Embed Size (px)
Citation preview

VENOUS DRAINAGE
OF HEAD AND
NECK
By:
Avneet K Soni
OMFS
1
•The venous system is a network of conduitsi.e. veins which transport deoxygenated bloodfrom tissues to the heart. Exceptions arethe pulmonary and umbilical veins, both ofwhich carry oxygenated blood to theheart. Equally important ,they serve as majorreservoirs of blood.• About 84% of entire blood volume of body isin systemic circulation and 16% in heart andlungs.• Of the 84 % in systemic circulation,64%is inveins,13%in arteries and 7% in systemicarterioles and capillaries
Introduction
2

Veins are classified as:Superficial veins are those whose course is close to the
surface of the body, and have no corresponding arteries.Deep veinsDeep veins are deeper in the body and have corresponding
arteries.Communicating veinsCommunicating veins (or perforator veins) are veins that
directly connect superficial veins to deep veins.Pulmonary veinsThe pulmonary veins are a set of veins that deliver oxygenated
blood from the lungs to the heart.Systemic veinsSystemic veins drain the tissues of the body and deliver
deoxygenated blood to the heart.
3
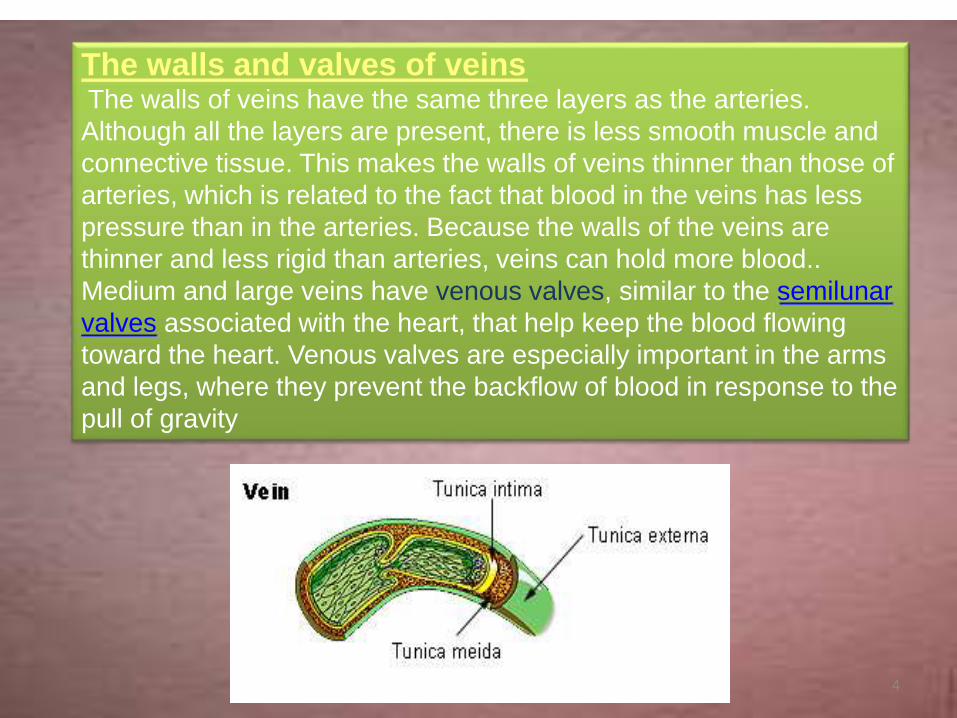
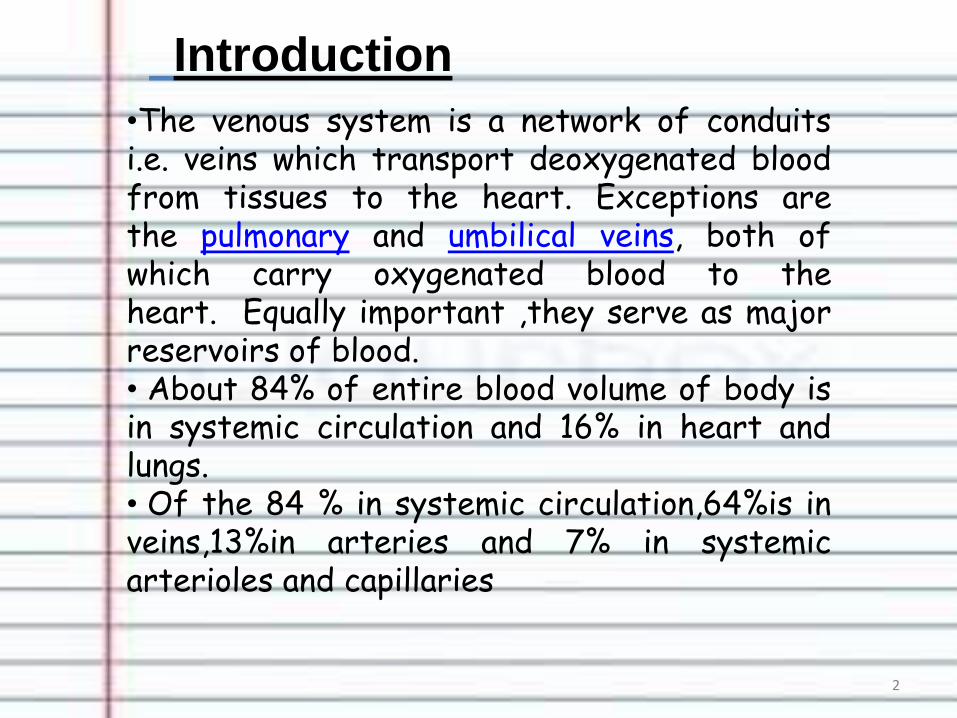
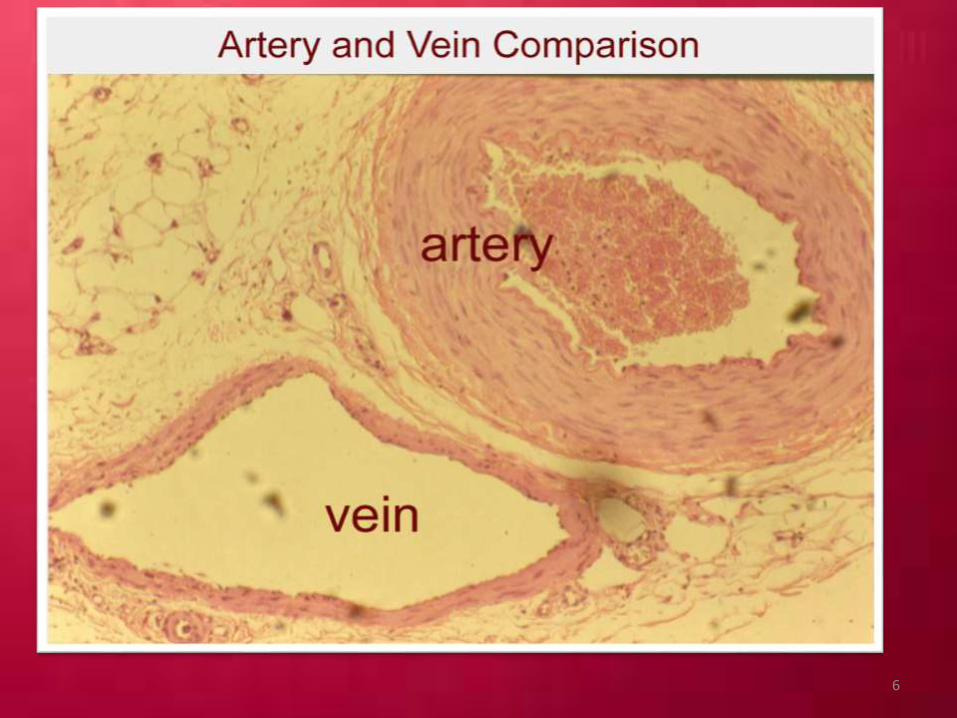
The walls and valves of veinsThe walls of veins have the same three layers as the arteries.
Although all the layers are present, there is less smooth muscle and
connective tissue. This makes the walls of veins thinner than those of
arteries, which is related to the fact that blood in the veins has less
pressure than in the arteries. Because the walls of the veins are
thinner and less rigid than arteries, veins can hold more blood..
Medium and large veins have venous valves, similar to the semilunar
valves associated with the heart, that help keep the blood flowing
toward the heart. Venous valves are especially important in the arms
and legs, where they prevent the backflow of blood in response to the
pull of gravity
4
Artery vs Vein
5
6

