopters: recess LR OU but use 2/3 amount
of adult “numbers”– High chance of overcorrection with recession LR OU
if use regular adult numbers for surgery in young children
Surgery for Exotropia
• Usually recess LR OU as initial operation• Convergence insufficiency with XT distance less
than XT at near:– Recess one LR, Resect one MR
• Poor vision in one eye– Recess LR, Resect/Tuck MR of eye with reduced
vision

Surgery for Exotropia• Beware of surgery for high AC/A ratio
– Surgery for distance deviation likely to cause esotropia and diplopia at near
• If prolonged cover testing reveals no deviation at near: patch one eye 60 minutes– If XT or X appears at near less than XT at distance: recess
LR OU– If no deviation at near after patching: measure AC/A ratio at
distance with minus lenses• If high AC/A ratio: prescribe minus lenses• Can do recession LR OU with posterior fixation MR OU

Exotropia: Clinical Examples
1. 2 y/o X(T) = 30, X’=18
2. 6 month old XT=XT’=55
3. 6 y/o VA OD 20/20, OS 20/200• CR: OD + 0.25, OS –6.00• LXT = 25

Exotropia: Clinical Examples
4. 12 y/o XT= 30. Surgery for ET age 3
5. 23 y/o medical student– Eyes tired with reading– Ex=0, X(T)= 15
Surgical Treatment of Exotropia
• Basic Exotropia XT=XT’– May be treated with Recess LR OU or
recess one LR, resect/tuck one MR– Various studies show different results, some
advocate one operation over the other– Most surgeons currently use recess LR OU

Surgical Treatment of Exotropia
• Desired position of eyes one week post op is:– LR recession OU over age 5: ET 4-10 diopters– Eyes become more exo in the weeks following
surgery– High recurrence rate if XT undercorrected at age one
week– With Recession one LR, desire smaller E after
surgery (2-6 diopters)