Embed Size (px)
Citation preview
VALVE
REPLACEMENT
THERAPY IN
HEART
DISEASE IN
ADULTSSubhasish Deb
Burdwan Medical College
Department of General Medicine
SUBHASISH DEB, BMCH
ACC/AHAVALVULAR HEART DISEASE
GUIDELINES 2014
Rick A.Nishimura,M.D.,FACC
Catherine M.Otto,MD.,FACC
SUBHASISH DEB, BMCH
SUBHASISH DEB, BMCH
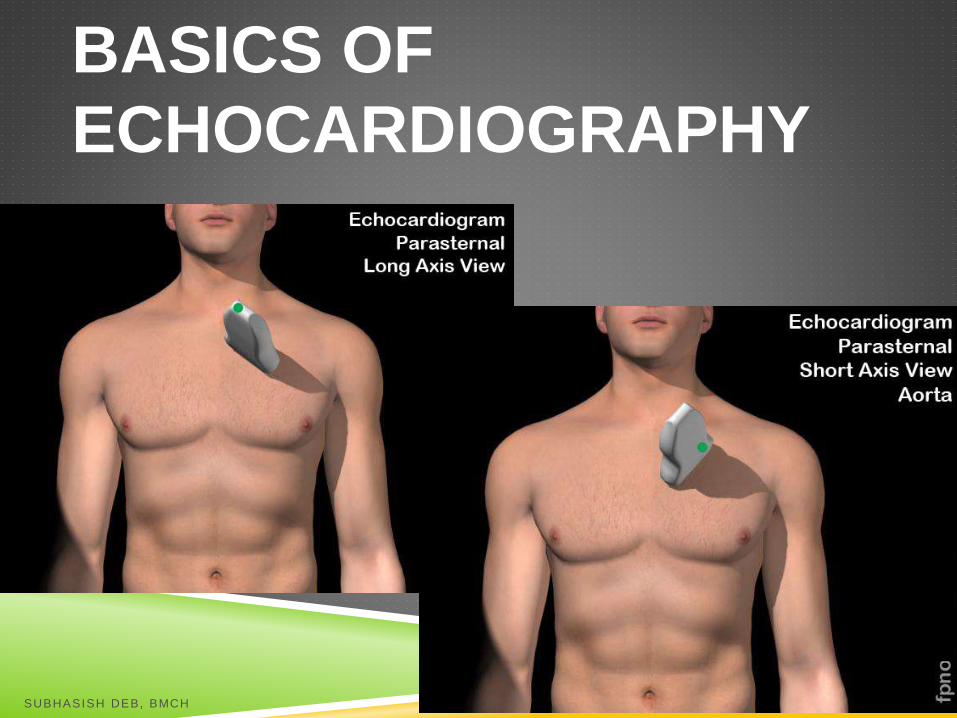
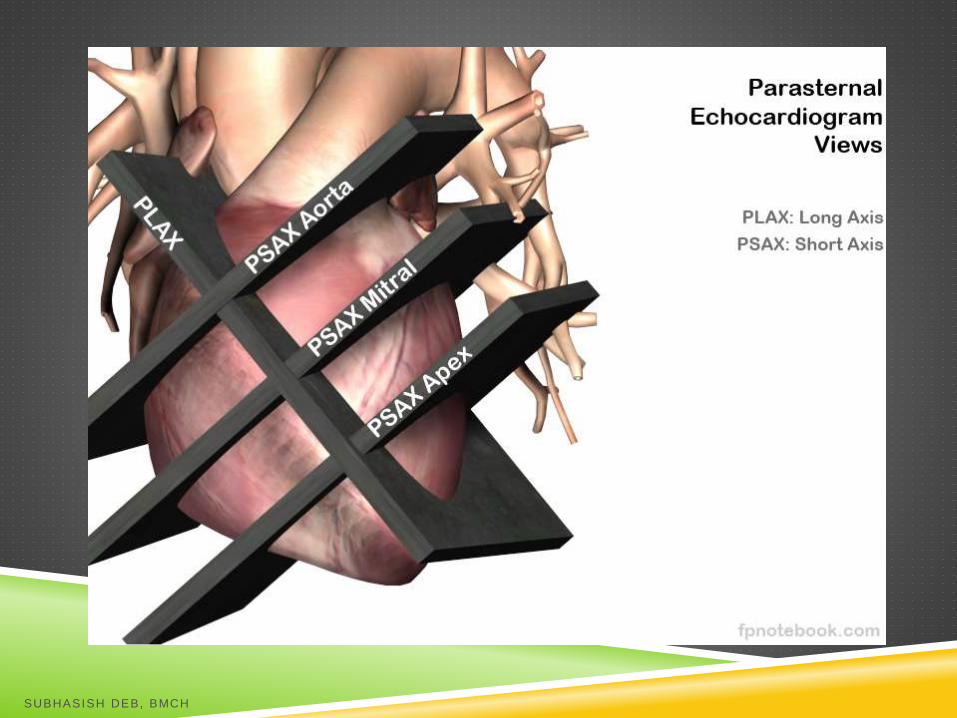
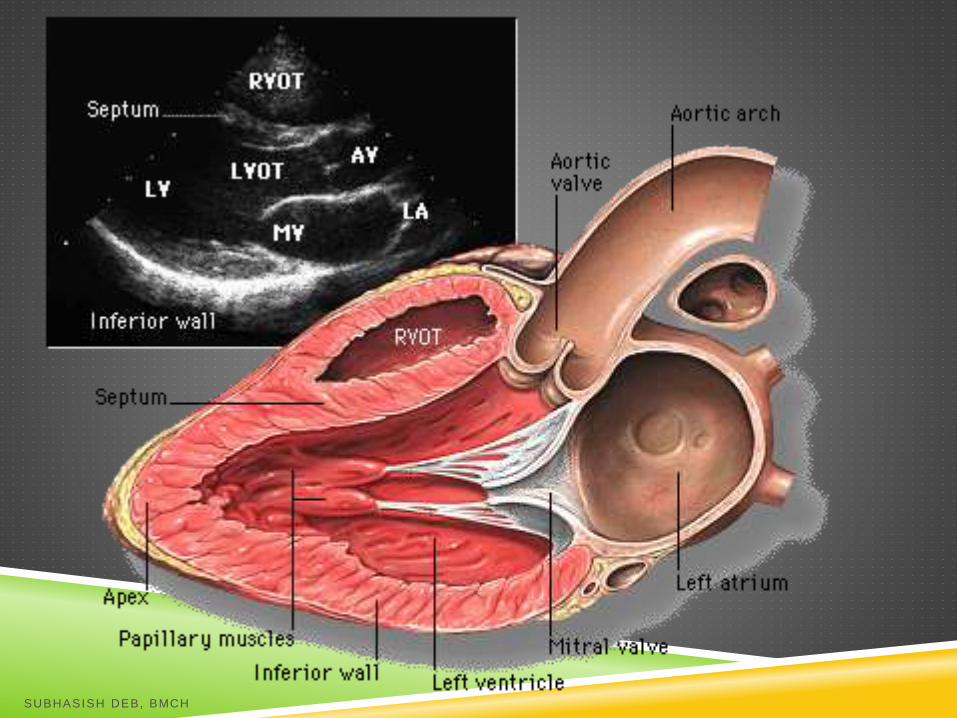
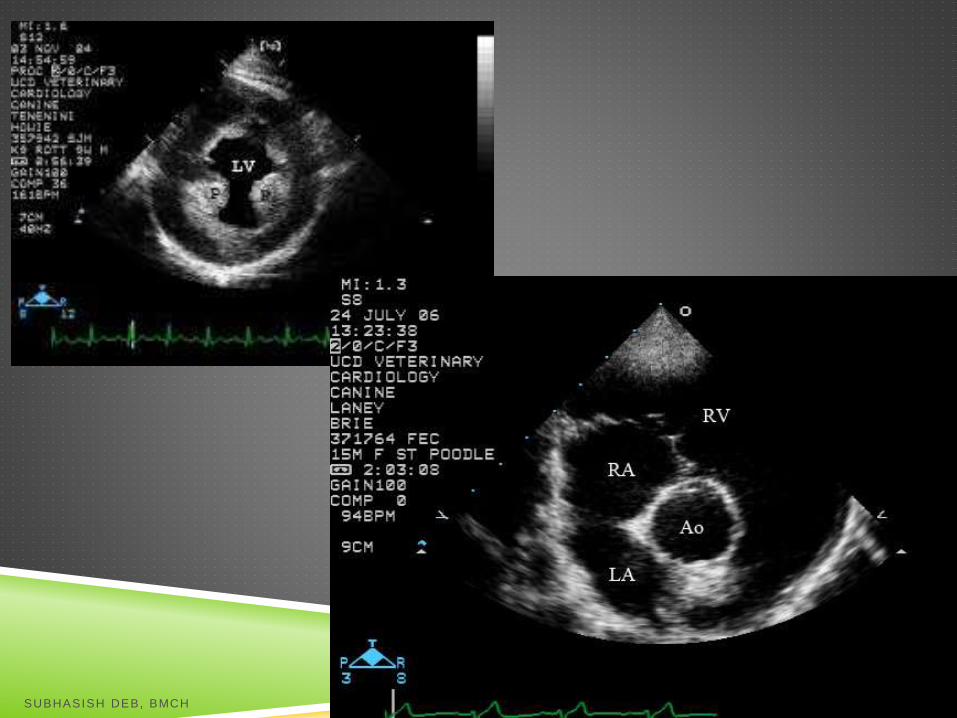