VENOUS SYSTEM ,HOW DOES IT WORK?
The venous system in the
body returns deoxygenatedblood from all parts of the body,including the organs, to the rightside of the heart, and then on tothe lungs, to be oxygenated.From the lungs, the oxygenatedblood passes to the left part ofthe heart, to be pumped to allthe tissues and organs of thebody.
7
• The venous system consists of large and small veins; the large veins tend to liealongside arteries. Veins are more thin-walled than arteries, they act as a reservoirfor blood, and about 60-70% of the body’s blood is in the venous system.
• Many veins have one-way valves to facilitate the flow of blood back to the heartagainst the force of gravity. This is especially applicable to the veins in the legs, andto a lesser extent, in the arms. The valves work in the same way as one- way swingdoors, the blood pushing the valves open as it travels toward the heart; the valvesclose as blood fills that part of the vein, and prevents backward flow.
• Though the legs have superficial veins (under the skin) and deep veins (in themuscles) which carry blood back to the heart, as well as connecting veins knownas “perforating veins” (which connect the superficial and deep veins), most of theblood is propelled back to the heart by the deep veins. Blood from the superficialveins mostly travels through the connecting veins to the deep veins and isreturned to the heart this way, this is also a one-way system, as the connectingveins have valves as well.
• The deep veins are surrounded by muscles enclosed in a fascial sheath. Walkingcompresses the veins and thrusts the blood back towards the heart.
• This is why exercise, especially walking, is so useful in preventing stasis of theblood in the legs, and consequently venous thrombosis.
• The one-way valves also help in this process of return of blood, as well as allowingthe deep veins to refill from the superficial veins.
8
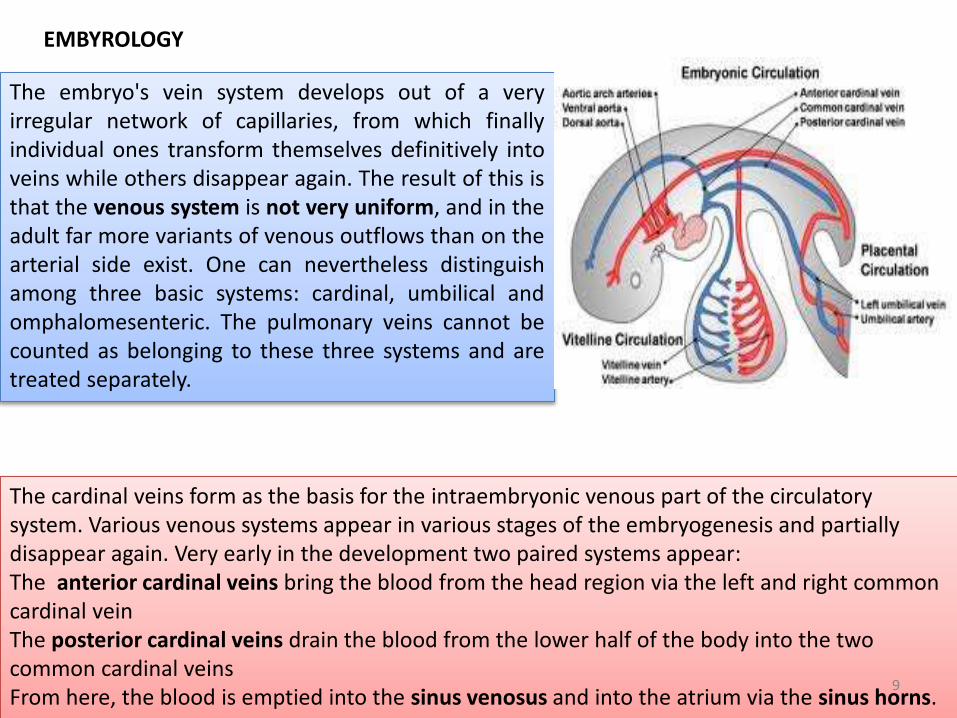
The embryo's vein system develops out of a veryirregular network of capillaries, from which finallyindividual ones transform themselves definitively intoveins while others disappear again. The result of this isthat the venous system is not very uniform, and in theadult far more variants of venous outflows than on thearterial side exist. One can nevertheless distinguishamong three basic systems: cardinal, umbilical andomphalomesenteric. The pulmonary veins cannot becounted as belonging to these three systems and aretreated separately.
The cardinal veins form as the basis for the intraembryonic venous part of the circulatory system. Various venous systems appear in various stages of the embryogenesis and partially disappear again. Very early in the development two paired systems appear:The anterior cardinal veins bring the blood from the head region via the left and right common cardinal veinThe posterior cardinal veins drain the blood from the lower half of the body into the two common cardinal veinsFrom here, the blood is emptied into the sinus venosus and into the atrium via the sinus horns.
EMBYROLOGY
9
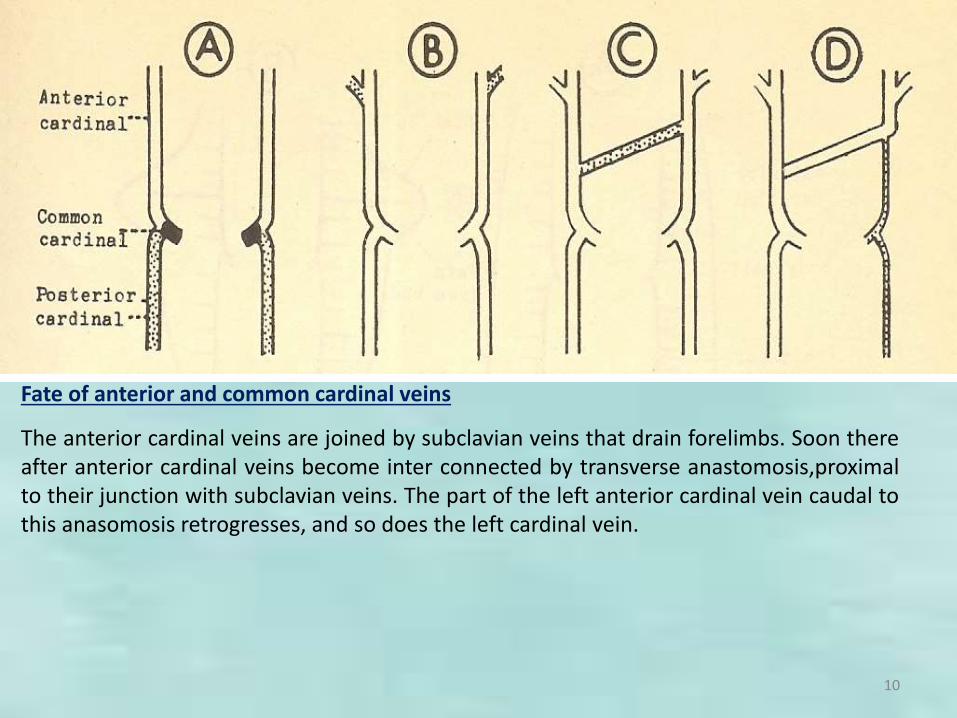
Fate of anterior and common cardinal veins
The anterior cardinal veins are joined by subclavian veins that drain forelimbs. Soon thereafter anterior cardinal veins become inter connected by transverse anastomosis,proximalto their junction with subclavian veins. The part of the left anterior cardinal vein caudal tothis anasomosis retrogresses, and so does the left cardinal vein.
10
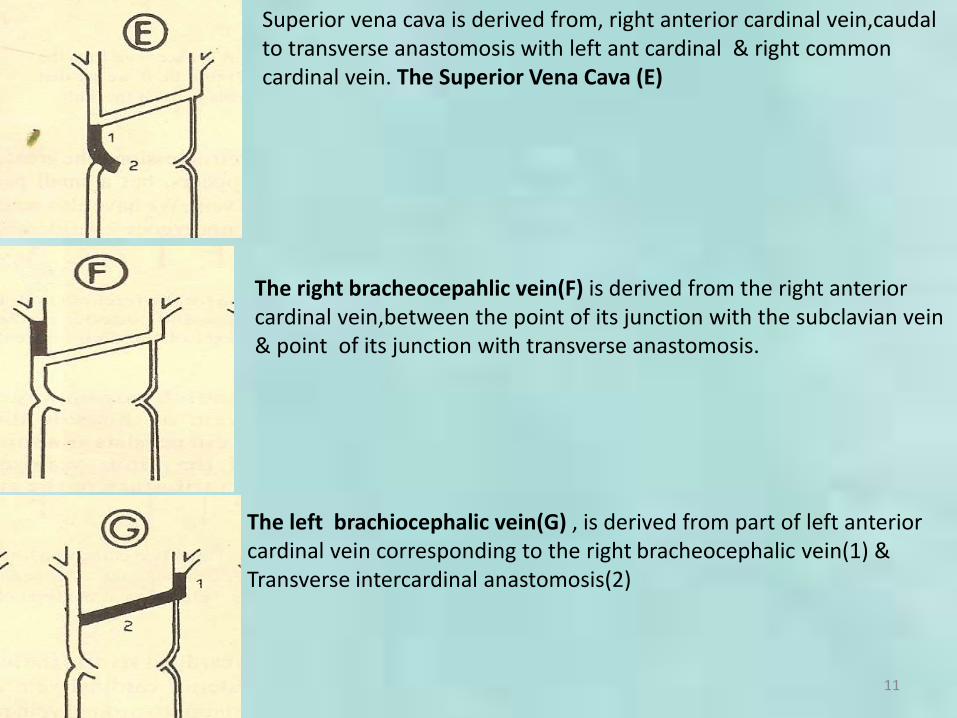
Superior vena cava is derived from, right anterior cardinal vein,caudalto transverse anastomosis with left ant cardinal & right common cardinal vein. The Superior Vena Cava (E)
The left brachiocephalic vein(G) , is derived from part of left anterior cardinal vein corresponding to the right bracheocephalic vein(1) &Transverse intercardinal anastomosis(2)
The right bracheocepahlic vein(F) is derived from the right anterior cardinal vein,between the point of its junction with the subclavian vein & point of its junction with transverse anastomosis.
11

The internal jugular veins (H) develop from the parts of the anterior cardinal veins cranial to their junction with subclavian veins
The external jugular veins arise as secondary channels and are not derived from anterior cardinal veins.
The caudal part of the anterior cardinal vein, and the whole of the common cardinal vein, for the
left side undergo retrogression. The greater part of the posterior cardinal vein of this side
disappears, but a small part adjoining the common cardinal vein persists as a small vein. Tthe
left horn of the sinus venosus undergoes considerable retrogression and is reduced to a
tributary of the right horn. These retrogressing veins of the left side persist into adult life as the
left superior intercostals vein and the coronary sinus.
12

Arteriovenous anastomoses are direct connections between smaller arteries and veins. Connecting vessels may be straight or coiled & often possses a thick muscular tunic. Simple arteriovenous anastomoses are widespread & occur notably in the skin of nose,lips,ears,nasal& alimentary mucosae,tongue,thyroid gland & sympathetic ganglia. In old age they atrophy ,sclerose and diminish in number & may contribute to less efficient temp. regulation.
13
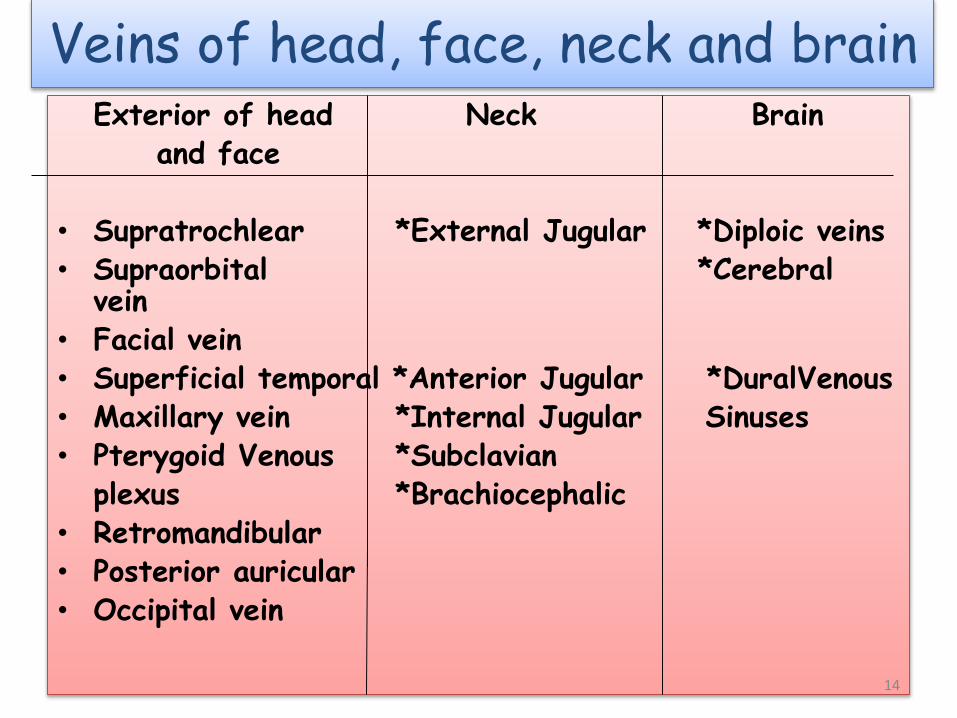
Veins of head, face, neck and brain Exterior of head Neck Brain
and face
• Supratrochlear *External Jugular *Diploic veins• Supraorbital *Cerebral
vein• Facial vein• Superficial temporal *Anterior Jugular *DuralVenous• Maxillary vein *Internal Jugular Sinuses• Pterygoid Venous *Subclavian
plexus *Brachiocephalic• Retromandibular• Posterior auricular• Occipital vein
14

Supra trochlear vein
Starts on the forehead from venous network which connects to the frontal tributaries of superficial temporal vein.
Joins supra-orbital vein to form facial vein near medial canthus.
15

Supraorbital vein
• begins on the forehead where it communicates with the frontal branch ofthe superficial temporal vein. It runs downward superficial to the Frontalismuscle, and joins the frontal vein at the medial angle of the orbit to formthe angular vein.Passes under orbicularis oculi. A branch passes throughsupraorbital notch to join superior ophthalmic vein .In notch it receivesveins from frontal sinus & frontal diploe.
16

Facial vein
• Coursing parallel to facial arteries arevalveless veins that provide theprimary superficial drainage of theface.
• Commences at the side on the root ofthe nose and
• Lies behind facial artery and is lesstortuous
• formed by the union of thesupraorbital and supratrochlear veinsat the medial canthus to form theangular vein
• Communicate with the cavernoussinus through the ophthalmic vein orvia the supraorbital vein.
17
Facial vein
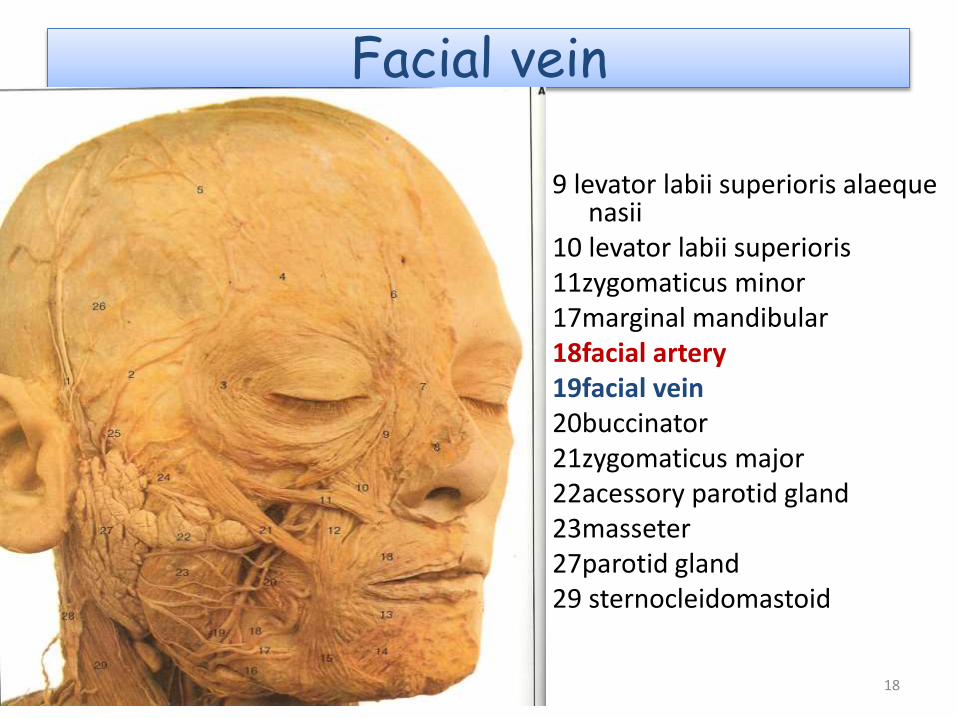
9 levator labii superioris alaequenasii
10 levator labii superioris11zygomaticus minor17marginal mandibular18facial artery19facial vein20buccinator21zygomaticus major22acessory parotid gland23masseter27parotid gland29 sternocleidomastoid
18
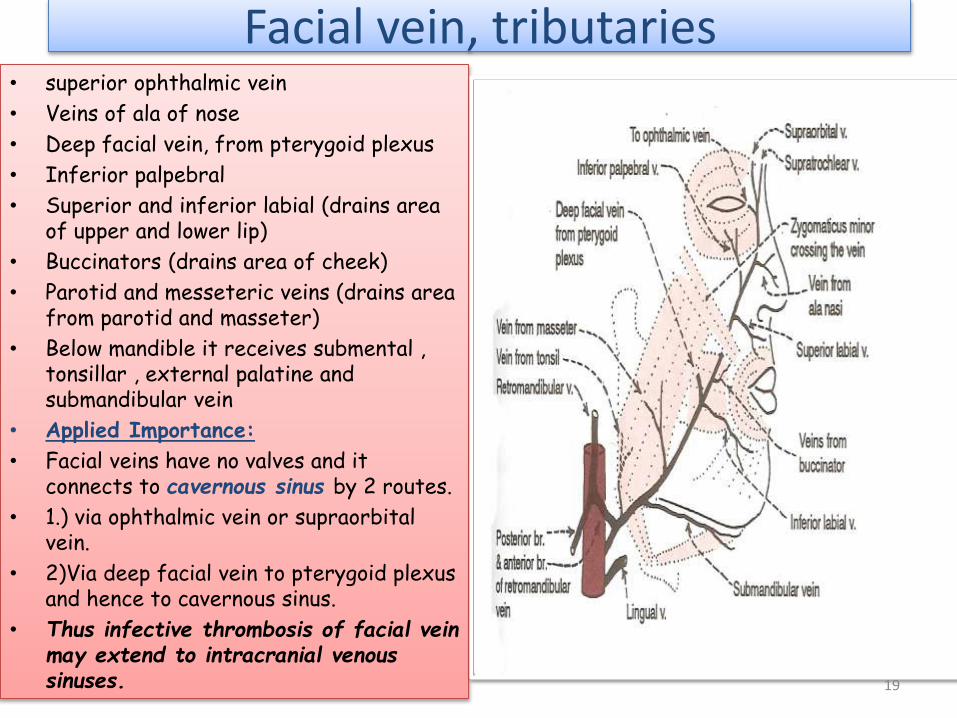
Facial vein, tributaries• superior ophthalmic vein
• Veins of ala of nose
• Deep facial vein, from pterygoid plexus
• Inferior palpebral
• Superior and inferior labial (drains area of upper and lower lip)
• Buccinators (drains area of cheek)
• Parotid and messeteric veins (drains area from parotid and masseter)
• Below mandible it receives submental , tonsillar , external palatine and submandibular vein
• Applied Importance:
• Facial veins have no valves and it connects to cavernous sinus by 2 routes.
• 1.) via ophthalmic vein or supraorbitalvein.
• 2)Via deep facial vein to pterygoid plexus and hence to cavernous sinus.
• Thus infective thrombosis of facial vein may extend to intracranial venous sinuses. 19

