Embed Size (px)
Citation preview

Vision Training
Bikash Sapkota
B. Optometry
BPKLCOS, IOM
Nepal

Contents• Vision Training
oOverview
oMisconception
oTips for success
• Office Vision Training
• Home Vision Training
• Conditions treated by vision training
• Sports Vision Training
• Controversy
• Summary

Vision Therapy
• Also called vision training, orthoptics, eye training, and eye exercises
• Clinical approach for correcting the effects of eye movement disorders, nonstrabismic binocular dysfunctions, accommodative disorders, strabismus, amblyopia, nystagmus, and certain visual perceptual (information processing) disorders
• Entails a variety of non-surgical therapeutic procedures designed to modify different aspects of visual function

Vision Therapy
• The “specific controlled visual tasks” are accomplished by using a wide variety of instruments and methods
• Specific instruments and methodology are described as “vision-training techniques”
• Includes multiple subskills or procedures
• Subskills represent sequential steps
• Pt’s visual dysfunction determines “the sequential plan”

Passive Therapy
Pt. experiences a change in visual stimulation without any
conscious effort
Active Therapy
Designed to improve visual performance by the pt.’s conscious
involvement in a sequence of a specific, controlled visual task
that provide feedback

Vision Training
• Vision training is active therapy as it requires conscious participation by the pt.
• It asks the pt. to use mental effort ( Giles 1947) to learn a specific visual response when performing a specific procedure
• Some method of identifying correct from incorrect responses (Biofeedback) should be incorporated into each training procedure (Forrest 1981; Letourneau 1976)

Vision Training
• Pt. is taught to obtain a correct response and then to repeat it until the response goes from a conscious effort to an unconscious reflexive level (Giles 1947)
• When a reflexive response is achieved, improved visual performance will transfer to other noncontrolled visual tasks (Consweet and Crane 1973)
• And ultimately will change the underlying visual processing mechanisms (Liu et al. 1979, North and Hensen 1982)

Vision Training
• The integrity of the sensory and motor systems underlies the final results of any mode of treatment
• VT attempts to reach the sensory and motor potentials by involving the active efforts of the pt. to maximize visual performance during each procedure
• The selection of suitable VT procedures for each pt. is essential and should not be a prearranged nonspecific program

Vision Training
• Successful vision training depends on three important elements:
1. An accurate diagnosis of the pt.’s visual problems
2. A careful selection of visual procedures to best remediate the problems
3. A collection of visual procedures that will facilitate the transfer of the learned visual skills to the pt.’s own visual world

Vision Training
• The achievement of the final goal occurs progressively, as correct responses from controlled tasks are transferred to noncontrolled tasks
• The underlying neuropsychophysiological mechanisms affected by vision training are still under intense investigation,
- and it is hoped that they will be clarified in future studies

Misconceptions about Vision Training
1. VT Improves the strength of the EOM Change the neurophysiological vergence-control
mechanism (Schor 1983) through repetition of specific visual stimulation
2. VT eliminates the need for lenses or surgical therapy VT is not a substitute
VT is an additional treatment

Overview of vision training
• Most procedures use separate targets for each eye
• Separation is accomplished by:
- Septum
- Mirrors
- Anaglyphic and vectographic systems
- Chiastopic/ orthopic techniques

Overview of vision training
• Polaroid or anaglyph reduce sensory stimulation by acting
as partial filters
- but they provide the advantage of apparently open
environment or open-space viewing (Vodnoy 1972)
• Septum and mirror allow viewing of targets without filters
- but introduce an artificial split field and often stimulate
proximal convergence

Tips for Successful Vison Training Program
• Prescribe incrementally
• Adapted to the individual patient
• Progress at the patient’s own rate
• Maintain the patient’s interest
• Use 2-4 therapy techniques or procedures per week

Office Vision Training (OVT)
Each OVT session usually consists of 3 parts
• First, pt.’s activities from the previous week are reviewed, in order to assess performance and progress
• Pt. is asked to demonstrate to the therapist how he/ she did the technique
• In this way, the therapist can ascertain whether the training was performed correctly and as prescribed

