Embed Size (px)
Citation preview
Cyrena De RamosSt. Cloud State UniversityNovember 12, 2014
• Understand data supporting the significance of VTE prophylaxis for medical patients
• Recognize 3 core measures related to VTE prophylaxis
• Understand correct use and contraindications for pharmaceutical VTE prophylaxis
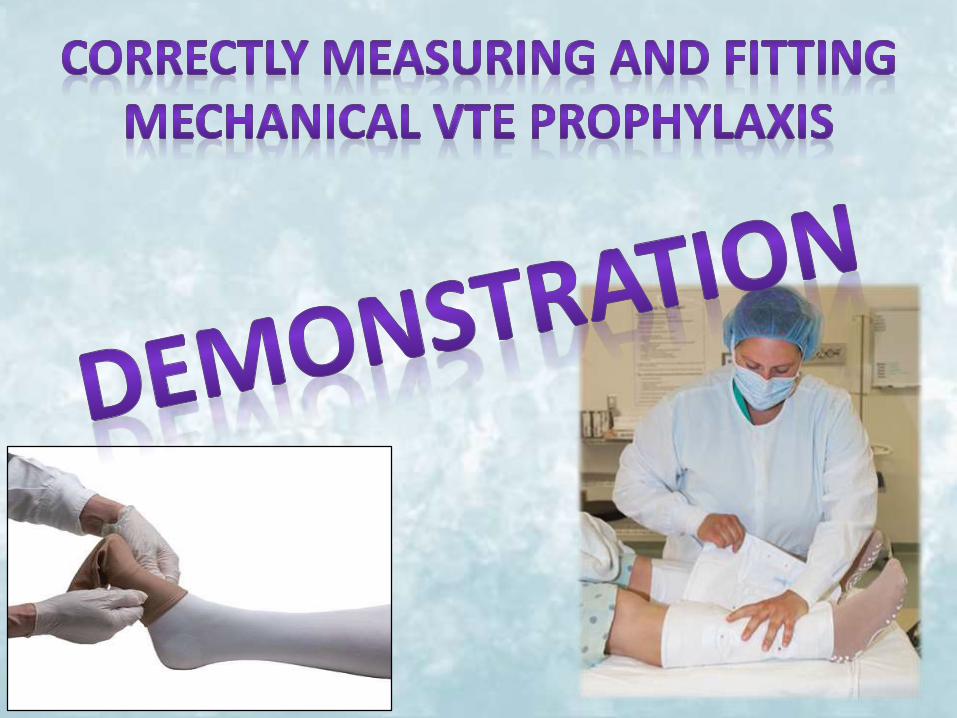
• Understand correct use, fit, and contraindications for mechanical VTE prophylaxis
• Identify various ways to improve patient compliance/use of VTE prophylaxis
• VTE comprising pulmonary embolism(PE) and deep vein thrombosis (DVT), accounts for 5% -10% of all deaths among hospitalized patients
• DVTs affect as many as 600,000 patients annually• PEs are recognized as the most common cause of
preventable hospital deaths and account for up to 200,000 deaths annually.