BASICS OF
ECHOCARDIOGRAPHY
SUBHASISH DEB, BMCH
SUBHASISH DEB, BMCH
SUBHASISH DEB, BMCH

SUBHASISH DEB, BMCH
SUBHASISH DEB, BMCH
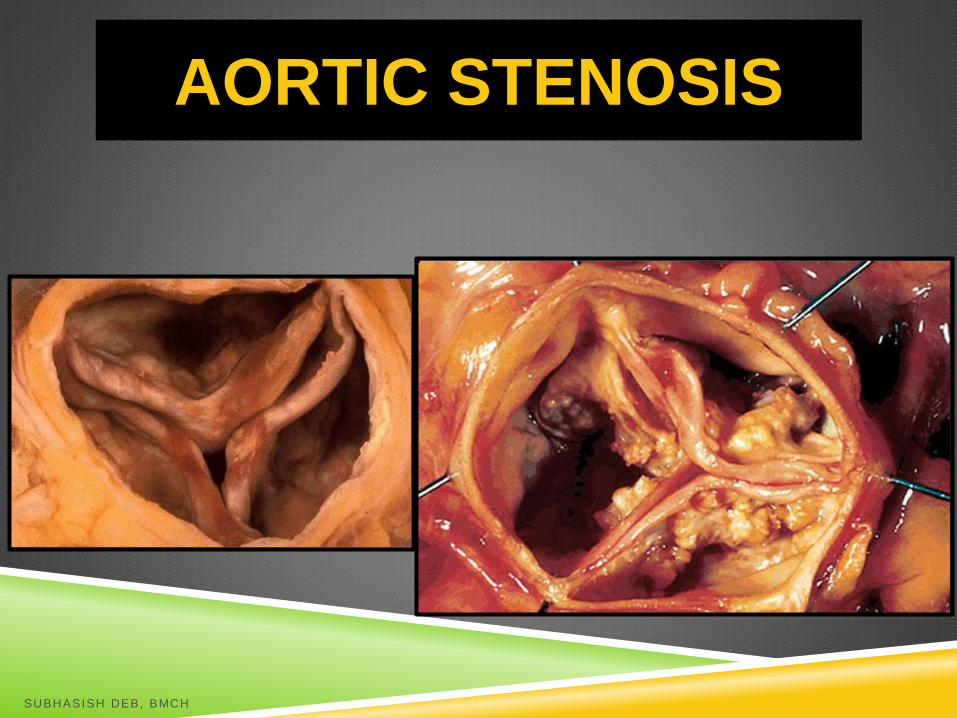
AORTIC STENOSIS
SUBHASISH DEB, BMCH
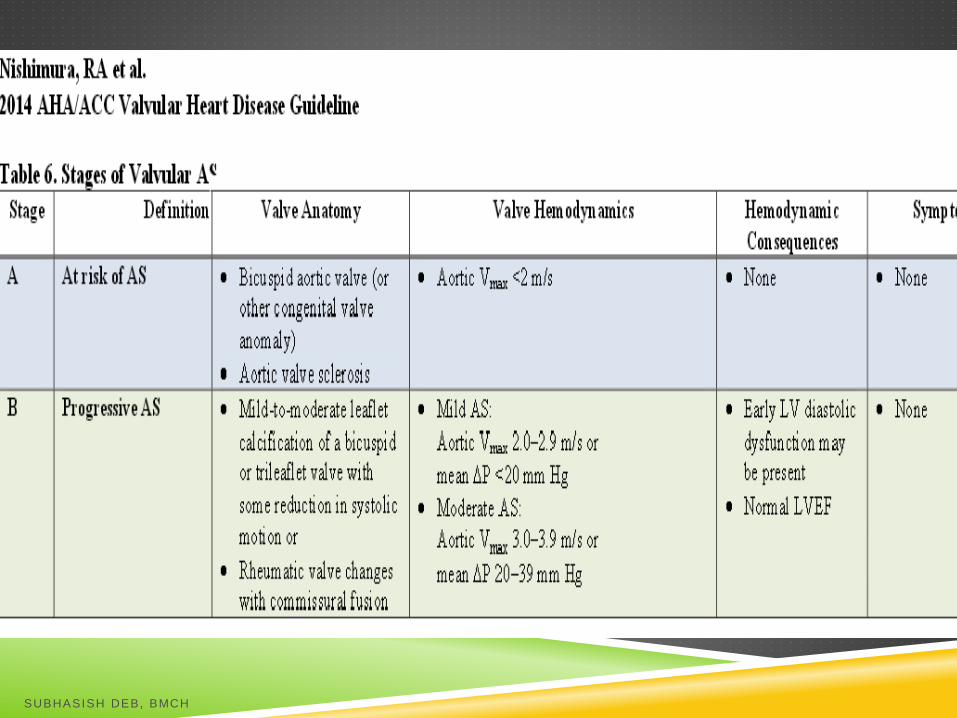
STAGES OF VALVULAR AS
Each of these stages are defined by:
1. Valve anatomy
2. Valve hemodynamics
3. The consequences of valve obstruction
on LT ventricle and vasculature
4. Patient symptoms
SUBHASISH DEB, BMCH