Office Vision Training (OVT)
• Second, the OVT is carried out, emphasizing techniques and procedures that cannot be done at home
• The OVT will enhance pt.’s performance on the techniques that will be prescribed for home vision training (HVT)

Office Vision Training (OVT)
• Third, changes in the HVT program are discussed, and any new techniques to be prescribed for HVT are taught
• Be ensure that pt. is capable of adequately performing the assigned procedures before leaving the office
• Both verbal and written instructions should be given to pt. (and to the parent, if the pt. is a child)

Home Vision Training (HVT)
• HVT is an integral part of the total treatment program for many pts.
• When properly controlled and administered, HVT significantly contributes to the success of the overall vision training program
• As an adjunct to OVT, it provides the continuity that is absent in an active therapy program managed entirely in the office

Home Vision Training (HVT)
• Parental involvement is necessary for HVT if the pt. is a child
• HVT is rarely successful when the parent is not emotionally or intellectually capable of administering the prescribed procedure
• HVT failures are more often due to a parent’s inability to deal with the family dynamics and stress created during active therapy than due to the inadequacies of the prescribed at-home training techniques (Shiva 1971)

Advantages of HVT
• Provides regular practice periods, which are necessary for correct responses to eventually become reflexive in nature
• Enables pts. to make progress on their own
• Results in a reduction in the frequency and total number of office visits
• Maintains the pt.’s interest

Educational Principles Underlying Vision Training (Spivey 1970)
• Better accomplished in an active rather than a passive manner
• Individualized process that occurs at different rates and in different ways for different pts.
• Accomplished more easily when it is meaningful and relevant to the pt.
• Goals should be realistic and achievable so that the pt. does not become discouraged

Educational Principles Underlying Vision Training
• Best accomplished when the pt. is provided with feedback so that he/she can monitor his/her own performance
- This feedback should be positive and rewarding,
not negative or punishing
• Facilitated in the presence of pleasant surroundings and good interpersonal relationships

Suggestions for Scheduling Vision Training
• Daily therapy for a short time is preferable to weekly therapy for longer time periods
• Total training time of 30 to 60 mins performed in one or multiple sessions per day is prescribed
• No. of daily sessions is dependent upon the pt.’s age, attention span, and time availability
• Although multiple daily sessions provide the best results, compliance may be best when one daily session is prescribed

Suggestions for Scheduling Vision Training
• For young children (3 to 7 yrs old), 2 to 4 daily sessions, each lasting 10 to 20 mins, are spread over the day
• Infants and toddlers are prescribed 4 to 6 daily sessions, each lasting 3 to 10 mins
• When HVT is possible and good results are anticipated, OVT can be prescribed on a once-per-week basis
• When HVT cannot be performed, a minimal schedule of 2 to 3 times per week of OVT is recommended

Suggestions for Training Patients of Different Ages
• Techniques that require strict visual attention and a steady body posture should be alternated with gamelike activities
• Short break when a child is losing interest or motivation
• Competitive games and a reward system can be used to increase motivation, concentration, and compliance

• Young children require short period of training, with frequent changes in activity or targets
• Attractive and interesting target help to hold the child’s interest
- Bright colors
- Moving objects
- Musical accompaniment
- Flashing lights
Suggestions for Training Patients of Different Ages

Role of Behavior Modification in Vision Training
• Important component of VT program for children (Feldman 1981; Granger and Letourneau 1977; Groffman 1969; Punnett and Steinhauer 1984)
• Take care to reward children for “looking carefully” and for “hard work” not for providing the correct answer
• Avoid saying “good” after a child responds or a procedure is completed, because it implies that the responses were correct

Role of Behavior Modification in Vision Training
• Saying “good looking” instead leaves the emphasis on good behavior rather than the child’s responses
• Always ask open-ended questions such as, “How many do you see?” rather than, “Do you see one?”