Superficial temporal
•Begins in a widespread network joined across scalp to contra-lateral vein and with supratrochlear, supraorbital, posterior auricular and occipital veins, all draining same network•cross posterior root of zygoma & enters parotid gland to unite with maxillary vein to form retromandibular vein.
20
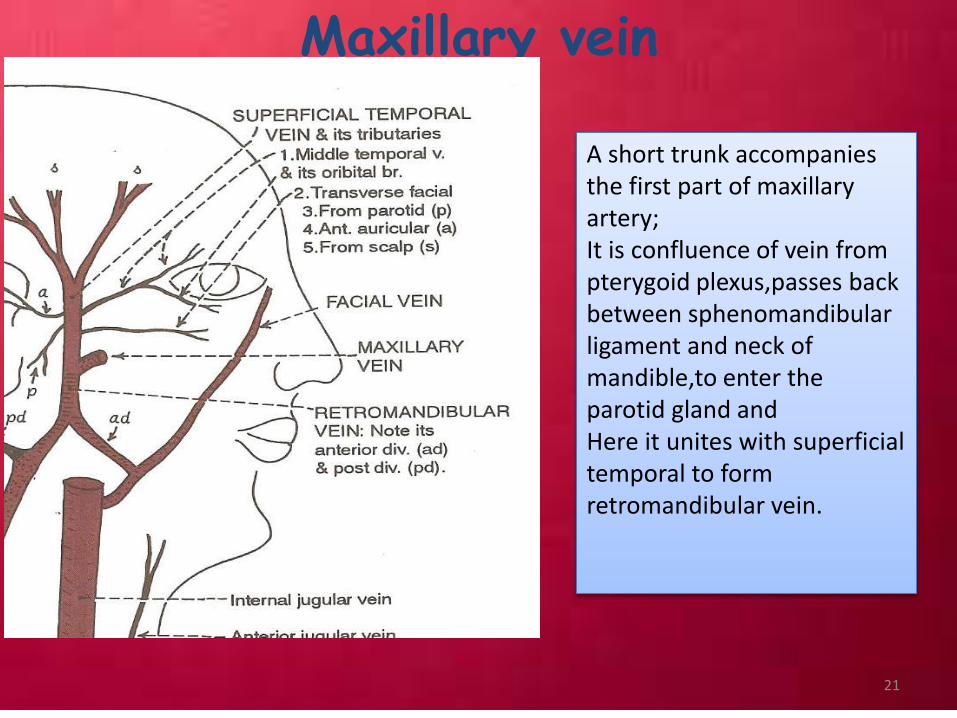
Maxillary vein
A short trunk accompanies the first part of maxillary artery;It is confluence of vein from pterygoid plexus,passes back between sphenomandibularligament and neck of mandible,to enter the parotid gland andHere it unites with superficial temporal to form retromandibular vein.
21

Retromandibular veinRuns posterior to ramus of the mandible within the substance of parotid glandSuperficial to external carotid artery and deep to facial nerveDivides into an anterior branch going forwards to join with facial vein andPosterior branch which joins posterior auricular to form external jugular vein
Knowledge of the normal anatomy of the extra-cranial FN and its relationship with the RMV isessential for surgeons dealing with parotid glands.Formation of the RMV by union of the superficialtemporal vein and maxillary vein mostly occurs ata level higher than the passage of the main trunkand branches of the FN, where they laterally passto the vein. In normal anatomical variation, therisk of bleeding from the RMV as a result of itsinjury is not high during parotid surgery. Incontrast, in cases of abnormal anatomicalvariation where RMV passes laterally to the FN orits branches, the risk of bleeding and nerve injuryduring parotid surgery is much higher.
22
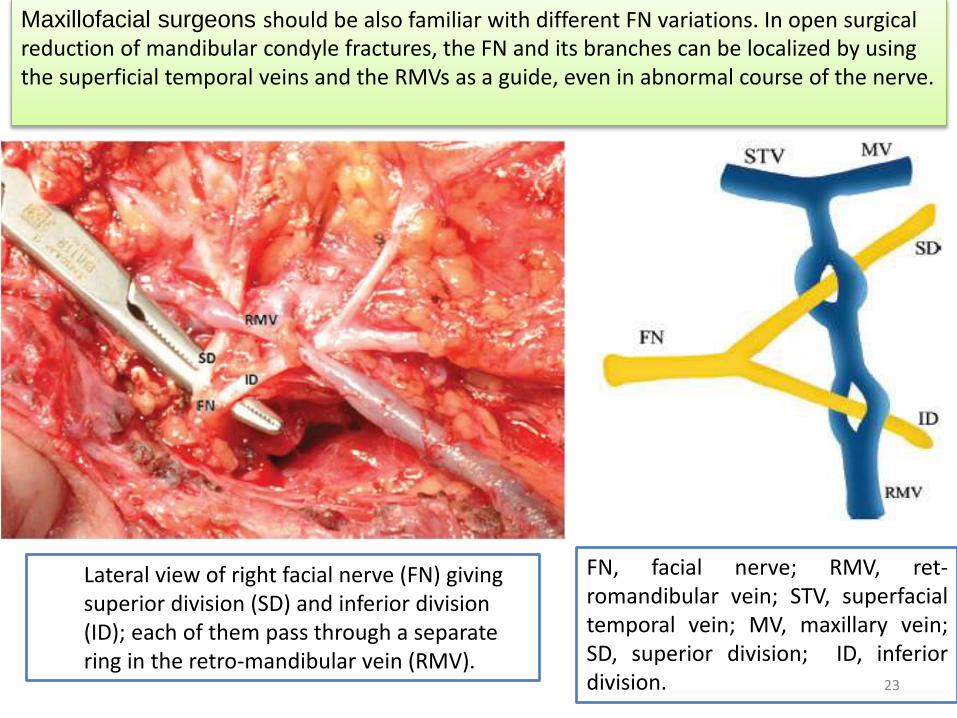
Lateral view of right facial nerve (FN) giving superior division (SD) and inferior division (ID); each of them pass through a separate ring in the retro-mandibular vein (RMV).
FN, facial nerve; RMV, ret-romandibular vein; STV, superfacialtemporal vein; MV, maxillary vein;SD, superior division; ID, inferiordivision.
Maxillofacial surgeons should be also familiar with different FN variations. In open surgical reduction of mandibular condyle fractures, the FN and its branches can be localized by using the superficial temporal veins and the RMVs as a guide, even in abnormal course of the nerve.
23

Posterior auricular
• Begins upon the side of neck,in a plexus which communicates with tributaries of occipital vein and temporal veins.
• Descends behind the auricula and joins the posterior division of retromandibular vein to form
external jugular vein.
• Applied: receives mastoid emissary veins from
sigmoid sinus. Infection here can be dangerous or fatal from retrograde thrombosis of cerebellar
and medullary veins.
24

Occipital vein
• Begins in posterior network in scalp, pierce the cranial attachment of trapezius, turns into suboccipital triangle and becomes deep.
• May follow occipital artery to end in internal jugular vein vein;
• Or join posterior auricular & hence external jugular vein.
25

26

Pterygoid venous plexus
Placed partly between temporalis and lateral pterygoid and partly between two pterygoids.Anteriorly reaches from the maxillary tuberosity and superiorly to the base of skullSphenopalatine,deep temporal, pterygoid, massetric, buccal, dental, greater palatine and middle meningeal veins and branches from inferior opthalmic veins are all tributaries.Connects with facial veins facial veins through deep facial veins & With cavernous sinus through veins that pass through sphenoidalemissary foramen, foramen ovale and lacerumIts deep tributaries are connected with middle meningeal vein.Applied : needle track communications can also result in infection to pterygoid plexus. PSA Block hematoma, black eye serves as a media for spread of external infection to eye.
27

Pathway of spread of infection to cavernous sinus
28

Veins of the neck
The word "jugular" refers to the throat or neck. It derives from the Latin "jugulum" meaning throat or collarbone and the Latin "jugum" meaning yoke. To go for the jugular is to attack a vital part that is particularly vulnerable.
29

30

External jugular vein largely drainsscalp and face, but also some deeperparts.Formed by union of post divisiion ofretromandibular vein & post auricularvein.Begins near the angle of mandible,justbelow the parotid gland and drains intosubclavian vein.Covered with platysma and superficialfascia and separated fromsternocleidomastoid by deep cervicalfascia.Between the entrance into subclavianvein, abt 4cm above clavicle, it is oftendilated as so called sinus.Surface anatomy: usualy visible as itcrosses sternocleidomastoid obliquely.Can be seen by effort blowing ofmouth closed
31

Tributries of external jugular vein
• Posterior external jugular vein
• Transverse cervical vein
• Suprascapular vein
• Anterior jugular vein
• A branch from internal jugular in the parotid
• Occasionally joined by occipital
32
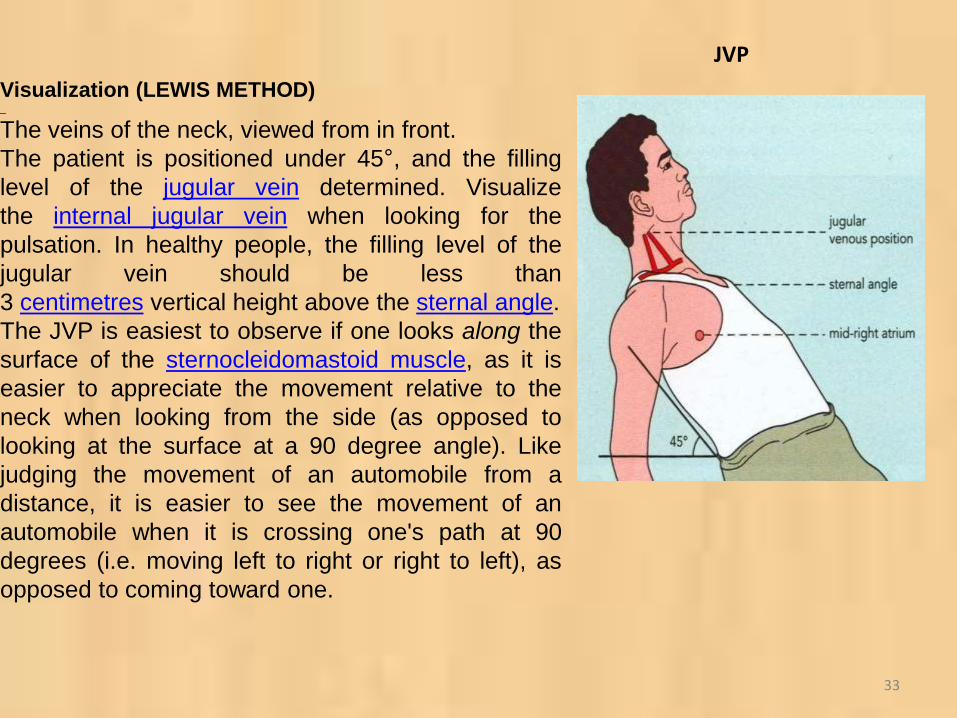
Visualization (LEWIS METHOD)
The veins of the neck, viewed from in front.
The patient is positioned under 45°, and the filling
level of the jugular vein determined. Visualize
the internal jugular vein when looking for the
pulsation. In healthy people, the filling level of the
jugular vein should be less than
3 centimetres vertical height above the sternal angle.
The JVP is easiest to observe if one looks along the
surface of the sternocleidomastoid muscle, as it is
easier to appreciate the movement relative to the
neck when looking from the side (as opposed to
looking at the surface at a 90 degree angle). Like
judging the movement of an automobile from a
distance, it is easier to see the movement of an
automobile when it is crossing one's path at 90
degrees (i.e. moving left to right or right to left), as
opposed to coming toward one.
JVP
33
• The JVP and carotid pulse can be differentiated several ways
• multiphasic - the JVP "beats" twice (in quick succession) in the cardiac cycle. In other words, there are two waves in the JVP for each contraction-relaxation cycle by the heart. The first beat represents that atrial contraction (termed a) and second beat represents venous filling of the right atrium against a closed tricuspid valve (termed v) and not the commonly mistaken 'ventricular contraction'. These wave forms may be altered by certain medical conditions; therefore, this is not always an accurate way to differentiate the JVP from the carotid pulse. The carotid artery only has one beat in the cardiac cycle.
• non-palpable - the JVP cannot be palpated. If one feels a pulse in the neck, it is generally the common carotid artery.
• occludable - the JVP can be stopped by occluding the internal jugular vein by lightly pressing against the neck. It will fill from above.
• varies with head-up-tilt (HUT) - the JVP varies with the angle of neck. If a person is standing, his JVP appears to be lower on the neck (or may not be seen at all because it is below the sternalangle). The carotid pulse's location does not vary with HUT.
• varies with respiration - the JVP usually decreases with deep inspiration.
Differentiation from the carotid pulse
34