Hemodynamic severity is
best characterized by the
TRANSAORTIC MAXIMUM VELOCITY
Or
MEAN PRESSURE GRADIENT
SUBHASISH DEB, BMCH
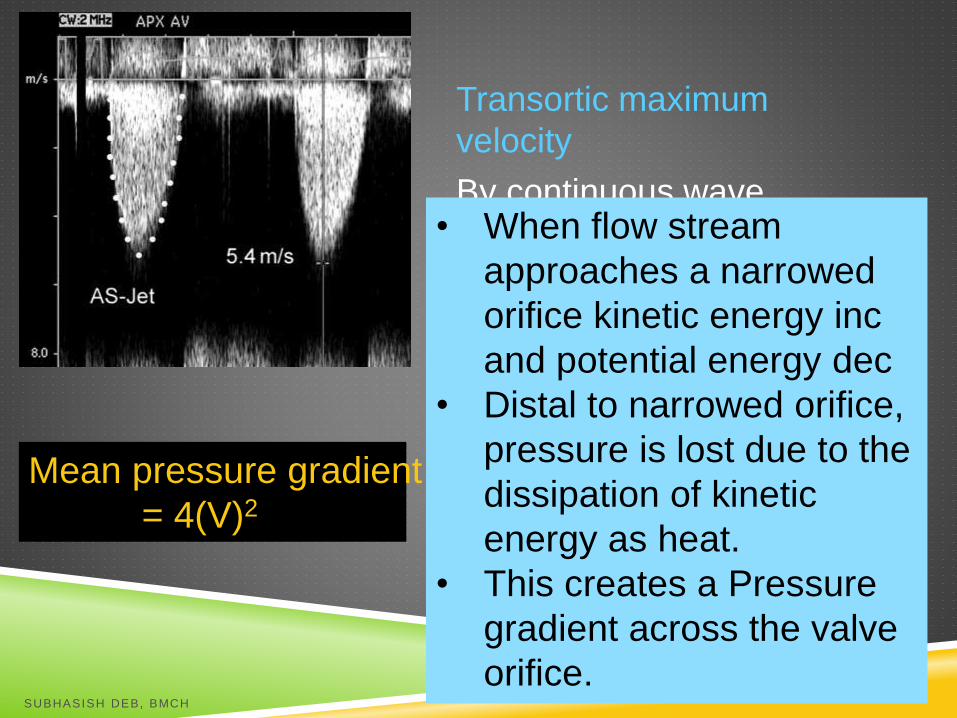
Transortic maximum
velocity
By continuous wave
doppler• When flow stream
approaches a narrowed
orifice kinetic energy inc
and potential energy dec
• Distal to narrowed orifice,
pressure is lost due to the
dissipation of kinetic
energy as heat.
• This creates a Pressure
gradient across the valve
orifice.