• 10% to 20% of medical patients acquire DVTs• Only 40% of at-risk medical patients receive
guideline recommended VTE prophylaxis
• 60% of DVTs and 50% of PEs could be avoided with proper use of VTE prophylaxis
• 100,000 lives could be saved annually with proper use of VTE prophylaxis
• 360,000 individuals would avoid the negative consequences of DVTs
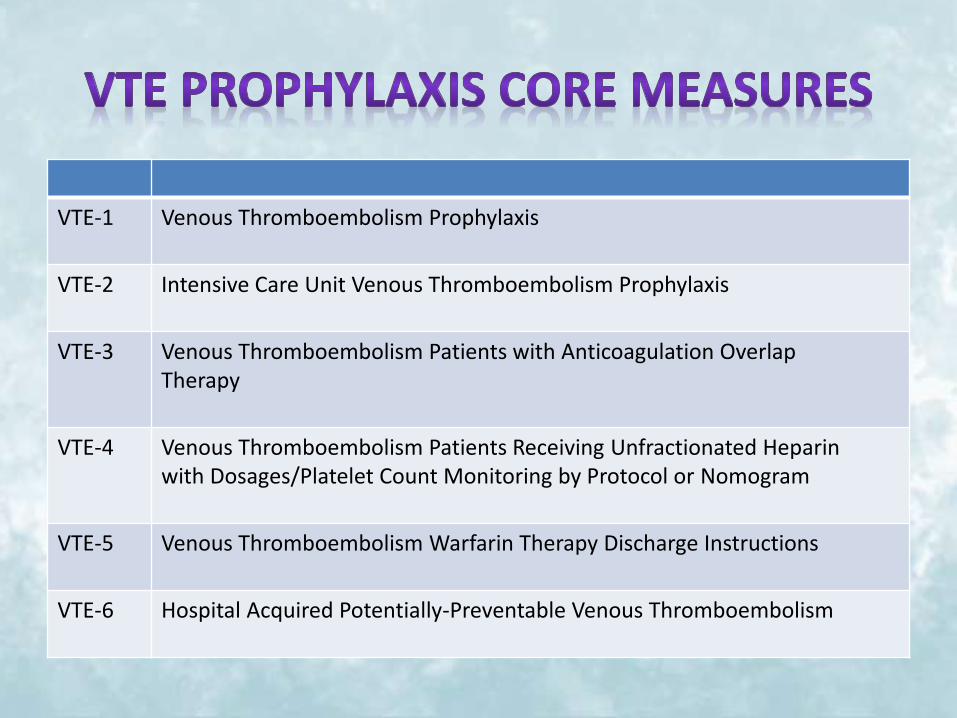
VTE-1 Venous Thromboembolism Prophylaxis
VTE-2 Intensive Care Unit Venous Thromboembolism Prophylaxis
VTE-3 Venous Thromboembolism Patients with Anticoagulation Overlap Therapy
VTE-4 Venous Thromboembolism Patients Receiving Unfractionated Heparin with Dosages/Platelet Count Monitoring by Protocol or Nomogram
VTE-5 Venous Thromboembolism Warfarin Therapy Discharge Instructions
VTE-6 Hospital Acquired Potentially-Preventable Venous Thromboembolism
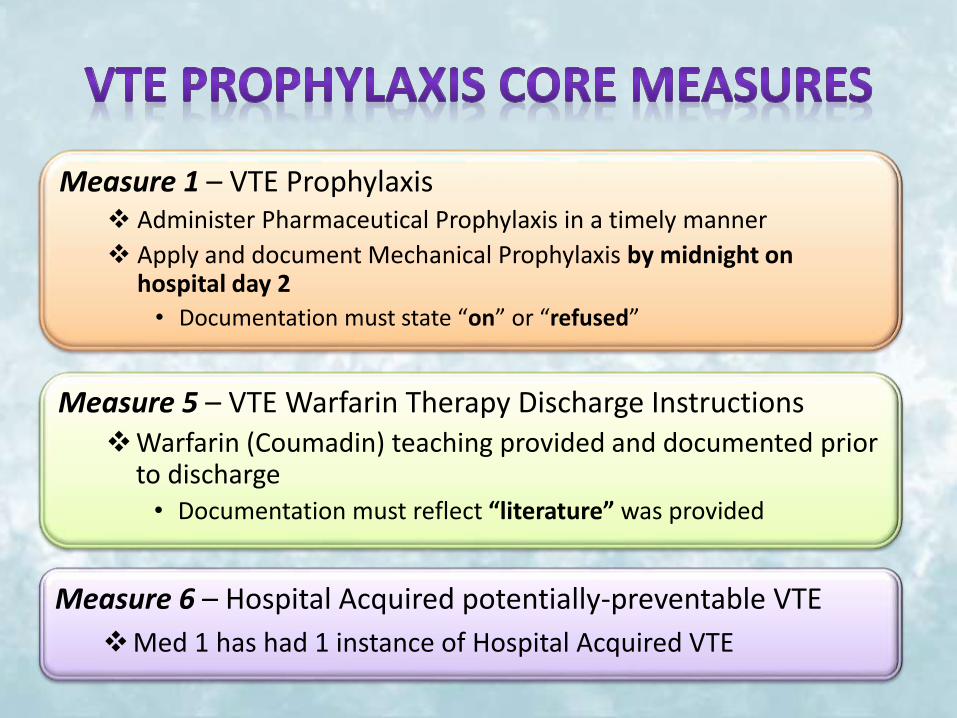
Measure 1 – VTE Prophylaxis Administer Pharmaceutical Prophylaxis in a timely manner
Apply and document Mechanical Prophylaxis by midnight on hospital day 2
• Documentation must state “on” or “refused”
Measure 5 – VTE Warfarin Therapy Discharge InstructionsWarfarin (Coumadin) teaching provided and documented prior
to discharge• Documentation must reflect “literature” was provided
Measure 6 – Hospital Acquired potentially-preventable VTE
Med 1 has had 1 instance of Hospital Acquired VTE
• Pharmacologic prophylaxis should include heparin or a related product– LMWH such as Enoxaparin (Lovenox)– Warfarin (Coumadin)