Jugular vein
No pulsations palpable
Pulsations are obliterated by pressure above the clavicle
Levels of pulse wave decrease on inspiration; increased on expiration
Usually two pulsations per systole
Pulsations sometimes are prominent without abdominal pressure
Carotid artery
pulsations palpable
Pulsations are not obliterated by pressure above the clavicle
No effects of respiration on pulse
One pulsation per systole
No effect of abdominal pressure on pulsations
35
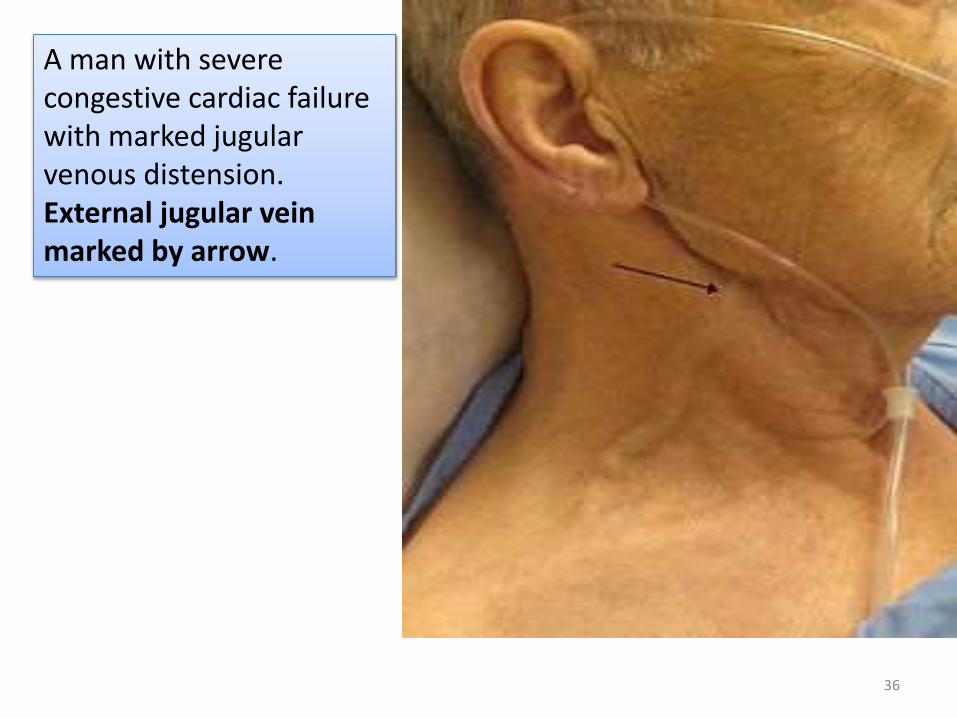
A man with severe congestive cardiac failure with marked jugular venous distension.External jugular vein marked by arrow.
36
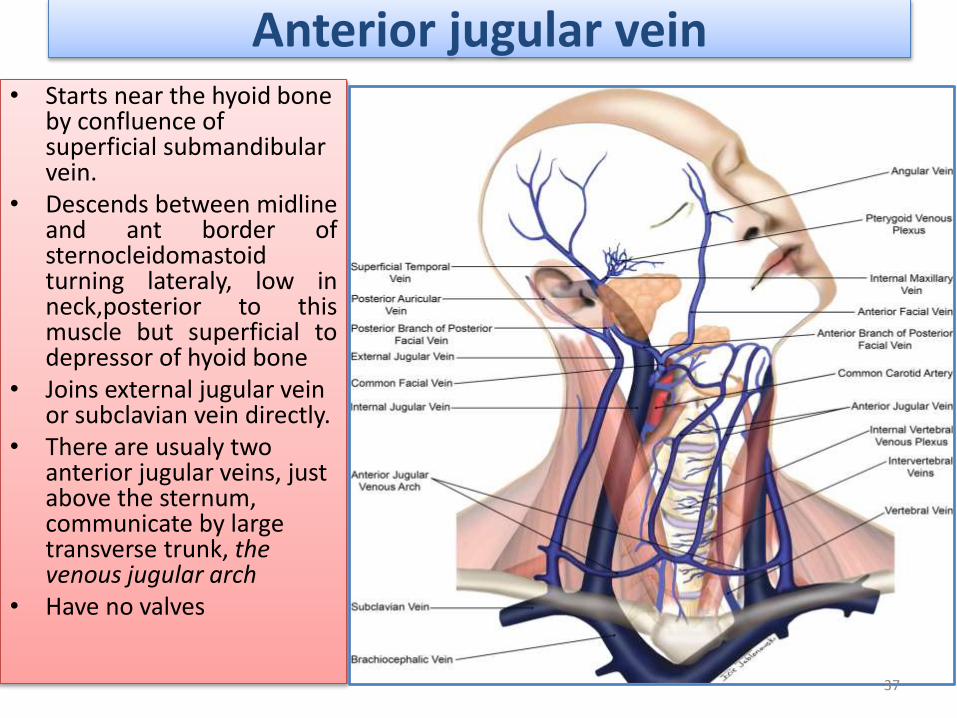
Anterior jugular vein• Starts near the hyoid bone
by confluence of superficial submandibularvein.
• Descends between midlineand ant border ofsternocleidomastoidturning lateraly, low inneck,posterior to thismuscle but superficial todepressor of hyoid bone
• Joins external jugular vein or subclavian vein directly.
• There are usualy two anterior jugular veins, just above the sternum, communicate by large transverse trunk, the venous jugular arch
• Have no valves
37
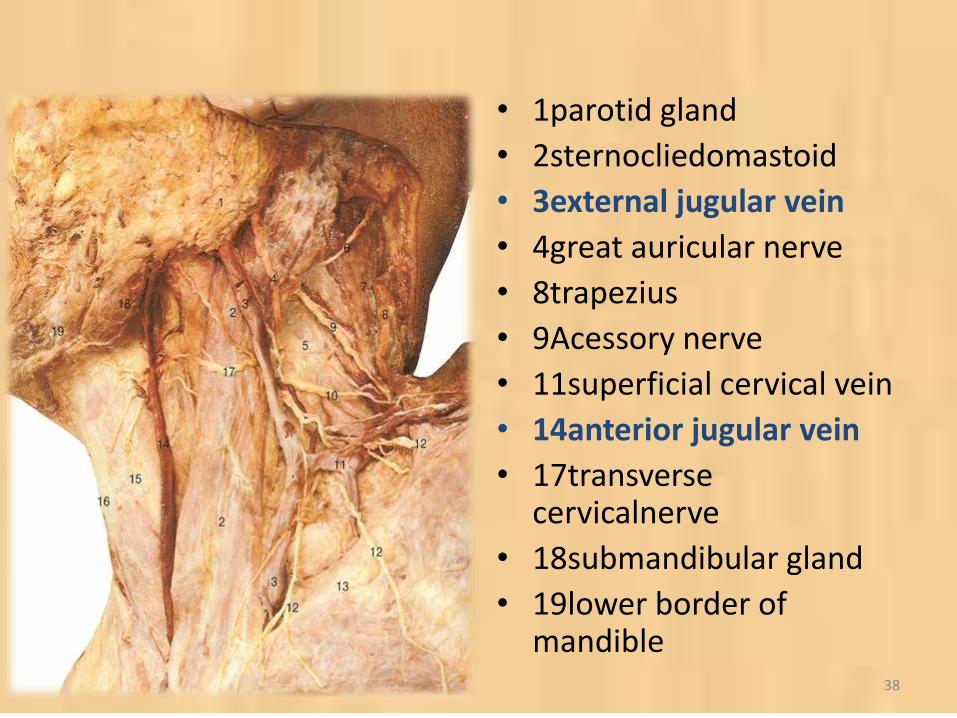
• 1parotid gland
• 2sternocliedomastoid
• 3external jugular vein
• 4great auricular nerve
• 8trapezius
• 9Acessory nerve
• 11superficial cervical vein
• 14anterior jugular vein
• 17transverse cervicalnerve
• 18submandibular gland
• 19lower border of mandible
38
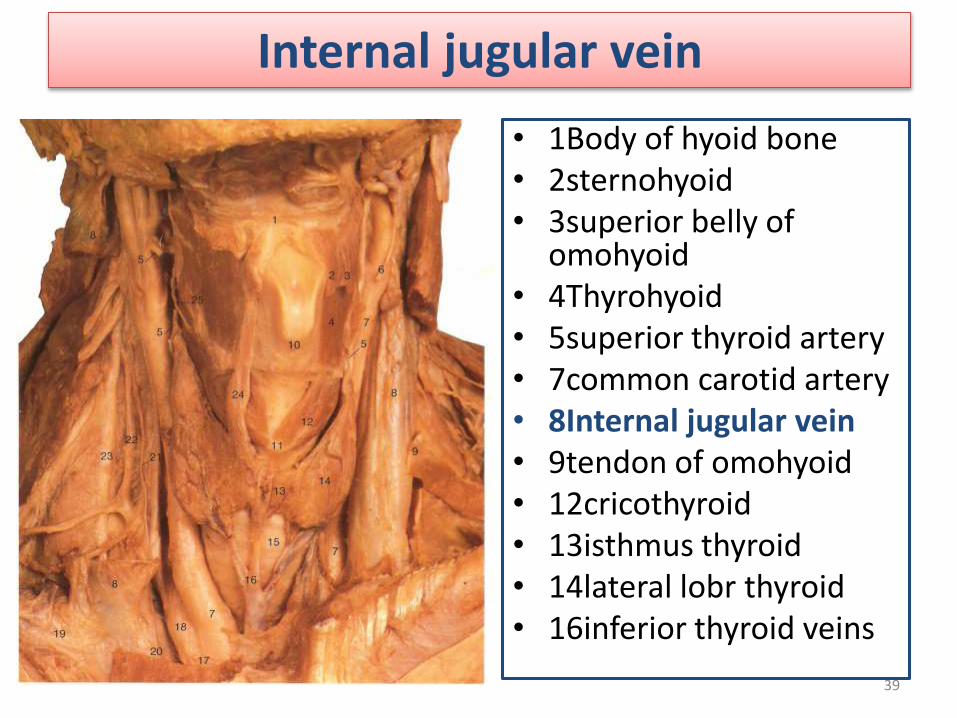
Internal jugular vein
• 1Body of hyoid bone• 2sternohyoid• 3superior belly of
omohyoid• 4Thyrohyoid• 5superior thyroid artery• 7common carotid artery• 8Internal jugular vein• 9tendon of omohyoid• 12cricothyroid• 13isthmus thyroid• 14lateral lobr thyroid• 16inferior thyroid veins
39
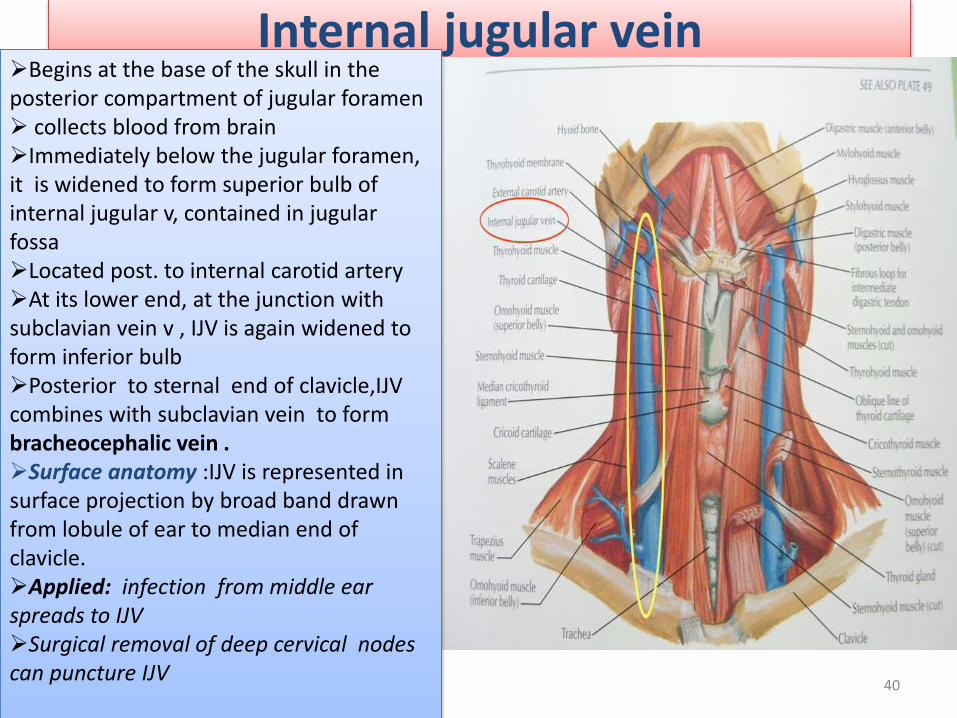
Internal jugular veinBegins at the base of the skull in the posterior compartment of jugular foramen collects blood from brainImmediately below the jugular foramen, it is widened to form superior bulb of internal jugular v, contained in jugular fossaLocated post. to internal carotid artery At its lower end, at the junction with subclavian vein v , IJV is again widened to form inferior bulbPosterior to sternal end of clavicle,IJVcombines with subclavian vein to form bracheocephalic vein .Surface anatomy :IJV is represented in surface projection by broad band drawn from lobule of ear to median end of clavicle.Applied: infection from middle ear spreads to IJV Surgical removal of deep cervical nodes can puncture IJV
40
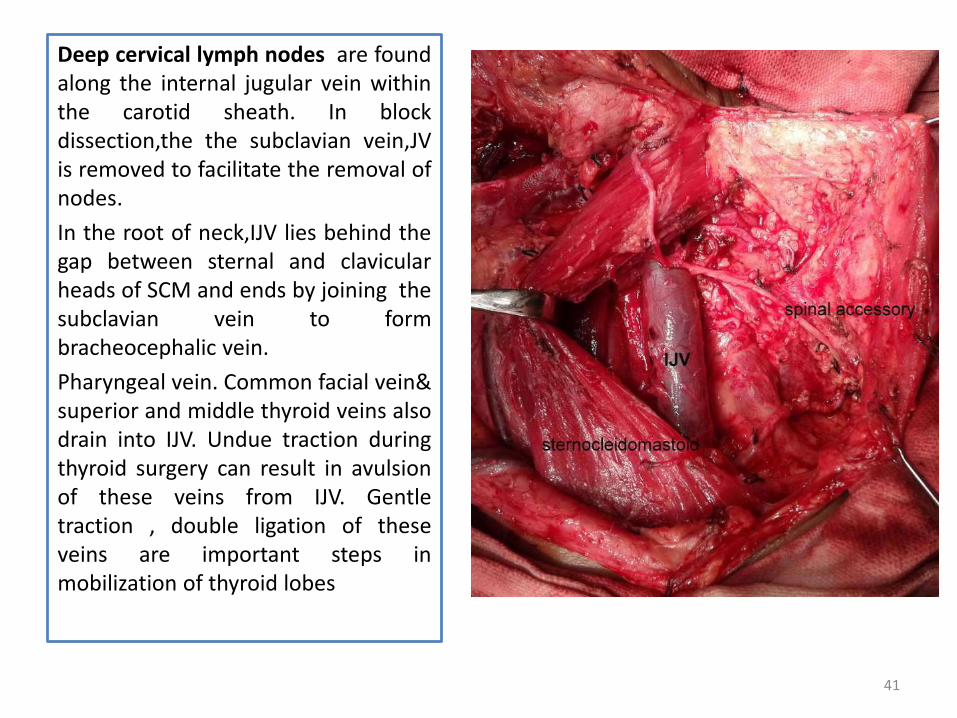
Deep cervical lymph nodes are foundalong the internal jugular vein withinthe carotid sheath. In blockdissection,the the subclavian vein,JVis removed to facilitate the removal ofnodes.
In the root of neck,IJV lies behind thegap between sternal and clavicularheads of SCM and ends by joining thesubclavian vein to formbracheocephalic vein.
Pharyngeal vein. Common facial vein&superior and middle thyroid veins alsodrain into IJV. Undue traction duringthyroid surgery can result in avulsionof these veins from IJV. Gentletraction , double ligation of theseveins are important steps inmobilization of thyroid lobes
41