Mean pressure gradient
= 4(V)2
SUBHASISH DEB, BMCH
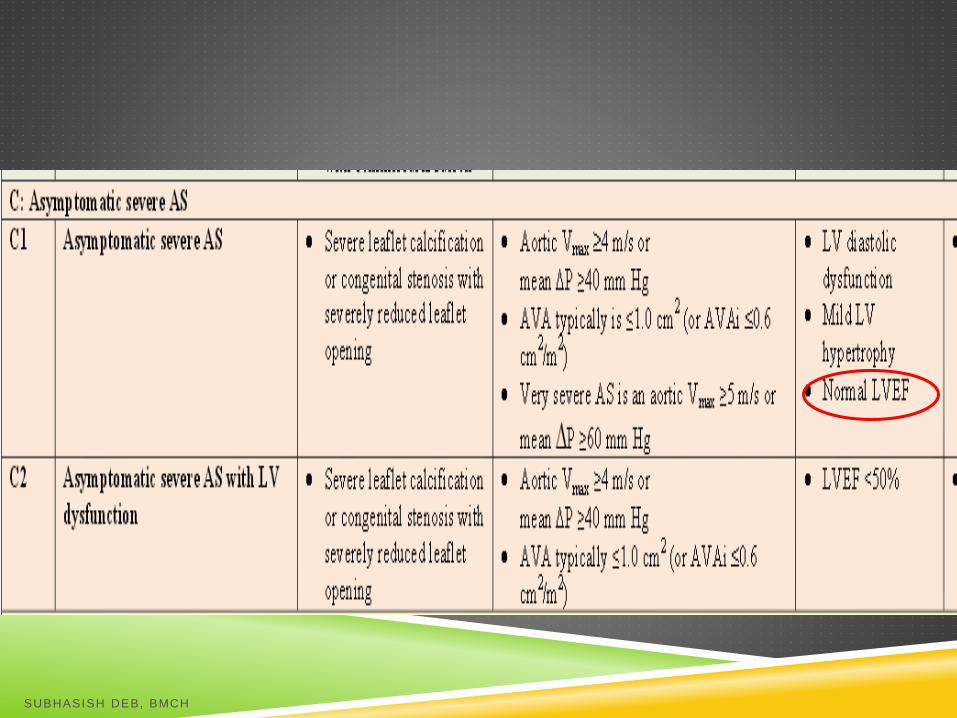
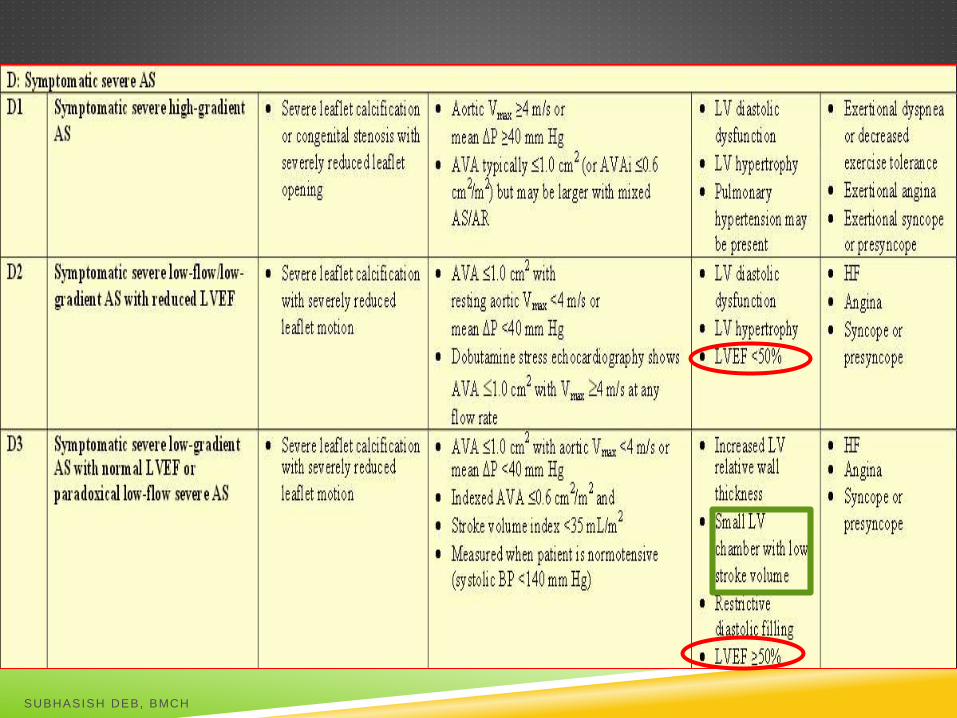
STAGING OF AS
SUBHASISH DEB, BMCH
SUBHASISH DEB, BMCH
SUBHASISH DEB, BMCH
AVAi – Aortic Valve Area Index:
Valve area should be indexed for body
surface area in smaller individuals so as to
not overestimate the severity of stenosis
based on valve area calculations.
SUBHASISH DEB, BMCH
SPECIAL SUB GROUPS
Some pts with AS have a low transaortic
volume flow rate due to either:
LV systolic dysfunction with a low LVEF
or
Small hypertrophied LV with low stroke
volume
Designated as
D2 (with low LVEF)
D3 (with normal LVEF)
SUBHASISH DEB, BMCH
SUBHASISH DEB, BMCH
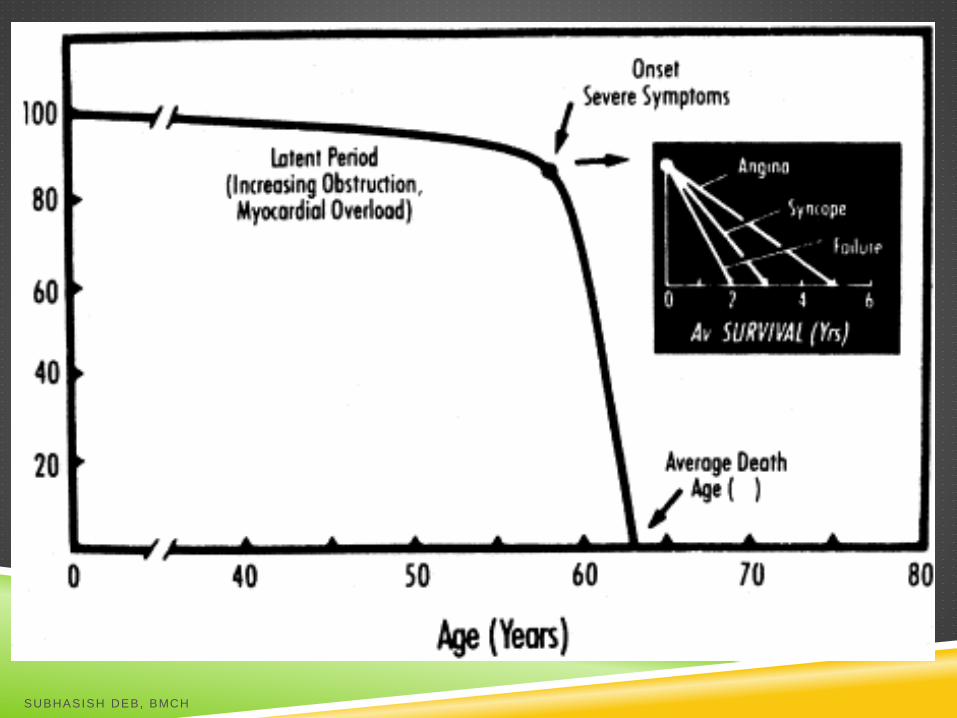
NATURAL H/O OF AS WITH
SYMPTOMS
Survival in AS declines abruptly with onset of symptoms.