• Preferred method of VTE prophylaxis when not contraindicated
• Pharmacologic prophylaxis is more effective than mechanical prophylaxis
• Implemented unless the risk for bleeding outweighs the expected benefit
• Continue throughout course of hospitalization, including at discharge
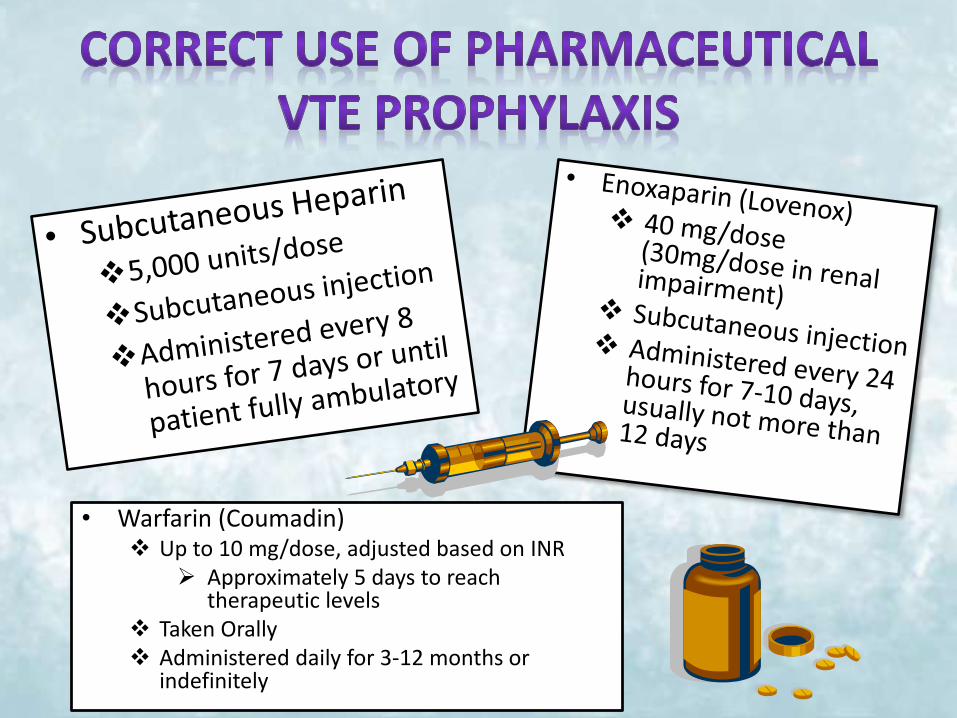
• Warfarin (Coumadin) Up to 10 mg/dose, adjusted based on INR
Approximately 5 days to reach therapeutic levels
Taken Orally Administered daily for 3-12 months or
indefinitely
• Active Bleeding• High-risk uncontrolled hemorrhage • Bleeding disorders, Thrombocytopenia, and/or
Conditions in which bleeding would be catastrophic• Renal dysfunction• Liver disease with Coagulopathy• Hypersensitivity to Heparin or LMWH• INR > 1.5• Spinal Tap or Epidural Anesthesia• Intracranial and/or Intraocular Surgery within 6 weeks• Major Trauma/Closed Head Injury/Intracranial Bleed• Uncontrolled Hypertension (SBP>200 mmHg, DBP> 110
mmHg)
• Mechanical VTE prophylaxis includes: – Thromboembolism-Deterrent Hose (TEDs)/ACE Wraps– Intermittent Pneumatic Compression Devices (IPCDs)– Foot Impulse Devices (FIDs)
• For patients unable to receive pharmacological VTE prophylaxis, or in conjunction with pharmacologic VTE prophylaxis
• Use as IPCDs and FIDs as much of the time as is possible and practical, both when in bed and when sitting in a chair
• TEDs should be worn day and night until the patient no longer has significantly reduced mobility (TEDs generally last about 3 months)