Conditions Treated by Vision Training
Strabismic and non-strabismic binocular dysfunctions
Ambylopia
Accommodative dysfunctions
Ocular motor dysfunctions
Visual motor disorders
Visual perceptual (visual information processing) disorders

Accommodative Therapy
• Directed towards improving accommodative amplitude, facility, sustaining ability, reducing response time
• Accommodative demand is altered by the use of plus or minus lenses or change in fixation distances
• Done monocularly and binocularly

Accommodative Therapy
Traditional Therapy
Hart Chart
Lens flippers
Loose minus lens rock
Split pupil rock
Brockstring Exercise
Computer Vision Therapy

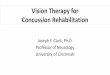
Hart Chart Rock Exercise
• Consists of two cardboard charts each with a block of 100 (10 rows of 10 letters each) black letters printed on white background
• Larger HC is used for distance fixation, smaller HC for near fixation
• Uses change in fixation distances
• Can increase AA, facility or both
- HC push up for AA training
- Altering fixation as facility therapy
Fig: Hart chart for accommodative rock

Lens Flippers
• Plus/minus lenses to produce rapid changes in the accommodative demand
• Choose lens flippers of equal dioptric powers(+/-0.50D to 2.00 DS)
• Flippers held directly in front of pt.’s eyes at the spectacle plane
• Begin with minus lenses, then plus side, make the letters clear within 1-2 secs without fatigue and discomfort

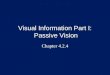
Binocular Accommodative Facility
• A red/green bar reader and red/green glasses are used along with age-appropriate reading material with about 20/30 size
• The bar reader is placed on top of the reading material
• Flip lenses are held before the pt.'s eyes, and is instructed to clear the print
• The pt. reads one line of print, and the flip lenses are flipped to the other side
• Can also be performed using any fusional vergence therapy procedure such as vectograms, tranaglyphs, the Aperture Rule
Fig: Binocular accommodative
facility using a bar reader
Fig: Aperture Rule used for binocular
accommodative facility

Loose Minus Lens Rock
• Loose minus lens, interposed directly in front of open eye to read the print
• If letters become blur, try to make it clear
• As soon as letters are clear, interpose minus lens and make letters clear within 1-2 seconds without fatigue and discomfort
• Start from -0.50 D
Fig: Loose lens rock procedure

Split Pupil Rock
• Loose minus lens held below the open eye and slowly moved upwards so that the top edge of lens bisects the pupil with monocular diplopia of target
• Images are separated vertically, top image appear larger than bottom
• See the top image and make it clear, shift gaze to bottom image and again make it clear within 1-2 seconds

Computer Vision Therapy
• Can improve vergence, accommodative, and oculomotor problems
• Most programs are set up to record pt.’s performance each session
oRemoves the problem of compliance
• Different products on the market
oHome Therapy System
oComputer Aided Vision Therapy
oPsychological Software Services

Computer Vision Therapy
• Pts. can use at home, work, wherever they have access to computer
• Trains eye movements, vergences, accommodation, and perceptual skills
• A study showed an improvement on tests of cognitive skills with computer vision therapy1
1- A study of the effectiveness of cognitive therapy delivered in a video game format. Helms D, Sawtelle SM. Optom Vis Dev 2007

Fusional Vergence Therapy
• Anaglyphs, Polaroids, and liquid Crystal Filters
Variable Tranaglyphs
Variable Vectograms
Nonvariable Tranaglyphs
Computerized Binocular Vision Therapy Procedures
• Lenses, Prisms, and Mirrors
Flip Prism or Loose Prism
• Septa and Apertures
Aperture Rule
Modified Remy Separator

• Paper, Pencil, and Miscellaneous Tasks
Eccentric Circles
Free Space Fusion Cards
Lifesaver Cards
• Stereoscopes
Brewster Stereoscopes
Cheiroscope
Wheatstone Stereoscope
• Voluntary Convergence Procedures
Brock String
Barrel Card/3-Dot Card
Fusional Vergence Therapy
Objectives of fusional vergence procedures Increase the amplitude of negative fusional vergence (NFV)
and positive fusional vergence (PFV) Decrease the latency of the fusional vergence response lncrease the velocity of the fusional vergence response

Anaglyphs, Polaroids, and Liquid Crystal Filters
Variable Tranaglyph
Fig: Peripheral tranaglyph targets
Fig: Peripheral tranaglyph target. Moving the
green slide to the left and the red slide to the
right creates a convergence-type demand

Fig: Variable vectograms Fig: Vortex vectogram Fig: Baseball vectogram.
Fig: Central tranaglyph targets Fig: Non variable Tranaglyph

Office Based Computer Vision Therapy
Computer Orthoptics VTS4 Liquid Crystal System
Fig. A: Child working with the Computer Orthoptics Random Dot Stereopsis program.
B: Patient's view of the Computer Orthoptics Random Dot Stereopsis target.