50% with onset of agina - die in 5yrs
50% with onset of syncope - die in 3 yrs
50% with onset of CHF – die in 2 yrs
Circulation. 1968;38[suppl V]:V-61
SUBHASISH DEB, BMCH
SUBHASISH DEB, BMCH
The exact pathophysilogic
changes that produce the onset of
symptoms and begin this
rapid downhill course are
unknown
SUBHASISH DEB, BMCH
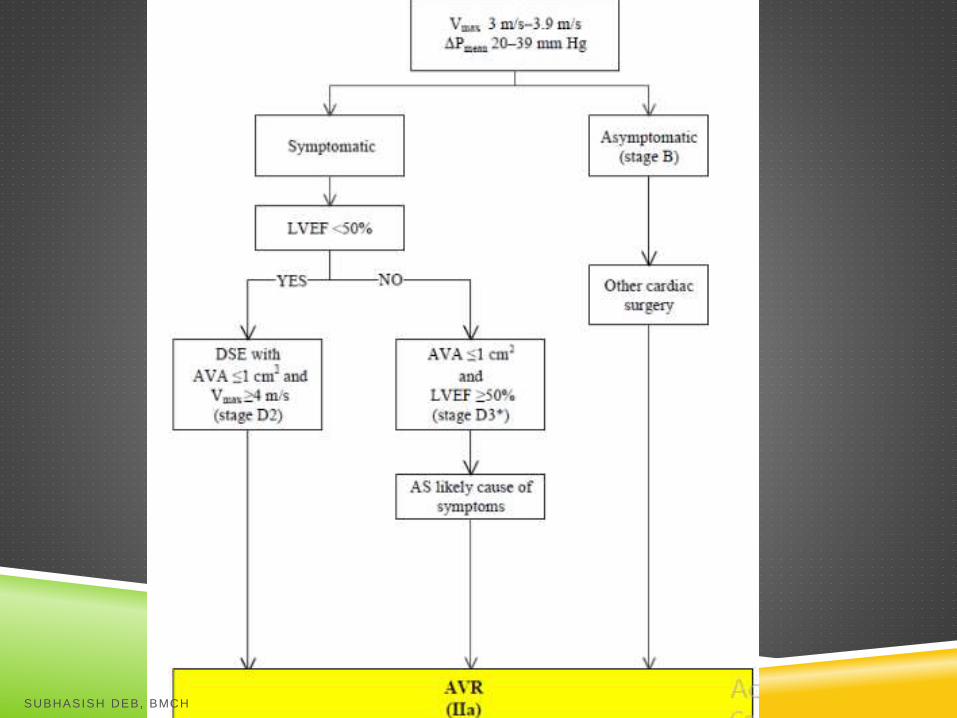
INDICATIONS FOR TIMING OF
INTERVNTION
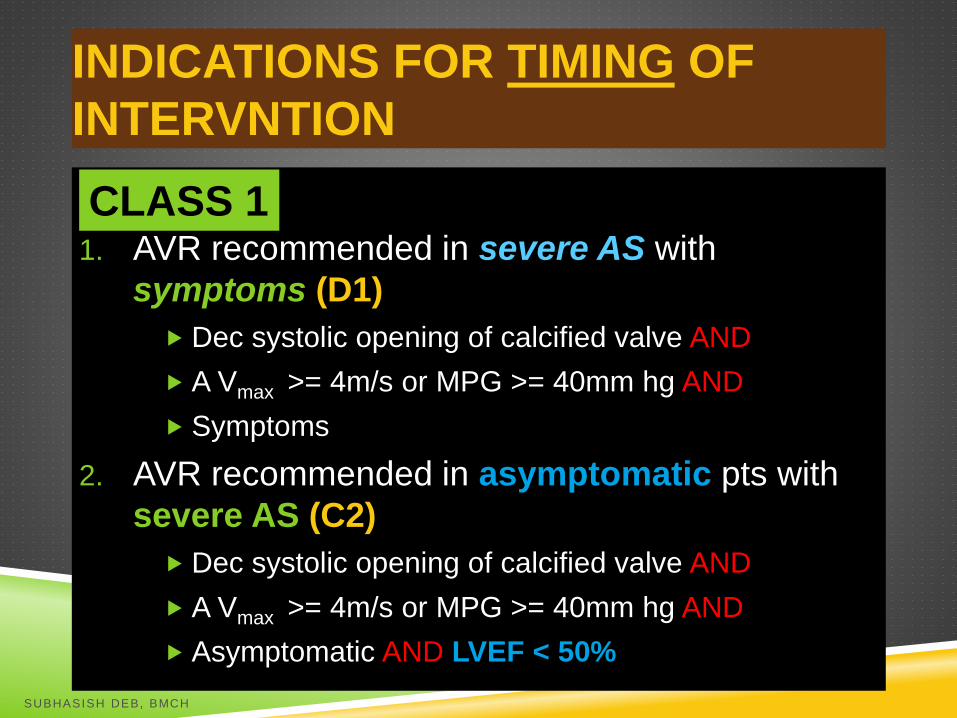
CLASS I :
1. AVR recommended in severe AS with
symptoms (D1)
Dec systolic opening of calcified valve AND
A Vmax >= 4m/s or MPG >= 40mm hg AND
Symptoms
2. AVR recommended in asymptomatic pts with
severe AS (C2)
Dec systolic opening of calcified valve AND
A Vmax >= 4m/s or MPG >= 40mm hg AND
Asymptomatic AND LVEF < 50%
CLASS 1
SUBHASISH DEB, BMCH
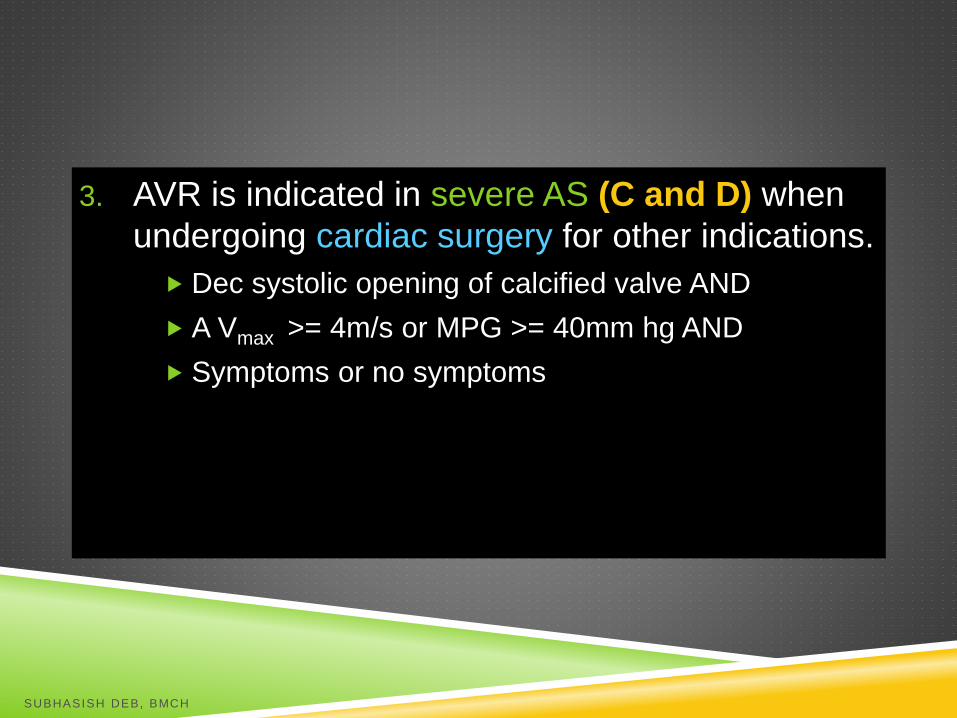
3. AVR is indicated in severe AS (C and D) when
undergoing cardiac surgery for other indications.
Dec systolic opening of calcified valve AND