• Continue to use mechanical VTE throughout the hospital stay, frequent ambulation is not a substitute
• Ensure patients have their legs measured and the correct size is provided• Re-measure legs in patients who develop edema or postoperative swelling• Remove TEDs twice daily for 30 minutes for hygiene and to skin inspection
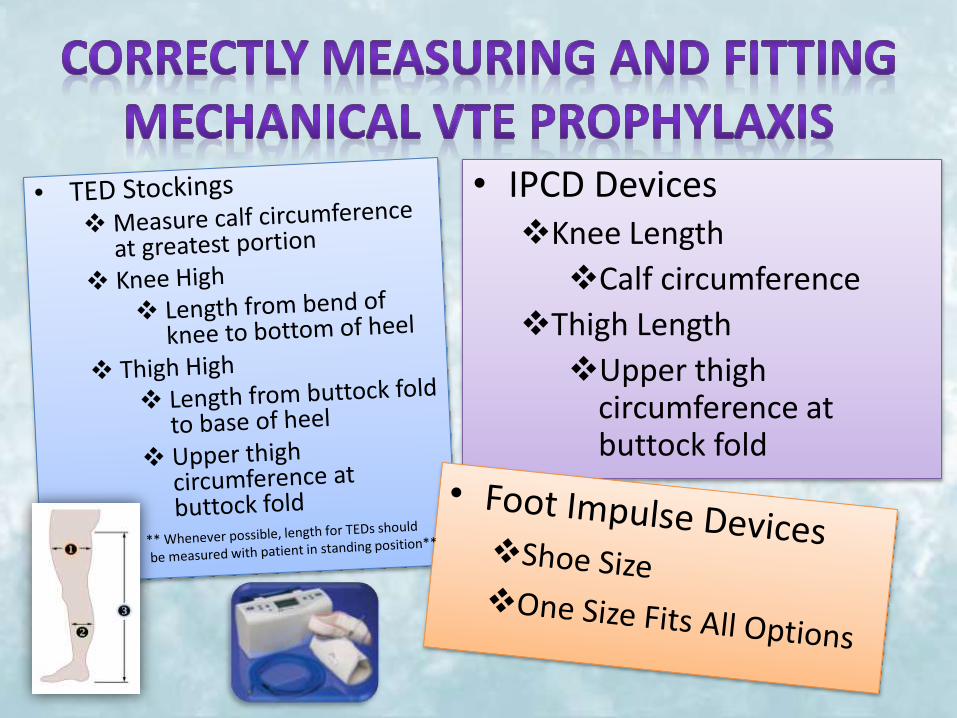
• IPCD DevicesKnee Length
Calf circumference
Thigh Length
Upper thighcircumference at buttock fold
Do not use TEDs on patients who have: Peripheral arterial bypass grafting Peripheral neuropathy or other causes of sensory impairment Any local conditions in which stockings may cause damage, for example
fragile 'tissue paper' skin, dermatitis, gangrene or recent skin graft Cardiac failure Severe leg edema or pulmonary edema from congestive heart failure Unusual leg size or shape Major limb deformity preventing correct fit.
• Use caution and clinical judgment when applying TEDs over venous ulcers or wounds.
• If arterial disease is suspected, seek expert opinion before TEDs• Stop using TEDS if there is marking, blistering, or discoloration of the
skin, or if the patient experiences pain or discomfort; may request order for FIDs or IPCDs
Do not use IPCDS on patients who have:
Any local leg condition in which the sleeves may interfere, such as: dermatitis, vein ligation [immediate postoperative] gangrene, recent skin graft.
