Embed Size (px)
Citation preview

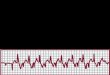
VENTRICULAR TACHYCARDIA
Dr. Y. Sridhar M.D.Consultant Intensivist
Dept. of Critical Care MedicineApollo Health City, Hyderabad

Definition• Wide complex rhythm QRS>0.12s
• Rate > 100 (or120) bpm
• Origin: from one of the Ventricles i.e., distal to the bundle of His.
• Three or more consecutive beats on a ECG.


Classification
• Duration of Episodes
• Morphology
• Symptoms

1.Duration of Episodes• Three or More beats on an ECG at a rate
>100bpm originating from Ventricles
• Non Sustained VT : If rhythm self-terminates
spontaneously in less than 30seconds
• Sustained VT : If rhythm lasts > 30seconds
(Even if it self-terminates spontaneously after
30s)

2.Morphology
• Monomorphic VT : same configuration beat to beat.
• Polymorphic VT : Continually changing QRS morphology
• Sinusoidal VT :sinusoidal appearance of rhythm
• Accelerated idioventricular rhythm (AIVR)

Monomorphic VT
• Most common cause : circuit through a region of old MI.
• Idiopathic VT (less common) No identifiable cause.
• Right Ventricular outflow tract (RVOT) tachycardia: MC Idiopathic VT
LBBB Morphology with inferior axis.


Polymorphic VTCauses• Active cardiac Ischemia• Electrolyte Disturbances• Drug Toxicity• FamilialTorsade de pointes (twisting of points)• Waxing and waning QRS amplitude during
tachycardia associated with prolonged QT interval


• Sinusoidal VT: seen in severe electrolyte disturbances • Hyperkalemia• Hypocalcemia• Hypomagnesemia
• AIVR» Wide complex ventricular rhythm at a rate of 40-
120bpm» Usually hemodynamically stable» MC cause :reperfusion arrhytmia in first 12hrs after
acute MI or during periods of elevated sympathetic tone.
» Typically preceded by sinus slowing» No treatment necessary. Self terminates.


Pathophysiology• Monomorphic VT :
• Increased automaticity of a single point in
either left or right ventricle
• Reentry circuit within the ventricle
• Polymorphic VT :
• Abnormalities in ventricular muscle
repolarization

Etiology• Structural Heart Disease : MI, Cardiomyopathies
(HCM), Myocarditis• Electrolyte Abnormalities : Hypokalemia,
Hyperkalemia, Hypocalcemia, Hypomagnesemia• Sympathomimetic agents : Ionotropes.• Drug toxicity : Digitalis, Methamphetamine, Cocaine• Systemic diseases : Sarcoidosis, RA, SLE.• Structural Congenital Disorders : Right ventricular
dysplasia, TOF

EtiologyProlonged QT Interval• Acquired :
• K Channel blocking medication : Quinidine, Erythromycin, Clarithromycin,Haloperidol, Droperidol
• Type 1A antiarrythmics : sotalol, amiodarone,
• Congenital : • Brugada syndrome• Congenital long and short QT syndromes• Catecholamingeric polymorphic VT

Diagnosis• “All WCT is VT until proven otherwise”• AV dissociaton : Dissociation of P wave from QRS
complex.• QRS Concordance : Absence of rS or Rs complex in any
precordial lead• RS > 100ms• Capture beats : Supraventricular beat conducts to
ventricle depolarising ahead of the next tachycardia beat• Fusion beats : Depolarisation simultanously with
excitation from a ventricular focus.





BRUGAGADA CRITERIA


Ultra simple Brugada Criteria
• In 2010 Joseph Brugada published simplified criteria
• Measuring R wave peak time (RWPT) in Lead Ⅱ• RWPT > 50ms• It measures duration of onset of QRS to first
change in polarity


Differential Diagnosis
• SVT with aberrant intraventricular conduction
• Preexcited Tachycardia (associated with or
mediated by accessory pathway)
• BBB
• Ventricular paced rhythms

Symptoms• Chest Pain• Light headedness• Palpitations• Syncope• Sudden Cardiac Death (SCD) :
• Ambulatory ECG records at SCD have shown 50-60% at sustained monomorphic VT as the initial event.

Treatment
Depends on Hemodynamics• Unstable VT
• Stable VT

ACLS Cardiac Arrest Algorithm.
Neumar R W et al. Circulation 2010;122:S729-S767
Copyright © American Heart Association

Stable VT
• Anti arrhythmic drug (AAD) therapy
• Implantable Cardioverter-Defibrillator (ICD)
• Catheter Ablation Therapy (CAT)
• Antiarrhythmic surgery

Tachycardia Algorithm.
Neumar R W et al. Circulation 2010;122:S729-S767
Copyright © American Heart Association



AMIODARONE• Large volume of distribution & long half life• Contraindications
• Iodine sensitivity• Sinus bradycardia• Heart block
• Precautions• Incompatible with NS• Preferable via CVC
• Adverse effects– Short term : Skin reactions,Brady, hypotension, corneal
microdeposits.

AMIODARONE– Long term :
• Pulmonary fibrosis, alveolitis, pneumonitis• Liver dysfunction..monitor LFT• Hypo or Hyperthyroidism (check TFT before
starting)• Peripheral neuropathy, myopathy, Cerebellar
dysfunction.• Concomitant Beta and Calcium channel
Blockers: Increased risk of bradycardia, AV Block
• Potentiates effect of Digoxin, Theophylline and Warfarin– Reduce dose

Implantable cardioverter-defibrillator (ICD)
• ICD therapy compared with conventional AAD associated with mortality reduction of 23-55% depending on risk group.
• Current ICD options:– Single chamber – Dual chamber – Biventricular cardiac resynchronization– Multilevel shock discharge for VT or VF
Complications: Inappropriate shock discharge
Defibrillator stormInfectionsExacerbation of HF

External Defibrillator
• Automated external Defibrillator
• Wearable automatic defibrillator– Worn under the clothing– Delivers shock whenever VF is detected.

• Procedure targets origin of VT• Useful in recurrent VT or “VT storm”.• Catheter is placed into heart chambers through femoral
vein• Radiofrequency energy is applied which produces a
small burn of about 4 to 5mm in diameter• Currently recommended in early treatment of VT when
AAD are not preferred or tolerated.


Figure 2. Mapping of VT. A 3-dimensional real-time map of the ventricle (created during the procedure) merged with a computed tomography scan (obtained before the procedure).
Tung R et al. Circulation 2010;122:e389-e391
Copyright © American Heart Association

Recurrent VT : Long term Management
• Risk of recurrence after successful resuscitation : 30-40%
• Management of Intercurrent diseases• Implantable Cardioverter Defibrillator• Long term therapy on Amiodarone.


Antiarrhythmic surgery
• Surgical resection of arrhythmogenic focus• Cardiac Sympathectomy• Aneurysm resection

Thank you!



















![Ventricular Tachycardia in the Ischemic Heart[1]](https://img.pdfslide.us/doc/110x75/55283aae49795921048b4677/ventricular-tachycardia-in-the-ischemic-heart1.jpg)