A Vmax >= 4m/s or MPG >= 40mm hg AND
Symptoms or no symptoms
SUBHASISH DEB, BMCH
SUBHASISH DEB, BMCH
SUBHASISH DEB, BMCH
SUBHASISH DEB, BMCH
CHOICE OF TREATMENT
1. Aortic valve replacement (surgical)
2. Percutaneous Balloon Aortic valvuloplasty
Only in children and young adults with congenital,
non calcific AS
High restenosis rate in adults (80% in 1 yr)
Can be used as a “bridging operation” who are too ill
to tolerate surgery.
3. Transcatheter Aortic Valve Replacement
SUBHASISH DEB, BMCH
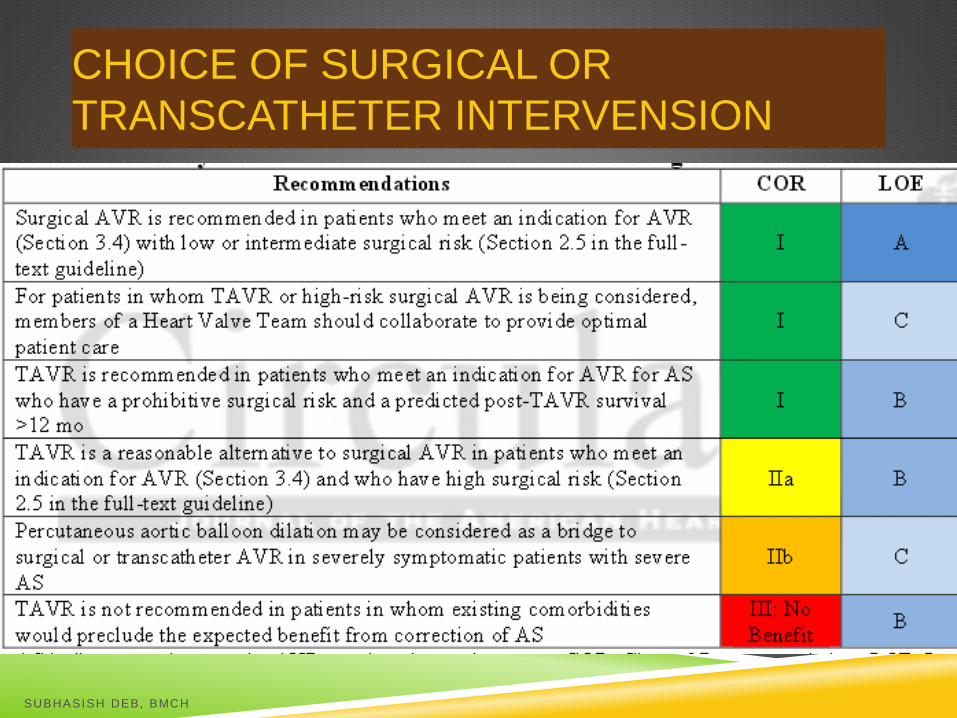
CHOICE OF SURGICAL OR
TRANSCATHETER INTERVENSION
SUBHASISH DEB, BMCH
TAVR
TAVI video
Dr Alain Criber Pioneered the 1st
transcathether aortic valve implatation
(TAVI) procedure 2002
SUBHASISH DEB, BMCH

Antegrade – Acute MR
Retrograde approaches
Transfemoral
Transapical
Transaortic
Two types of stent-vavle devices:
1. Balloon expandable valves (Edwards SAPIEN)
2. Self-expanding valves (Medtronic CoreValve)
SUBHASISH DEB, BMCH