Severe arteriosclerosis or other ischemic vascular disease. Massive edema of the legs or pulmonary edema from congestive heart
failure Extreme deformity of the leg Suspected pre-existing deep venous thrombosis
Do not use FIDs on patients who have: Conditions where an increase of fluid to the heart may be detrimental Congestive Heart Failure Pre-existing deep vein thrombosis, thrombophlebitis or pulmonary
embolism
Provide clear and comprehensive patient education on VTE, health risks, and benefits to VTEo Include literature for the patient to reviewo Explain the patient’s individual risk factors
Investigate the reason for refusalo Brainstorm ideas with the patient to overcome barriers and implement
prophylaxis
Provide a consistent messageo All members of the healthcare team must provide the patient with similar
reliable information regarding the importance of VTE prophylaxis, including consistent use of prophylaxis
Be a patient advocateo If a patient refuses one method of VTE prophylaxis, ask the physician if they
would like to order an alternative method (Ex. Patient refuses Heparin but is willing to use IPCD)
Be persistent!o Continue to reinforce the education and ask the patient on a regular basis if
they would like to begin using VTE prophylaxis
Lorraine is a 68-year-old woman with a past medical history of coronary artery disease (CAD) (s/p MI x 2, coronary artery bypass graft [CABG 8 years ago), hyperlipidemia, hypertension, and heart failure. She is admitted with a 1-week history of fatigue, shortness of breath at rest, and a 15-pound weight gain over the last week. She is diagnosed with acute decompensatedheart failure and diuretic therapy is initiated.
Mimi is a 73-year-old woman admitted to the medical unit with pneumonia. She has been hospitalized frequently over the last 2 months for a brain tumor, which was removed 5 weeks ago. She has been very weak since the surgery and can only pivot transfer.

Anderson, F. & Audet, A. M. (2010). Preventing deep vein thrombosis and pulmonary embolism. Retrieved from https://www.outcomes-umassmed.org/DVT/best_practice/index.htm#Section1
Bozarth, A. L., Bajaj, N., & Abdeljalil, A. (2013). A Review of venous thromboembolism prophylaxis for hospitalized medical patients. Hospital Practice, 41(3), 60-69. doi: 10.3810/hp.2013.08.1069
Camden, R. & Ludwig, S. (2014). Prophylaxis against venous thromboembolism in hospitalized medically ill patients: Update and practical approach. American Journal of Health-System Pharmacy, 71(11), 909-917. doi: 10.2146/ajhp130475
Covidien. (2010). A-V impulse foot compression system. Retrieved from http://www.covidien.com/imageServer.aspx/doc233675.pdf?contentID=28688&contenttype=application/pdf
Covidien. (2013). Kendall SCD 700 series controller. Retrieved from http://www.covidien.com/imageServer.aspx/doc233674.pdf?contentID=42968&contenttype=application/pdf
Dentali, F., Douketis, J. D., Gianni, M., Lim, W., & Crowther, M. A. (2007). Meta-analysis: Anticoagulant prophylaxis to prevent symptomatic venous thromboembolism in hospitalized medical patients. Anals of Internal Medicine, 146(4), 278-288.
Elpern, E., Killeen, K., Patel, G., & Senecal, P. A. (2013). The application of intermittent pneumatic compression devices for thromboprophylaxis. American Journal of Nursing, 113(4), 30-36.
Haut, E. R., & Lau, B. D. (2013). Prevention of venous thromboembolism: Brief update review. Retrieved from http://www.ncbi.nlm.nih.gov/books/NBK133363/pdf/TOC.pdf
King, C. S., Holley, A. B., Jackson, J. L., Shorr, A. F., & Moores, L. K. (2007).Twice versus three times daily heparin dosing for thromboembolism prophylaxis in the general medical population: A metaanalysis. Chest, 131(2), 507-516. doi:10.1378/chest.06-1861
Laryea, J. & Champagne, B. (2013). Venous thromboembolism prophylaxis. Clinics in Colon and Rectal Surgery, 26(03), 153–159. doi: 10.1055/s-0033-1351130
National Institute for Health and Care Excellence. (2010). Venous thromboembolism: Reducing the risk of venous thromboembolism (deep vein thrombosis and pulmonary embolism) in patients admitted to hospital. NICE Clinical Guideline. Retrieved from http://www.nice.org.uk/guidance/cg92/resources/guidance-venous-thromboembolism-reducing-the-risk-pdf
Piazza, G., Nguyen, T., Morrison, R., Cios, D., Hohlfelder, B., Fanikos J., Paterno, M., . . . Goldhaber, S. (2012). Patient education program for venous thromboembolism prevention in hospitalized patients. American Journal of Medicine, 125(3), 258-264. doi: 10.1016/j.amjmed.2011.09.012.
The Joint Commission. (2014). Core measure sets: Venous thromboembolism. Retrieved from http://www.jointcommission.org/core_measure_sets.aspx