Bilateral internal, external, posterior external and anterior
jugular vein ligations and excisions performed in the neck due
to larynx tumors . Radical neck dissection is a standard
procedure in the management of head and neck cancer
patients with bilateral lymph node metastasis to the neck.
Sacrifice of both internal and external jugular veins bilaterally
has been recognized as a dangerous approach leading to
intracranial hypertension with subsequent neurological sequela
and death.. After bilateral jugular vein ligations, digital
subtraction angiography (DSA) showed that the venous
drainage route of the brain had been diverted from the jugular
veins to the vertebral venous plexus.
42

Tributaries of internal jugular vein
•Into superior bulb•Inferior petrosal sinus•Veins of pharynx•Root of tongue & sublingual area•Superior thyroid vein•Middle thyroid vein
:
43
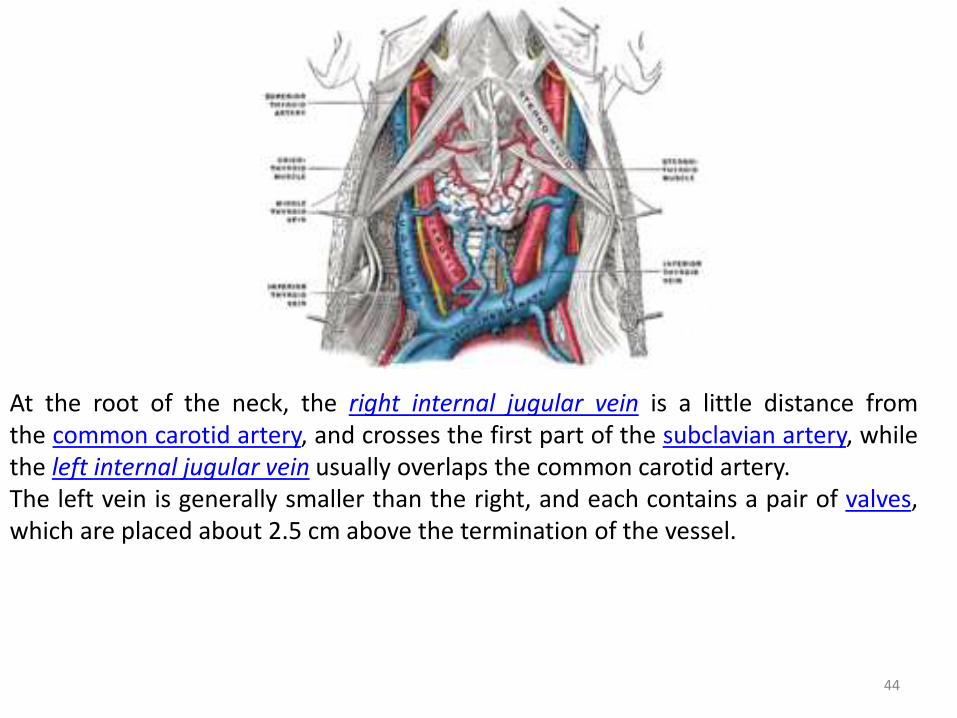
At the root of the neck, the right internal jugular vein is a little distance fromthe common carotid artery, and crosses the first part of the subclavian artery, whilethe left internal jugular vein usually overlaps the common carotid artery.The left vein is generally smaller than the right, and each contains a pair of valves,which are placed about 2.5 cm above the termination of the vessel.
44
• Thrombosis of the internal jugular (IJ) vein is an underdiagnosed condition that may occur as acomplication of head and neck infections, surgery, central venous access, local malignancy,polycythemia,hyperhomocysteinemia, neck massage, and intravenous drug abuse.
• thrombosis may become secondarily infected, producing a septic thrombophlebitis. An infected IJthrombus caused by extension of an oropharyngeal infection is referred to as Lemierre syndrome. Theincidence of Lemierre syndrome has fallen dramatically since the use of antibiotics began in the late 1950s.However, it still occurs, particularly in underserved populations.
• The frequency of IJ vein thrombosis in individuals who abuse intravenous drugs is not known, but it usuallyoccurs in people who have been using injectable drugs for years and have exhausted all peripheral accesssites.
• The symptoms and signs of IJ thrombosis can often be very subtle, making it easy to overlook the diagnosis. Pain and swelling at the angle of the jaw and a palpable cord beneath the sternocleidomastoid muscle both may be absent in a significant minority of patients. Once infection has set in, other objective findings may be found. Tovi et al described the following clinical manifestations in their 1991 series of patients with septic IJ thrombosis as follows:
• Clinical manifestations of IJ thrombosis occur in the following percentages of patients:
• Fever - 83% of patients
• Leukocytosis - 78% of patients
• Cervical pain - 66% of patients
• Mass or neck swelling - 72% of patients
• Sepsis syndrome - 39% of patients
• Pleuropulmonary complications - 28% of patients
• Superior vena cava syndrome - 11% of patients
• Chylothorax - 5% of patients
• Jugular foramen syndrome - 6% of patients
• Increased intracranial pressure with symptoms that include headache, visual disturbances, and altered sensorium - rare
APPLI ED
ASPECTIJV
45

Jugular phlebectasia in children• Jugular phlebectasia is a congenital dilatation of jugular vein which appears as a
soft, compressible mass in the neck only during straining or crying. It should be
differentiated from laryngocele, cysts and tumors of neck which may also appear
during straining. Ultrasonography (US) and computerized tomography (CT) are
diagnostic methods to distinguish the pathology
• More common in internal jugular vein.
• The Valsalva maneuver is most important for establishing the diagnosis.
Ultrasound or CDFI, or in combination with the Valsalva's breathing test, was the
diagnostic procedure of choice to confirm the diagnosis of JVP because of its
clarity, safety, and low cost. Surgical intervention is recommended for cosmetic
and psychologic purposes. Ligation or excision of the involved jugular vein is very
safe, simple, and effective for most patients. However, in cases of lesions of the
right and bilateral internal jugular veins, longitudinal constriction suture
venoplasty plus encapsulation might be more preferable and safer, and should be
recommended. Otherwise, treatment should be conservative (follow-up
evaluation).
46
• The jugular veins are relatively superficial and notprotected by tissues such as bone or cartilage. Thismakes them susceptible to damage. Due to the largevolumes of blood that flow though the jugular veins,damage to the jugulars can quickly cause significantblood loss, which can lead to hypovolemic shock andthen death if not treated.
• It should also be noted that cuts or abrasions in theskin near the jugular vein will bleed longer and moreprofusely (i.e. from chewing tobacco or shavingaccidents). Since 95% of the body's blood passesthrough this vein, it takes on average about 30minutes to fully stop a shaving abrasion on the face.
47
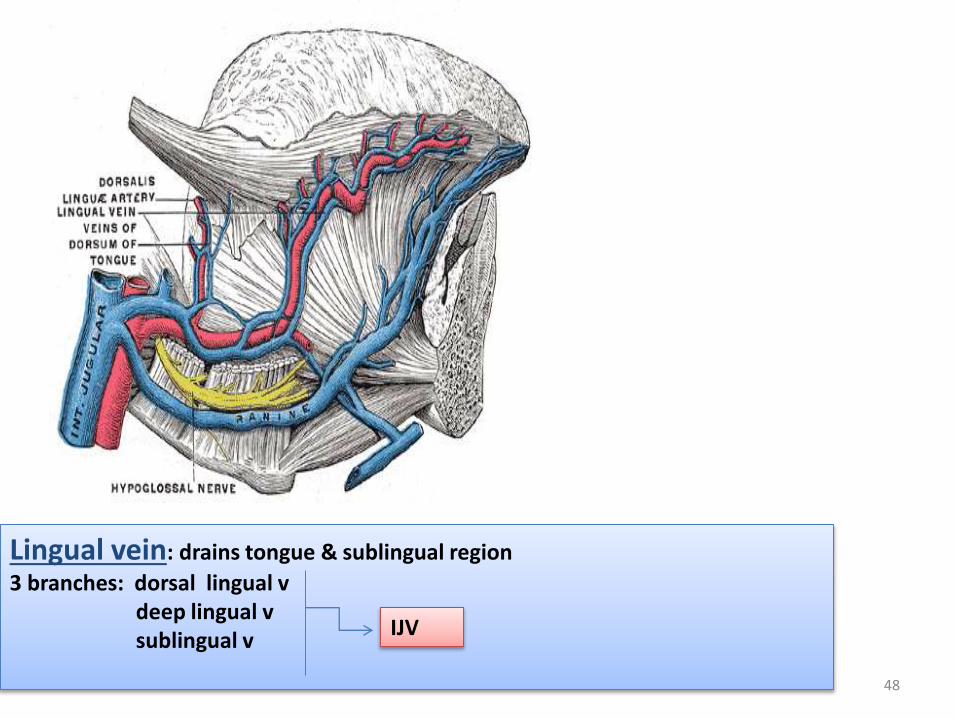
Lingual vein: drains tongue & sublingual region
3 branches: dorsal lingual v deep lingual v sublingual v
IJV
48