Lenses, Prisms and Mirrors:
Flip Prism or Loose Prism
• The objective is to supplement other fusional vergence therapy techniques such as such as tranaglyphs, vectograms, the Aperture Rule, and Eccentric or Free Space Circles
• For example, if a pt. is working with a Quoit vectogram doing convergence therapy and finds the task very easy, additional BO prism could be used to increase the level of difficulty of the task
• Alternatively, BI prism could be used to decrease the difficulty of the task

Septa and AperturesAperture Rule
A: Single Aperture- the visual axes cross at a distance closer than the viewed targets, creating a chiastopic or BO fusion demandB: Double Aperture- the visual axes cross at a distance farther away than the viewed targets, creating an orthopic or BI fusion demand

Aperture Rule
• Fusion occurs through chiastopic (base-out) or orthopic(base-in) fusion
• Consists of a rulerlike apparatus, two plastic slides-one with a single aperture and the other with a double aperture and 12 cards with varying disparities, ranging from 2.5 to 30 Δ
Fig: Location of the plane of accommodation and convergence
during convergence therapy using the Aperture Rule.

Fig: Aperture Rule for convergence therapy
Fig. A: Right-eye view of Aperture Rule card
B: Left-eye view of Aperture Rule card
C: View of Aperture Rule card with both eyes

Paper, Pencil and Miscellaneous TasksEccentric circles, Free Space Fusion Cards A and Lifesaver Cards
Fig: Eccentric Circles setup for convergence
therapy, illustrating planes of accommodation
and vergence
Fig. A: Pt.’s perception of Eccentric Circles setup
with the "As" during chiastopic fusion.The outer
rings appear to be floating closer.
B: Pt.'s perception of Eccentric Circles setup
with the "As" during orthopic fusion. The inner
rings appear to be floating closer.
Appearance When Fusing Base-Out
Appearance When Fusing Base-In

Lifesaver Cards and Free Space Fusion Cards B
Fig: Lifesaver and
Free Space Fusion Cards BFig: New Lifesaver Cards

Modified Remy Separator
• It is used for divergence therapy
• Useful for home therapy
• If the pt. experiences any difficulty, plus lenses are helpful to get started
• Discontinue this technique when the pt. can achieve fusion with a divergence demand of about 15 base-in
Fig: Modified Remy separator
using a septum and Lifesaver card

StereoscopesBrewster Stereoscope
• Designed to separate the fields of the two eyes using a septum
• Optical system consists of + 5.00 D spheres
• Optical centers are usually separated by 95 mm, which induces BO prism because the separation is wider than the average pt.'s IPD
• Stereoscope targets can be placed at varying distances
• Can be used to vary both the accommodative demand and convergence demand
Fig: Bernell-0-Scope. Fig: Sample stereograms. A: Base-out
Bioptograms. B: Keystone cards AN 9 and
AN 77.

Accommodative Demand
• Because the power of the stereoscope lenses is known and the distance of the target from the lens plane is known, one can easily calculate the accommodative demand, using the following formula:
A= (l/TD)- P
Where, A= accommodation (D)
TD = distance between target and lens plane (m)
P = power of stereoscope lenses (D)

Examples
• You are working with a stereoscope with +5.00 D lenses and a 95 mm lens separation. If you place the stereoscopic card at 20 cm, what is the accommodative demand?
Answer
A= (l/TD)- P A = (l/0.2) - 5 A=5-5=0
- At a working distance of 20 cm, there is no accommodative demand. This is the distance setting for this particular stereoscope.
• If the target is now moved to a working distance of 13 cm, what is the accommodative demand?
Answer
A= (l/TD)- P A = (1/0.13) - 5 = 7.6 - 5 = 2.6 D
- At a working distance of 13 cm, the accommodative demand is about 2.6 D.