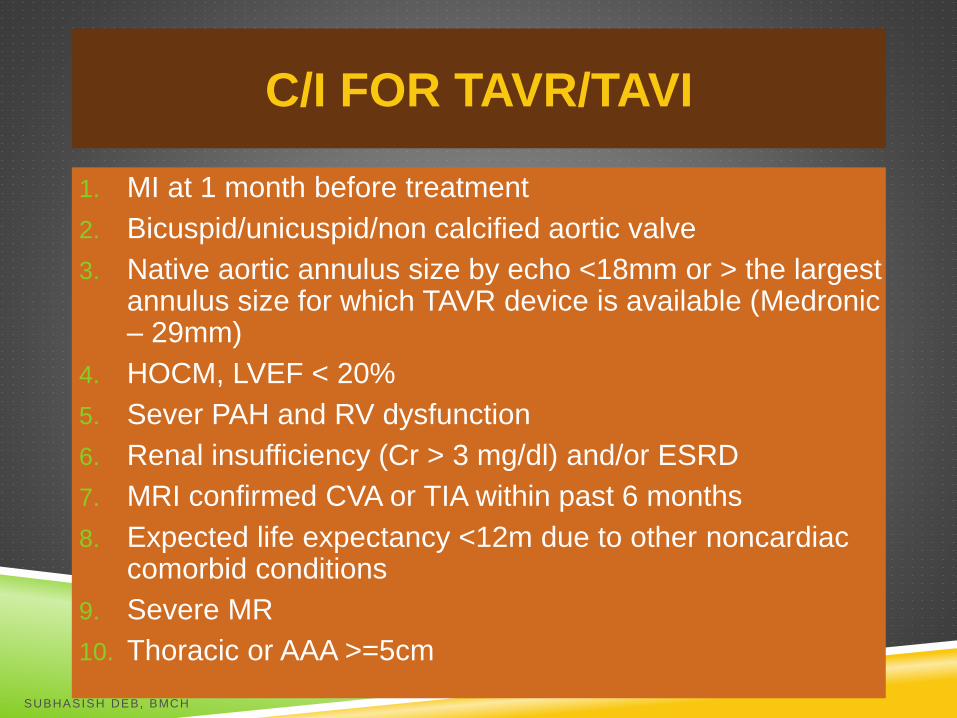
C/I FOR TAVR/TAVI
1. MI at 1 month before treatment
2. Bicuspid/unicuspid/non calcified aortic valve
3. Native aortic annulus size by echo <18mm or > the largest annulus size for which TAVR device is available (Medronic– 29mm)
4. HOCM, LVEF < 20%
5. Sever PAH and RV dysfunction
6. Renal insufficiency (Cr > 3 mg/dl) and/or ESRD
7. MRI confirmed CVA or TIA within past 6 months
8. Expected life expectancy <12m due to other noncardiaccomorbid conditions
9. Severe MR
10. Thoracic or AAA >=5cm
SUBHASISH DEB, BMCH
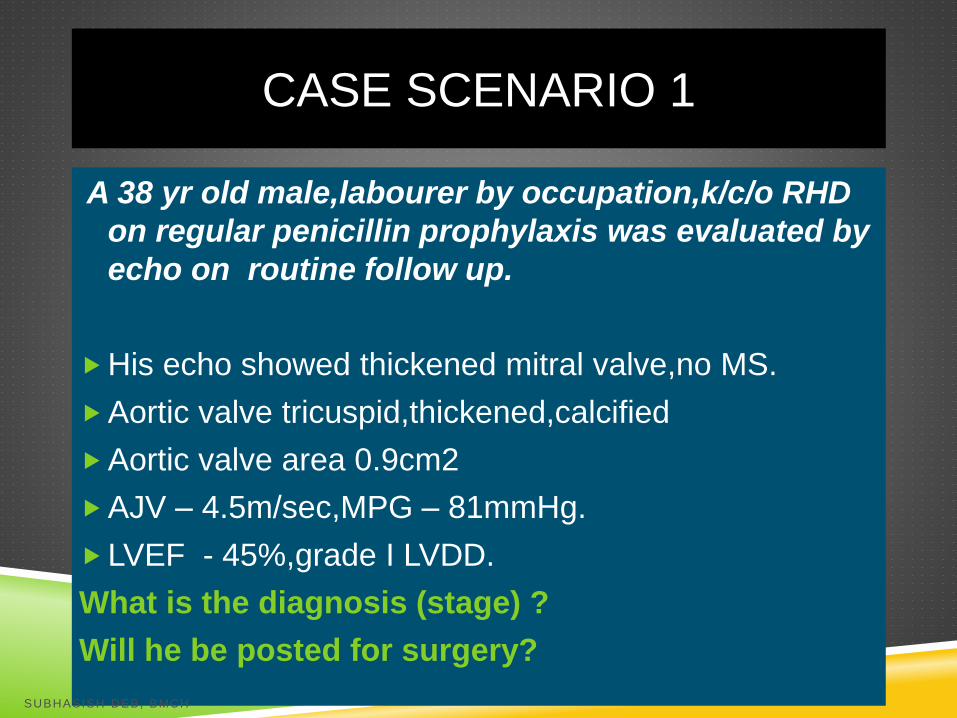
CASE SCENARIO 1
A 38 yr old male,labourer by occupation,k/c/o RHD
on regular penicillin prophylaxis was evaluated by
echo on routine follow up.
His echo showed thickened mitral valve,no MS.
Aortic valve tricuspid,thickened,calcified
Aortic valve area 0.9cm2
AJV – 4.5m/sec,MPG – 81mmHg.
LVEF - 45%,grade I LVDD.
What is the diagnosis (stage) ?
Will he be posted for surgery?