Abnormaly dilated, tortuous veins produced by prolonged, increaseintraluminal pressure. Small purplish or blue-black round swellings under thetongue with age and are known as “caviar lesions”
Lingual varicosity
Veins are supposed to act as one-way valves and shouldn't allow back flow of blood. But if a vein becomes weak, blood may flow backwards and collect in your vein causing inflammation and swelling. These swollen veins are varicose veins. Varicose veins are normally found on the backs of your calves or on the inside of your leg. No treatment is indicated for lingual varices.. Care needs to be exercised when performing surgery in this region due to the high vascularity of the area.
49
Subclavian vein
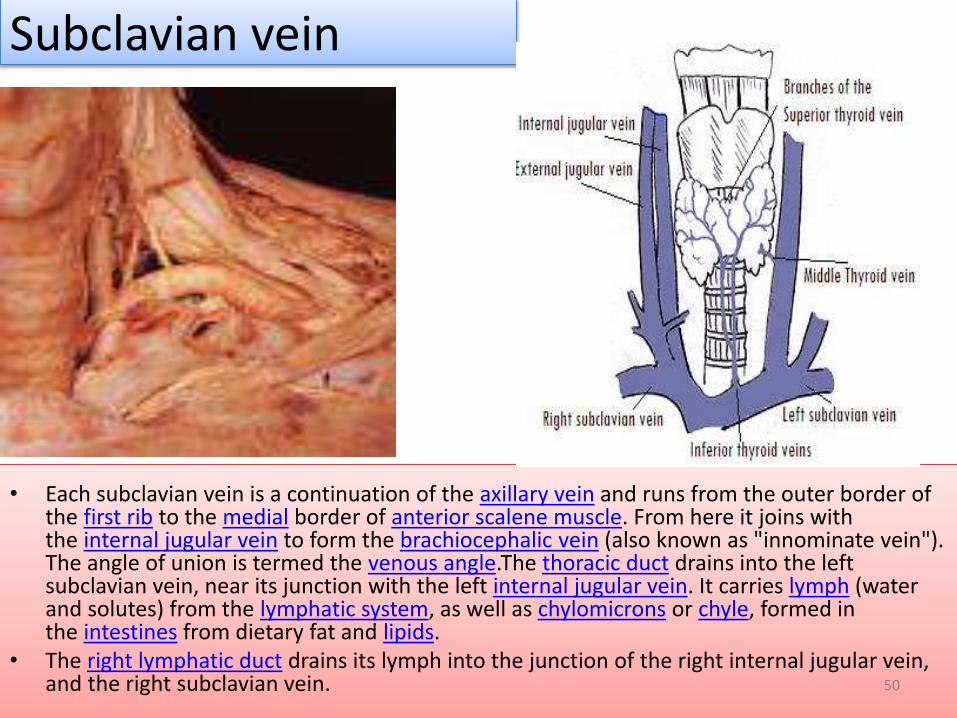
• Each subclavian vein is a continuation of the axillary vein and runs from the outer border of the first rib to the medial border of anterior scalene muscle. From here it joins with the internal jugular vein to form the brachiocephalic vein (also known as "innominate vein"). The angle of union is termed the venous angle.The thoracic duct drains into the left subclavian vein, near its junction with the left internal jugular vein. It carries lymph (water and solutes) from the lymphatic system, as well as chylomicrons or chyle, formed in the intestines from dietary fat and lipids.
• The right lymphatic duct drains its lymph into the junction of the right internal jugular vein, and the right subclavian vein. 50

51
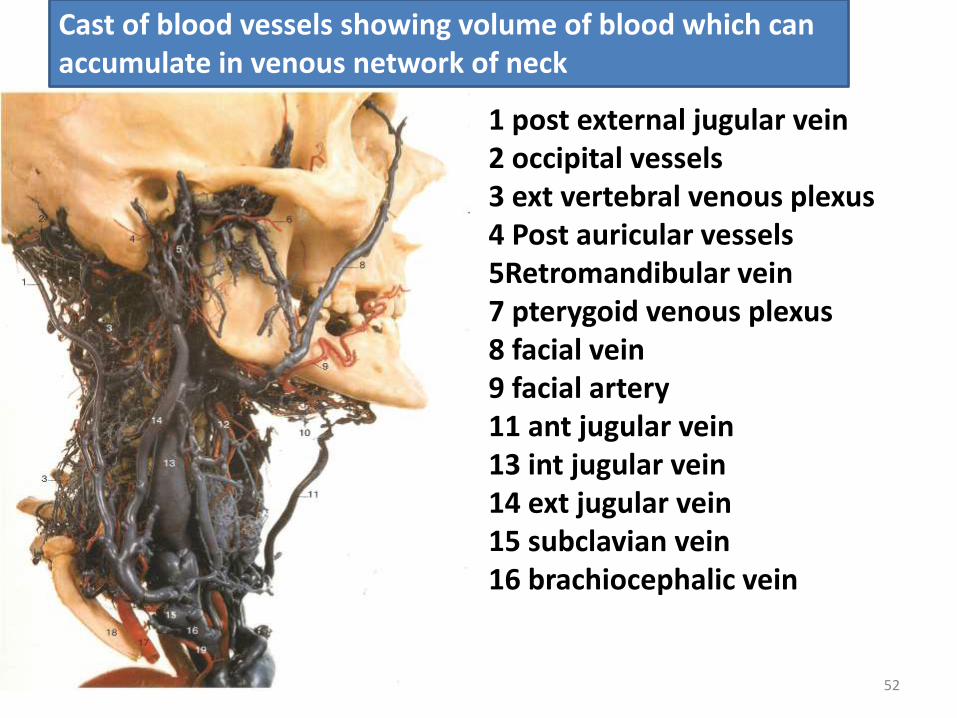
1 post external jugular vein2 occipital vessels3 ext vertebral venous plexus4 Post auricular vessels5Retromandibular vein7 pterygoid venous plexus8 facial vein9 facial artery11 ant jugular vein13 int jugular vein14 ext jugular vein15 subclavian vein16 brachiocephalic vein
Cast of blood vessels showing volume of blood which can accumulate in venous network of neck
52
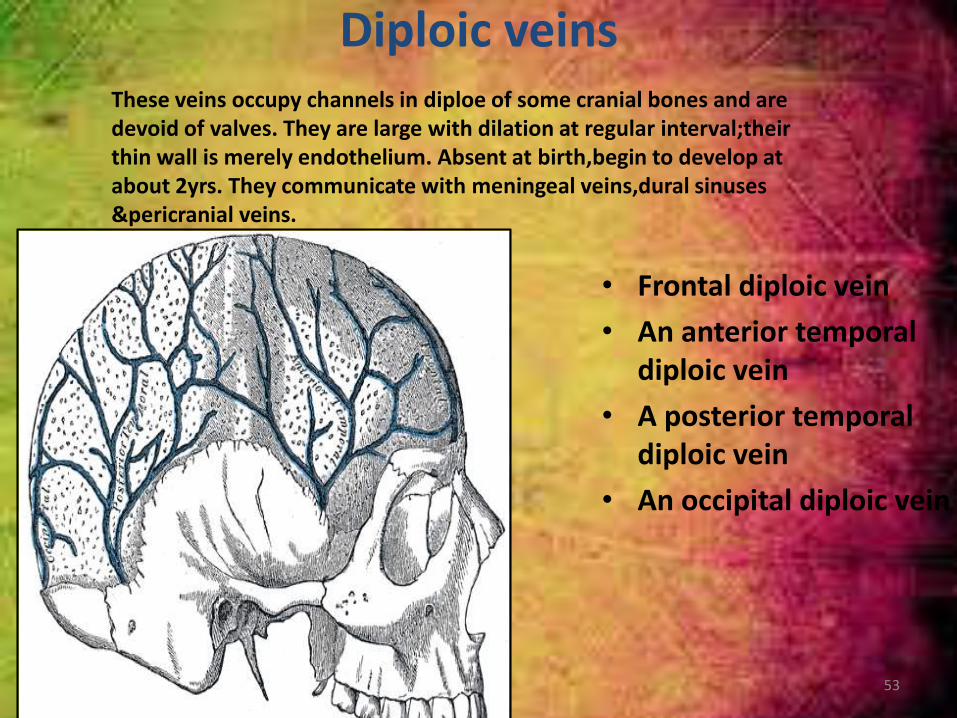
Diploic veins
• Frontal diploic vein
• An anterior temporal diploic vein
• A posterior temporal diploic vein
• An occipital diploic vein
These veins occupy channels in diploe of some cranial bones and are devoid of valves. They are large with dilation at regular interval;theirthin wall is merely endothelium. Absent at birth,begin to develop at about 2yrs. They communicate with meningeal veins,dural sinuses &pericranial veins.
53

Cerebral veins• They are divided into
external & internal groups according to the outer surface or inner parts of hemispheres they drain into.
• External cerebral veinSuperior cerebral vein
• middle cerebral vein• Inferior cerebral veins • Basal vein .• Internal cerebral veins
External cerebral veins drain into superior saggital sinusInternal cerebral veins drain into great cerebral veins of Galen
54
CRANIAL VENOUS SINUSES
These are spaces between endosteal & meningeal layers
of duramater.
General features:
Their walls are formed by duramater lined by
epithelium, muscular coat is absent
They have no valves
Receive 1) venous blood from brain, meninges and
bone
2) the CSF
major draining pathways from the brain,predominantly
to internal jugular veins.
They communicate with veins outside the skull through
emissary veins. These connections help to keep pressure
of blood in sinus constant.
55

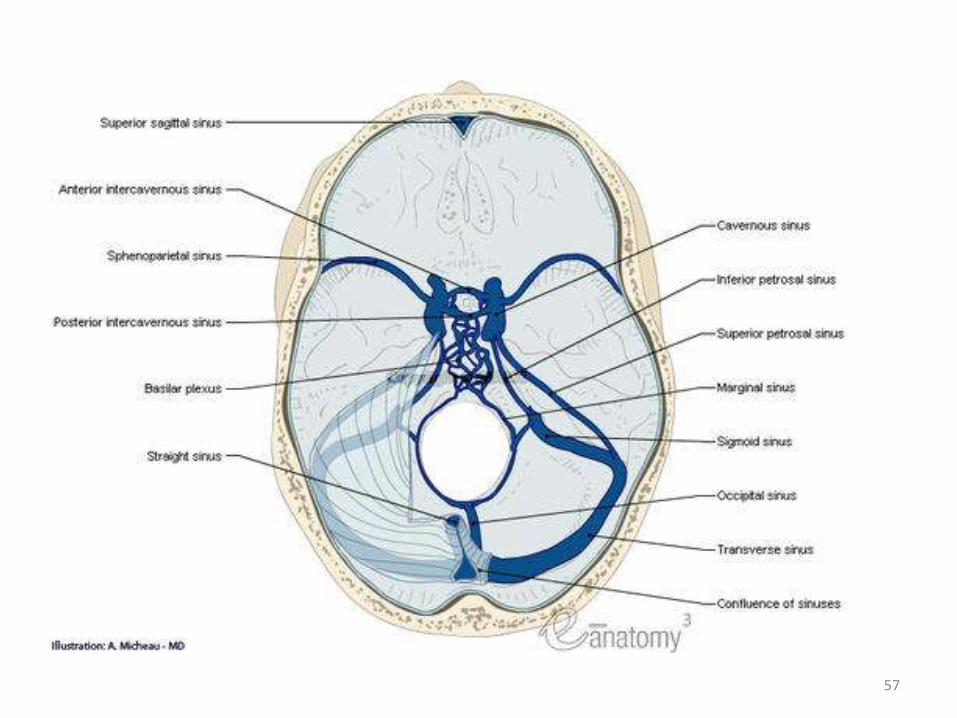
Paired
Cavernous sinus
Superior petrosal sinus
Inferior petrosal sinus
Transverse sinus
Sigmoid sinus
Sphenoparietal sinus
Middle meningeal veins
• Unpaired
• Superior saggital sinus
• Inferior saggital sinus
• Straight sinus
• Occipital sinus
• Ant. intercavernous S
• Post. intercavernous S
• Basilar plexus of veins
Dural venous sinuses
56
57