Convergence Demand
• C = (P X LS)- (TS/TD)
where
C = vergence demand in prism diopters
P = power of stereoscope lenses
LS = separation of optical centers of stereoscope lenses (cm)
TD = distance of stereogram from stereoscope lenses (m)
TS = separation of corresponding points of the stereogram (cm)

Examples
• You are working with a stereoscope with +5.00 D lenses and a 95 mm lens separation. What is the vergence demand for a 60 mm target set at 20 cm?
Answer
C = (P X LS)- (TS!ID) C = (5 X 9.5) - (6.0/0.2) = 47.5- 30 = 17.5 BO
• If you use the same stereoscope as in above example and the same card, now set at a working distance of l3 cm, what is the vergence demand?
Answer
C = (P X LS)- (TS!ID) C = 47.5 - (6.0/0.13) = 47.5 - 46.0 = 1.5 BO

Cheiroscope
Fig: Keystone Correct-Eye Scope setup
for cheiroscopic tracing.
Fig: Cheiroscopic tracing forms
Fig: Illustration of drifting during cheiroscopic tracing.

Wheatstone Stereoscope
Fig: Variable Prismatic Stereoscope
Fig: Patient working with Variable Prismatic
Stereoscope

Voluntary Convergence Procedures
Brock String Employs the principle of physiological diplopia
Objectives
- Develop the kinesthetic awareness of converging
and diverging
- Develop the ability to voluntarily converge
- Normalize the near point of convergence

Procedures
1. Recognition of physiological diplopia
2. Jumps, two brads at near, and introduction of fixation accuracy
3. Jumps, three beads at near
4. Jumps, far to near
5. Jumps, three beads (near, intermediate, far)
6. Push-ups and push-aways
7. Bug on a string

Fig. A: Patient working with Brock string.
B: Patient's perception when looking at the near, or
C: far bead when using the Brock string.

Barrel Card/ 3-dot Card
Fig: Patient working with Barrel Card Fig: Patient working with Albee 3-Dot Card

• Vergence therapy resulted in some improvement in both objective findings and symptoms for some subjects. (The effectiveness of pencil pushups treatment for convergence insufficiency: a pilot study. Gallaway M et al, Optom Vis Sci 2002 Apr)
• Office-based vergence accommodative therapy is an effective treatment for children with symptomatic convergence insufficiency. (Randomized clinical trial of treatments for symptomatic convergence insufficiency in children. Convergence Insufficiency Treatment Trial Study Group, Arch Ophthalmol. 2008 Oct)

Antisuppression Procedures
• Cheiroscope
• Bar Reader
• TV Trainer
• Red/Green Glasses and Penlight
• Vertical Prism Dissociation
• Mirror Superimposition
• Computer Home Therapy Procedures Home Therapy System
• Computer Aided Vision Therapy: Computer Vergences Program-Random Dot Stereo grams

TV Trainer
• Sheet of plastic with one side all green and the other side all red
• Attached to the TV, and the pt. wear red/green glasses
• Eye behind the red filter sees through the red side of the TV trainer, while eye behind the green filter sees through the green side
• If one eye suppression-one side of the TV trainer will turn black
Fig. A: TV trainer. B: TV trainer positioned on TV

• Pt. holds a small mirror at a 45-degree angle in front of one eye and views a target through the mirror
• With the other eye, views another target
• Pt. must try to superimpose one image on top of the other
Mirror Superimposition
Fig: First-degree targets used with
mirror superimposition
Fig: Second-degree target used with
mirror superimposition

Vision Training for Amblyopia
• Pleoptics
• Near activities
• Active stimulation therapy using CAM vision stimulator
• Syntonic phototherapy
• Role of perceptual learning
• Binocular stimulation
• Software-based active treatments
• Exposure to dark

Ocular Motility Procedures
• Loose Prism jumps
• Hart Chart: Saccadic Therapy
• Letter and Symbol Tracking
• Visual Tracing
• Rotator Type Instruments
• Flashlight Tag
• Computer Software/Advanced Technology Procedures
• Afterimage Technique