58
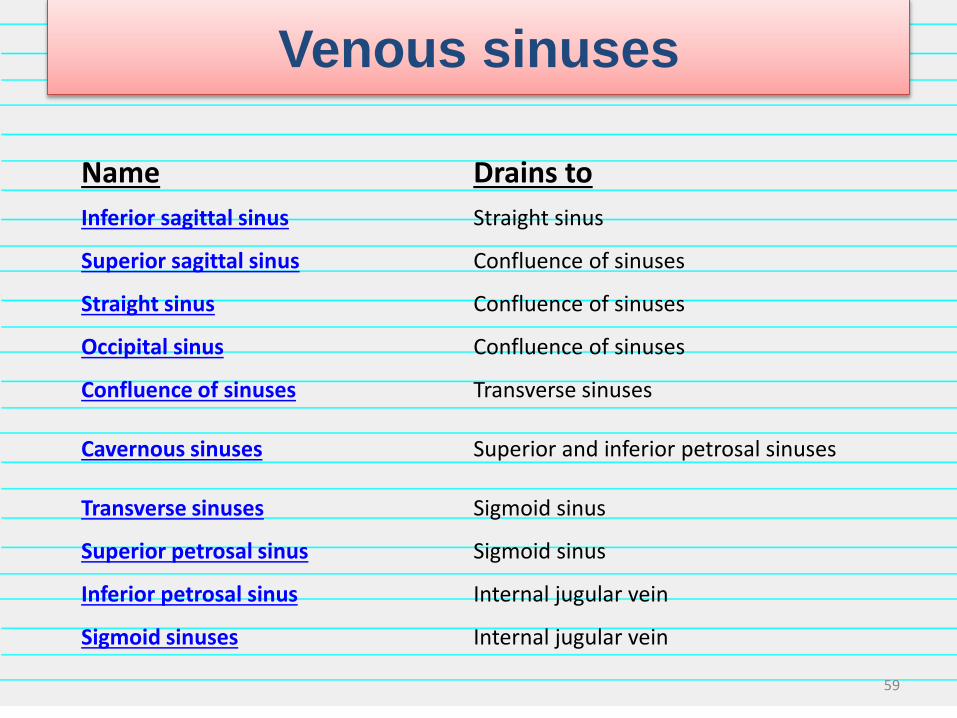
Venous sinuses
Name Drains to
Inferior sagittal sinus Straight sinus
Superior sagittal sinus Confluence of sinuses
Straight sinus Confluence of sinuses
Occipital sinus Confluence of sinuses
Confluence of sinuses Transverse sinuses
Cavernous sinuses Superior and inferior petrosal sinuses
Transverse sinuses Sigmoid sinus
Superior petrosal sinus Sigmoid sinus
Inferior petrosal sinus Internal jugular vein
Sigmoid sinuses Internal jugular vein
59

Sup cerebral vein superior saggital sinusright transverse sinussigmoid sinusRt IJV
Deep cerebral vgreat cerebral vstraight sinusleft transverse slft sigmoid slft IJV
60
Clinical relevance
Dural sinus thrombosis may lead to haemorrhagic infarction with
serious consequences including epilepsy, neurological deficits
and death.
Common causes of dural venous sinus thrombosis include head
and neck infections, head injury,skull fractures or intracranial
hematomas either by direct compression of the sinus or
endothelial damage within the sinus can cause the activation of
coagulation system resulting in sinus occlusion.Brain cells
contain an abundance of thromboplastin that is released after
injury inducing an hypercoagulable state leading to destruction of
platelets & erythrocytes followed by thrombus formation.
Most common thrombosed sinuses are tranverse,cavernous &
superior saggital sinus
Clinical symptomsheadache,papilloedema,impaired consciousness, vomitting.
61

Metastasis of tumour cells to dural sinuses
Tha basilar and occipital sinuses communicate through the
foramen magnum with the internal venous plexuses. Because
these venous channels are valveless, compression of the
thorax, abdomen, or pelvis as occurs during heavy coughing and
straining may force venous blood from these regions into
vertebral venous system and from it into dural venous sinuses.
As a a result, pus in the abscesses and tumour cells in these
regions may spread to vertebrae and brain.
62
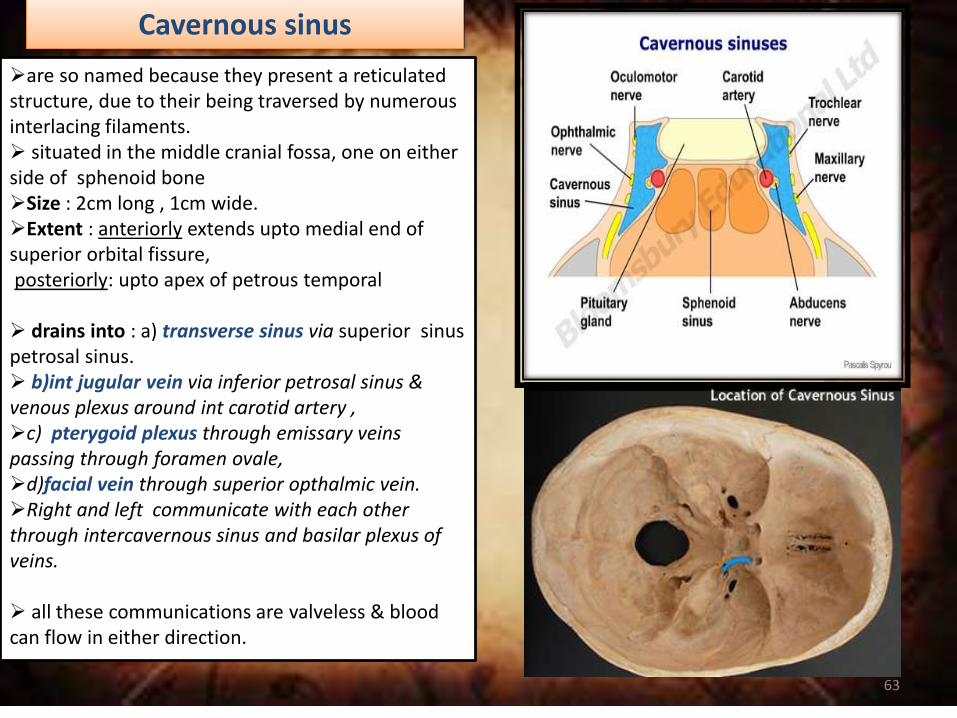
Cavernous sinus
are so named because they present a reticulated structure, due to their being traversed by numerous interlacing filaments. situated in the middle cranial fossa, one on either side of sphenoid boneSize : 2cm long , 1cm wide.Extent : anteriorly extends upto medial end of superior orbital fissure,posteriorly: upto apex of petrous temporal
drains into : a) transverse sinus via superior sinus petrosal sinus. b)int jugular vein via inferior petrosal sinus & venous plexus around int carotid artery ,c) pterygoid plexus through emissary veins passing through foramen ovale, d)facial vein through superior opthalmic vein.Right and left communicate with each other through intercavernous sinus and basilar plexus of veins.
all these communications are valveless & blood can flow in either direction.
63
t
12
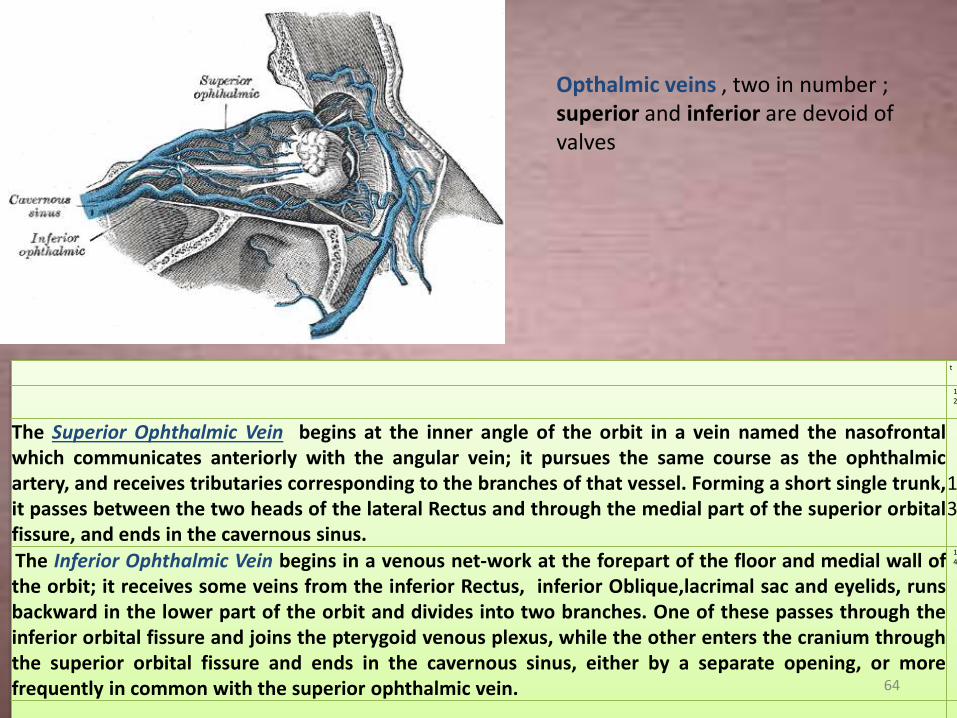
The Superior Ophthalmic Vein begins at the inner angle of the orbit in a vein named the nasofrontalwhich communicates anteriorly with the angular vein; it pursues the same course as the ophthalmicartery, and receives tributaries corresponding to the branches of that vessel. Forming a short single trunk,it passes between the two heads of the lateral Rectus and through the medial part of the superior orbitalfissure, and ends in the cavernous sinus.
13
The Inferior Ophthalmic Vein begins in a venous net-work at the forepart of the floor and medial wall ofthe orbit; it receives some veins from the inferior Rectus, inferior Oblique,lacrimal sac and eyelids, runsbackward in the lower part of the orbit and divides into two branches. One of these passes through theinferior orbital fissure and joins the pterygoid venous plexus, while the other enters the cranium throughthe superior orbital fissure and ends in the cavernous sinus, either by a separate opening, or morefrequently in common with the superior ophthalmic vein.
14
Opthalmic veins , two in number ; superior and inferior are devoid of valves
64

Applied anatomy Thrombosis caused by sepsis in the danger area of face, nasal cavity, paranasal sinuses give rise to :Nervous symptoms: 1) severe pain in the eye and forehead in the area of distribution of opthalmic nerve.2) Involvement of 3rd, 4th and 6th nerve resulting in paralysis of muscle supplied.Venous symptoms:1) Marked edema of eyelid, cornea & exopthalmos due to
congestion of orbital vein.Carotid and cavernous communication: because of peculiar relationship of cavernous sinus to internal carotid artery a communication may occur between the two as a result of injury.When this happens the arterial pressure is communicated through the sinus to vein of orbit & as a result the eye become prominent & pulsate with each heart beat( pulsating exopthalmos)
65

Cavernous sinus thrombophlebitis results as a complication of a prior orbitalcellulitis or may be a starting point of such an infection. In either event, theinflammation originates in the neighbourhood. The known avidity for theorbit to share the troubles of the neighour is due to free venouscommunication, anteriorly with the facial vein through angular vein andposteriorly with the cavernous sinus through the Ophthalmic veins. Thus anysuppuration in the vast area drained by these veins should be eyedsuspiciously and dealt with caution, as the prognosis is mostly fatal, becauseof the involvement of the cavernous sinus in the absence of proper therapy.With modern chemo-therapy the cases are seen rarely and only as a result ofinadequate attention and care of a seemingly harmless inflammation and or aresistant strain of organism.
66
Emissary veins are conduits between the extracranial scalp veins and the diploicand intracranial venous systems. These veins are valveless and therefore cantransmit infection from the extracranial to the intracranial compartment.
The meningeal veins are epidural veins that lie within the dura draining the falxcerebri, the tentorium, and the cranial dura. They run in shallow grooves on theinner table of the skull to communicate with the dural sinuses or traverseextracranially to the pterygoid plexus in the deep face or vertebral plexus aroundthe cervical spine.
The diploic veins are small irregular endothelial-lined channels coursing betweenthe inner and outer tables of the skull. These communicate with the extracranialvenous system, the meningeal veins, and the dural sinuses. They are rarely seenusing angiography unless enlarged, as in the case of an arterial-venousmalformation.
Communication between extracranial and intracranial veins
67