Loose prism jump
• While the pt. views a target monocularly, a prism is placed before the fixating eye
• Prism displaces the image of the fixation object off the fovea and a saccade will be necessary to regain foveal fixation
• Must be able to quickly and accurately regain fixation
• Important goal is to be sensitive to very small amounts of prism

Hart Chart: Saccadic Therapy
• Place the Hart chart about 5 to 10 ft from the pt.
• Occlude the pt.'s left eye with an eye patch
• Instruct pt. to call out the first letter in column 1 and then the first letter in column 10,
- the second letter from the top in column 1 and the second
letter from the top in column 10 and so on

Letter and Symbol Tracking
• Occlude pt.'s one eye
• Tell the patient to begin at the upper right and scan from left to right to find the first letter "a"
• Ask the patient to then find the very first "b," cross it out, and continue through the entire paragraph
• The goal is to complete this task as quickly as possible
Fig: Symbol tracking workbook
ABC DE FGH tJKLM N OPQRSTUVWXYZ
a bcdefghijklmnopqrstuvwxyz
lin chako evi nomd zeby thipg nare.
Zuth pirm nuroc dif stok. Nileg myt
lolf. Tixs nom reus zab tuin lugah.
Marb sewt rotsir puje. Yonak nesud
voz alee. Xart chod bugm turh sref
tree gen foru. Vab reps tique kowj.
Dagh meulb fwer ilg side. Ubc they
bouf yed neoph vaik. Wolen kig peab
nod tenc xerb. Rait rebey fal zibtMin. Sec .
Fig: Letter tracking workbook

Visual Tracing
• Contains tracing tasks that gradually increase in level of difficulty from the beginning to the end of the book
• Occlude one of the pt.'s eyes and ask the pt. to place the pen on the letter "A" and to trace along the line until the end of the line
• As the pt.'s accuracy and speed improve, the next level of difficulty can be added
Fig: Visual tracing workbook

Rotator-Type Instruments
• Occlude pt.’s one eye
• Instruct the pt. to place a golf tee into a hole in the pegboard
• The holes on the innermost part of the rotating pegboard are the easiest to work with, and the outer holes are the most difficult
• To combine saccadic eye movements with pursuit eye movements, a pattern can be drawn to follow on a wall directly behind the rotating pegboard
Fig: Rotating pegboard (concentric circles are
different colors: red, yellow, and blue)Fig: Automatic rotator

Afterimages
• Any photographic flash device with narrow slit can be used to create afterimages
• Occlude pt.’s one eye
• Instruct pt. to fixate at the center of the vertical slit on the flash unit
• Activate the flash unit and, after the flash, ask the pt. to blink rapidly or flicker the lights in the room
• Can enhance any ocular motor technique such as Hart chart saccadic technique and the automatic rotating device

Computer Software/ Advanced Technology Procedures
• Computer Orthoptics Liquid Crystal Automated Vision Therapy (VTS4)11
• Computer Perceptual Therapy (CPT)b
• Sanet Vision Integrator (SVI)
• Neurovision Rehabilitator (NVR)
• The Perceptual Visual Tracking Program (PVT)
Fig: Sanet Vision Integrator-Saccadic
procedure
Fig: Sanet Vision Integrator-Pursuit
procedure

Therapy for Heterophoria
Exercises for Esophoria
1. Divergence exercises with prisms• Prisms of increasing strength are placed base-in before one
eye while he/she is fixating an object at a distance
• Loose prisms, a prism bar or rotating (Risley) prisms may be used: prism bar is preferred
• Performed for a few mins. at each
weekly visit

2. Divergence Exercise on Synoptophore
• Performed on synoptophore using stereopsis slides, because they provide the strongest stimulus to fusion
• After fusing 2 pictures, pt. is trained to maintain a single vision (by relaxing convergence) while the instrument tubes are diverged
• Should be performed for about 5 mins.
at each weekly visit

3. Physiologic Diplopia Exercises using Stereograms in the Crossed Position
• While pt. is fixating a distance object, the stereogram card is held about 25 cm in front of eyes
• Pt. will perceive 4 pictures (due to crossed physiological diplopia)
• He/ she is trained to adjust its position until the 2 central pictures are fused and pt. perceives 3 pictures
• Pt. is trained to maintain the joined pictures and to see it clearly
• Pt. can practice at home for few
mins. several times a day