• Sinus pericranii (SP) is a rare disorder characterized by a congenital (oroccasionally, acquired) epicranial venous malformation of the scalp. Sinuspericranii is an abnormal communication between the intracranial andextracranial venous drainage pathways. Treatment of this condition hasmainly been recommended for aesthetic reasons and prevention ofhemorrhage. Sinus pericranii is a venous anomaly where a communicationbetween the intracranial dural sinuses and dilated epicranial venousstructures exists. That venous anomaly is a collection of nonmuscularvenous blood vessels adhering tightly to the outer surface of the skull anddirectly communicating with intracranial venous sinuses through diploicveins. The venous collections receive blood from and drain into theintracranial venous sinuses. The varicosities are intimately associated withthe periostium, are distensible, and vary in size when changes inintracranial pressure occur.
• the nature of this malformation remains unclear. Congenital, spontaneous, and acquired origins are accepted.The surgical treatment involves the resection of the extracranial venous package and ligation of the emissary communicating vein. In some cases of SP, surgical excision is performed for cosmetic reasons.
Sinus pericranii
68
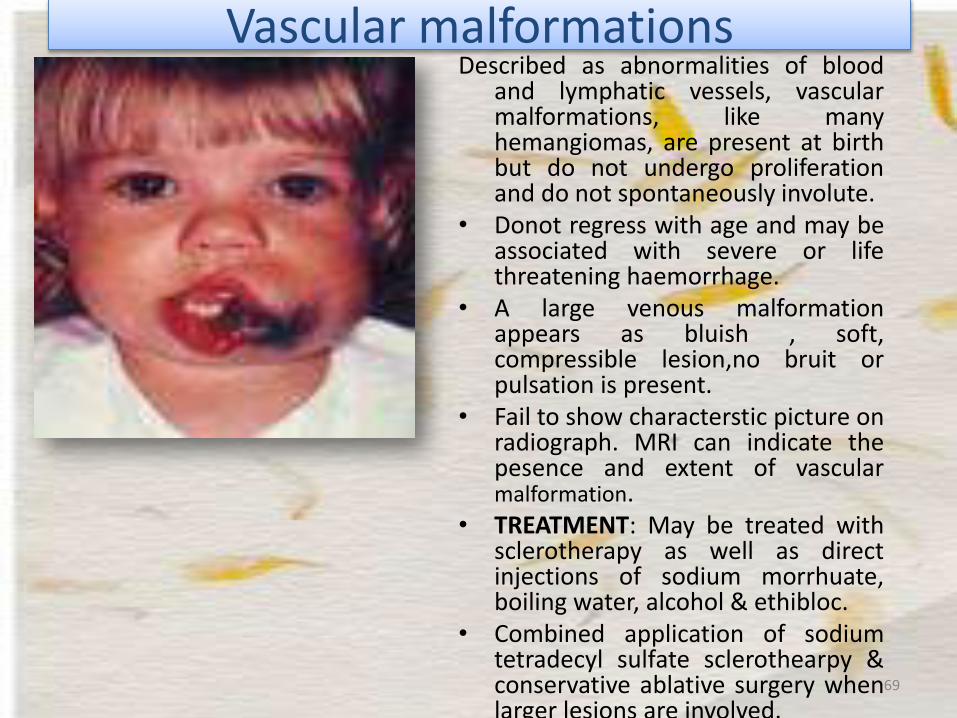
Vascular malformationsDescribed as abnormalities of blood
and lymphatic vessels, vascularmalformations, like manyhemangiomas, are present at birthbut do not undergo proliferationand do not spontaneously involute.
• Donot regress with age and may beassociated with severe or lifethreatening haemorrhage.
• A large venous malformationappears as bluish , soft,compressible lesion,no bruit orpulsation is present.
• Fail to show characterstic picture onradiograph. MRI can indicate thepesence and extent of vascularmalformation.
• TREATMENT: May be treated withsclerotherapy as well as directinjections of sodium morrhuate,boiling water, alcohol & ethibloc.
• Combined application of sodiumtetradecyl sulfate sclerothearpy &conservative ablative surgery whenlarger lesions are involved.
69

Telangiectasias on the face are often treated with a laser. Laser therapy uses a light beam that is pulsed onto the veins in order to seal them off, causing them to dissolve. These light-based treatments require adequate heating of the veins. These treatments can result in the destruction of sweat glands, and the risk increases with the number of treatments.
Telangiectasias or angioectasias are small dilated blood
vessels near the surface of the skin or mucous membranes,
measuring between 0.5 and 1 millimeter in diameter.They
can develop anywhere on the body but are commonly seen
on the face around the nose, cheeks, and chin. They can
also develop on the legs, specifically on the upper thigh,
below the knee joint, and around the ankles. Many patients
who suffer with spider veins seek the assistance of
physicians who specialize in vein care or peripheral vascular
disease. These physicians are called phlebologists or
interventional radiologists.
Some telangiectasia are due to developmental abnormalities
that can closely mimic the behaviour of benign vascular
neoplasms. They may be composed of abnormal
aggregations of arterioles, capillaries, or venules.
Telangiectasia
70
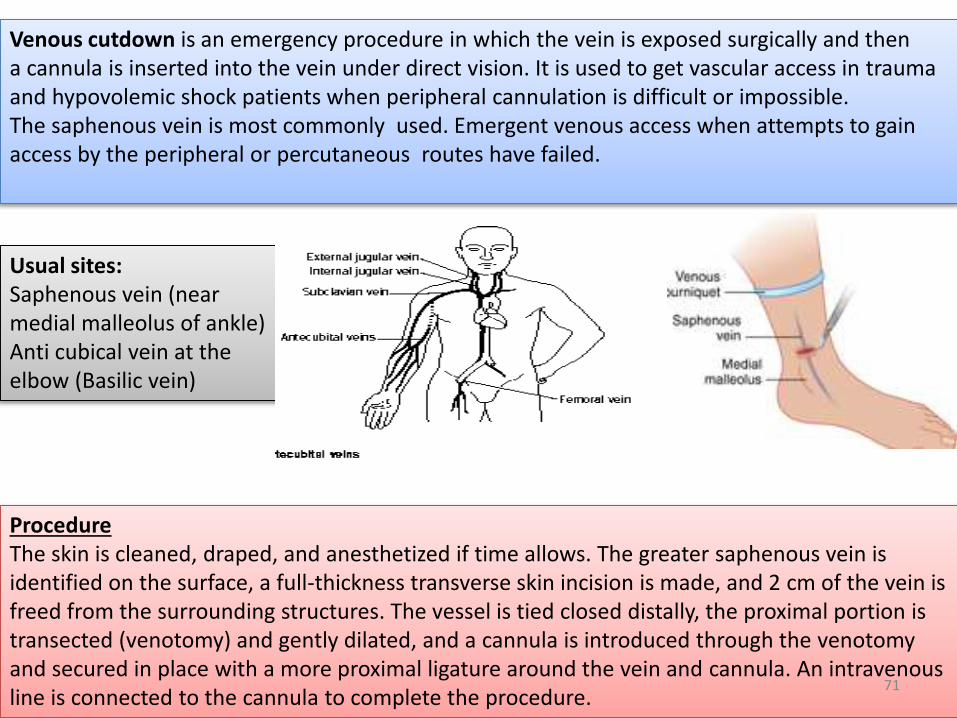
Usual sites:Saphenous vein (near medial malleolus of ankle)Anti cubical vein at the elbow (Basilic vein)
ProcedureThe skin is cleaned, draped, and anesthetized if time allows. The greater saphenous vein is identified on the surface, a full-thickness transverse skin incision is made, and 2 cm of the vein is freed from the surrounding structures. The vessel is tied closed distally, the proximal portion is transected (venotomy) and gently dilated, and a cannula is introduced through the venotomyand secured in place with a more proximal ligature around the vein and cannula. An intravenous line is connected to the cannula to complete the procedure.
Venous cutdown is an emergency procedure in which the vein is exposed surgically and then a cannula is inserted into the vein under direct vision. It is used to get vascular access in trauma and hypovolemic shock patients when peripheral cannulation is difficult or impossible. The saphenous vein is most commonly used. Emergent venous access when attempts to gain access by the peripheral or percutaneous routes have failed.
71

72
Complications of venous cutdown include cellulitis, hematoma, phlebitis, perforation of theposterior wall of the vein, venous thrombosis and nerve and arterial transection. Thisprocedure can result in damage to the saphenous nerve due to its intimate path with thegreat saphenous vein, resulting in loss of cutaneous sensation in the medial leg. Over theyears the venous cutdown procedure has become outdated by the introduction and recentpre hospital developments of intraosseous infusion in trauma/hypovolemic shock patients.
complications
73

In medicine, a central venous catheter ("central line", "CVC", "central venous line" or "centralvenous access catheter") is a catheterplaced into a large vein in the neck (internal jugularvein), chest (subclavian vein or axillary vein) or groin (femoral vein). It is used to administermedication or fluids, obtain blood tests (specifically the "mixed venous oxygen saturation"), anddirectly obtain cardiovascular measurements such as the central venous pressure.
Indications and usesIndications for the use of central lines include:Monitoring of the central venous pressure (CVP) in acutely ill patients to quantify fluid balanceLong-term Intravenous antibioticsLong-term Parenteral nutrition especially in chronically ill patientsLong-term pain medicationsChemotherapyCentral venous catheters usually remain in place for a longer period of time than other venousaccess devices, especially when the reason for their use is longstanding (such as total parenteralnutrition in a chronically ill patient). The line is then inserted using the Seldinger technique: ablunt guidewire is passed through the needle, then the needle is removed. A dilating device maybe passed over the guidewire to slightly enlarge the tract. Finally, the central line itself is thenpassed over the guidewire, which is then removed. All the lumens of the line are aspirated (toensure that they are all positioned inside the vein) and flushed. A chest X-ray is typicallyperformed afterwards to confirm that the line is positioned inside the superior vena cava and, inthe case of insertion through the subclavian vein, that no pneumothorax was caused as a sideeffect.
74

75
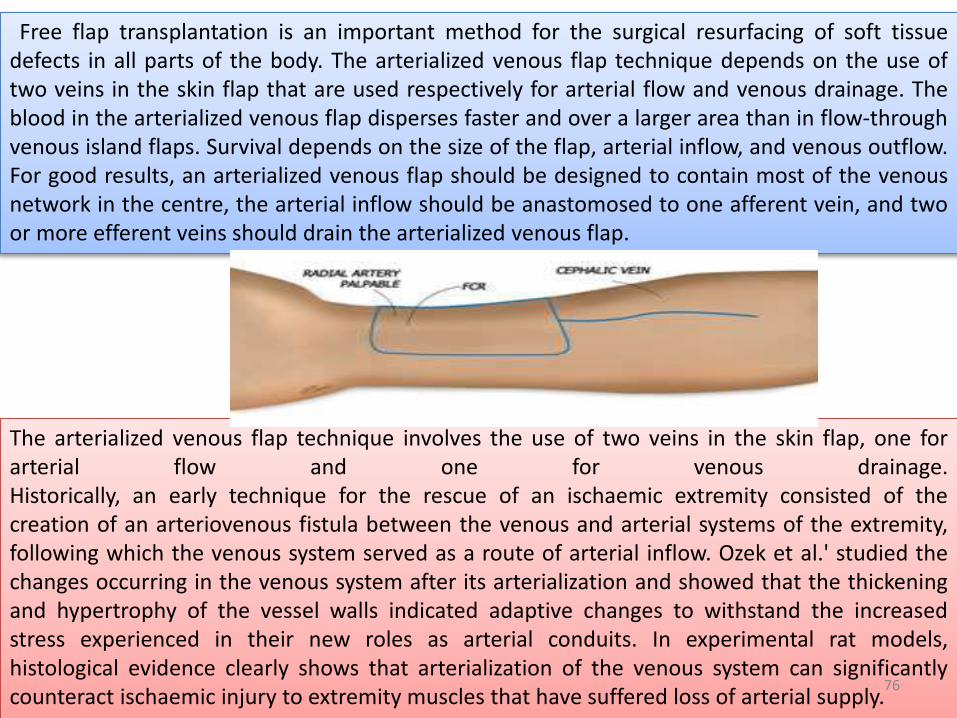
Free flap transplantation is an important method for the surgical resurfacing of soft tissuedefects in all parts of the body. The arterialized venous flap technique depends on the use oftwo veins in the skin flap that are used respectively for arterial flow and venous drainage. Theblood in the arterialized venous flap disperses faster and over a larger area than in flow-throughvenous island flaps. Survival depends on the size of the flap, arterial inflow, and venous outflow.For good results, an arterialized venous flap should be designed to contain most of the venousnetwork in the centre, the arterial inflow should be anastomosed to one afferent vein, and twoor more efferent veins should drain the arterialized venous flap.
The arterialized venous flap technique involves the use of two veins in the skin flap, one forarterial flow and one for venous drainage.Historically, an early technique for the rescue of an ischaemic extremity consisted of thecreation of an arteriovenous fistula between the venous and arterial systems of the extremity,following which the venous system served as a route of arterial inflow. Ozek et al.' studied thechanges occurring in the venous system after its arterialization and showed that the thickeningand hypertrophy of the vessel walls indicated adaptive changes to withstand the increasedstress experienced in their new roles as arterial conduits. In experimental rat models,histological evidence clearly shows that arterialization of the venous system can significantlycounteract ischaemic injury to extremity muscles that have suffered loss of arterial supply.
76

nada et al. studied factors affecting the survival ofthe arterialized venous flap and found that theseflaps could become necrotic in the presence of arelative excess of arterial blood inflow and that twovenous exits were more effective than one. Theyconcluded that survival depended on the size of theflap, arterial inflow, and venous outflow.
Woo et al.They recommended the following procedures for complete survival:an arterialized venous flap should be designed to contain most of the venous network in the centrethe arterial inflow should be anastomosed to one afferent veintwo or more efferent veins should drain the arterialized venous flap
Both the arterial and venous trees are actively involved in the exchange of oxygen and carbon dioxide.
77

Thank you
78











![ASSISTED VENOUS DRAINAGE. Gravity Drainage Patient to reservoir height gradient – [ table height ] Venous line resistance as contributed by the venous](https://img.pdfslide.us/doc/110x75/56649f125503460f94c255ca/assisted-venous-drainage-gravity-drainage-patient-to-reservoir-height-gradient.jpg)