4. Exercise using diploscope
5. Exercise using Remy separator
6. Reading bar exercise

Exercises for Exophoria
• The aim is to improve the fusional convergence (relative position convergence)
1. Convergence exercise with prisms• Similar to that described for esophoria, except that in it, prisms
are placed base-out in front of the eyes
• Watch the pt.’s eyes to make certain that he/ she is converging and has not diverged and suppressed

2. Convergence exercise using synoptophore• Performed as described for esophoria, except that in it, the
instrument arms are slowly converged, beginning at an angle at which pt. can fuse the picture
3. Physiologic diplopia exercise using stereogram
in the uncrossed position
4. Convergence exercise using diploscope

Vision Therapy after Acquired Brain Injury
• A number of investigators have described treatment of binocular vision, accommodative, and eye movement problems associated with ABI using vision therapy (Brahm KD 2009, Ciuffreda kJ 2008, and others)
• Vision therapy is an excellent option when the pt. has adequate cognitive, memory, and attention skills
• Recent studies concluded that the majority of participants who completed the study experienced meaningful improvements in signs and symptoms
(Conrad JS et al Optom Vis Sci. 2017 Jan)
(Gallaway M et al 2017 Jan)

Sports Vision Training
• Works on improving the visual abilities of an athlete that are most necessary for excellence in their sport
• The visual skills necessary for peak athletic performance in many sports are:
Dynamic visual acuity
Focusing skills (Accommodation)
Tracking
Saccadic eye movement
Fixation Binocularity Depth perception

Sports Vision Training
Visual recognition and reaction time
Visual concentration
Peripheral awareness
Central-peripheral integration
Eye-hand-body coordination
Visual memory
Visualization
• Specific Sports VT program is assigned for specific type of sports. E.g peripheral vision enhancement training for team sports
Good peripheral vision is needed to keep
an eye on other players during team sports

• In a study, the claim that sports vision training can enhance visual skills and the level of sporting performance was investigated
• There was no evidence for VT improving either visual or motor performance(Joanne et al, Efficacy of Sports Vision Training Programs, Optom and
vis science 1997 )
• Another study suggested that certain visual abilities,e.g. the peripheral perception or the choice reaction time are trainable and can be improved by means of an appropriate VT. An automatic improvement of othervisual abilities could not be verified(Sebastian et al, The impact of a sports VT Program in youth field
hockey players, J of Sports sci and med 2012)

Controversy
• The U.K. College of Optometrists noted the “Continued absence of rigorous scientific evidence to support behavioral management approaches” in the second college of Optometrists report {Judith Warner (10 March 2010). “Concocting a Cure for Kids With Issues”.}

Controversy
• In 2009 The American Academy of Pediatrics reviewed 35 years of the literature in support of vision therapy and issued a stern warning about the seductions of treatments: “Ineffective, controversial methods of treatment such as vision therapy may give parents and teachers a false sense of security that a child’s learning difficulties are being addressed, may waste family and/or school resources and may delay proper instruction or remediation.” {Judith Warner (10 March 2010). “Concocting a Cure for Kids With Issues”.}

Controversy
• The website by the American Association for Pediatric Ophthalmology and Strabismus states: “Behavioral vision therapy is considered to be scientifically unproven” and “There is no evidence that vision therapy delays the progression or leads to correction of myopia.” (“Vision Therapy — AAPOS”. Aapos.org. Retrieved 2013-02-15.)
• Some physicians are skeptical about the efficacy of “vision therapy” stating that it lacks data and is mostly anecdotal (Jo Seltzer (30 Nov 2010). “Ophthalmologists express skepticism about vision therapy”. St. Louis Beacon.)

Summary
• Vision training is active therapy as it requires conscious participation by the pt.
• The achievement of the final goal occurs slowly and progressively
• VT is not a substitute to lenses or surgical therapy, it is an additional treatment
• Variety of BSV related conditions can be treated with VT
• The underlying neuropsychophysiological mechanisms affected by VT are still under intense investigation
• VT is the most controversial subject in eyecare profession

References