SUBHASISH DEB, BMCH
Severe Asympotmatic AS with LV
dysfunction (stage C2)
Take him for surgery
SUBHASISH DEB, BMCH
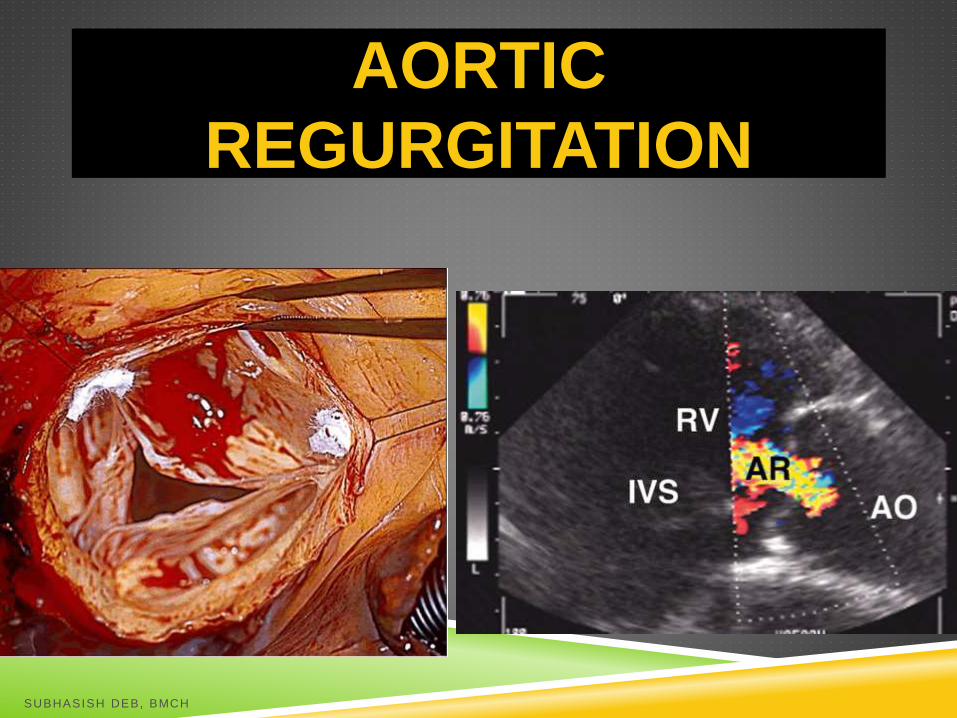
AORTIC
REGURGITATION
SUBHASISH DEB, BMCH
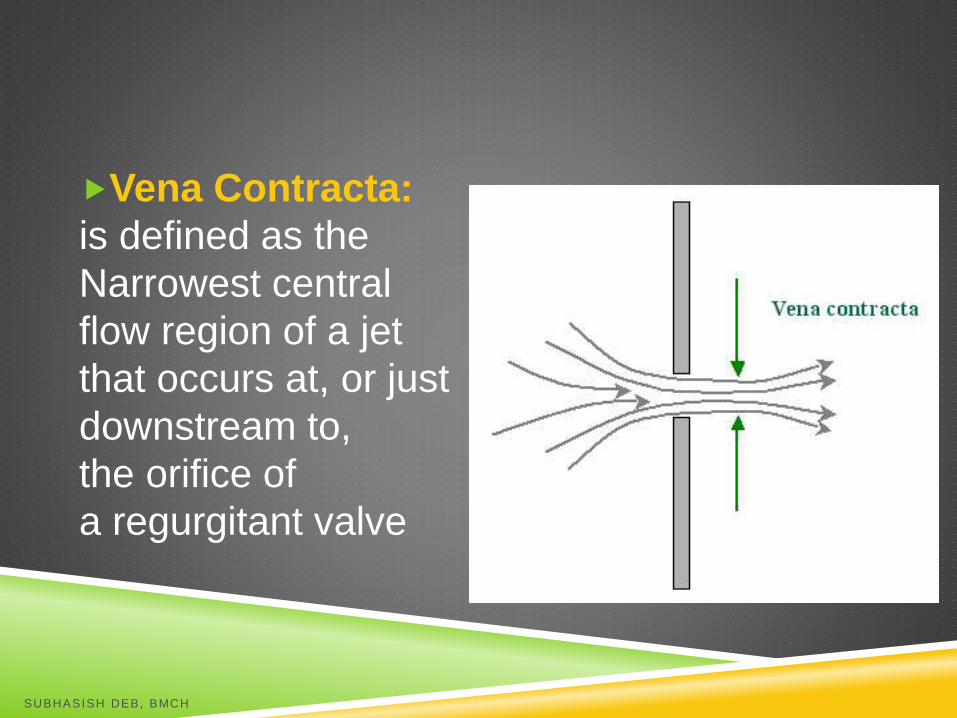
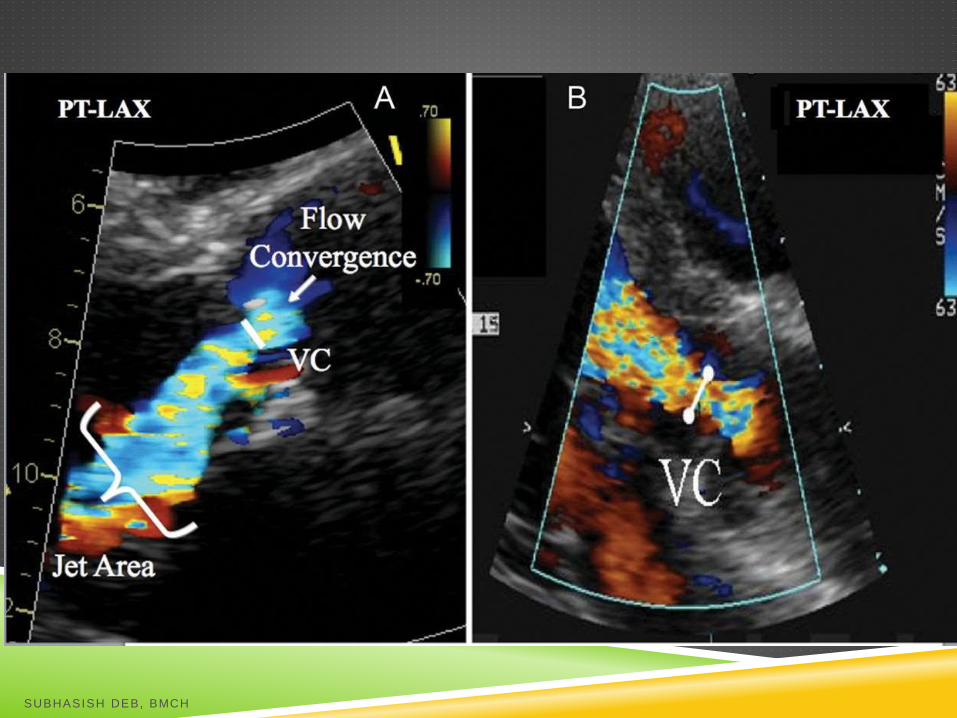
Vena Contracta:
is defined as the
Narrowest central
flow region of a jet
that occurs at, or just
downstream to,
the orifice of
a regurgitant valve
SUBHASISH DEB, BMCH
SUBHASISH DEB, BMCH
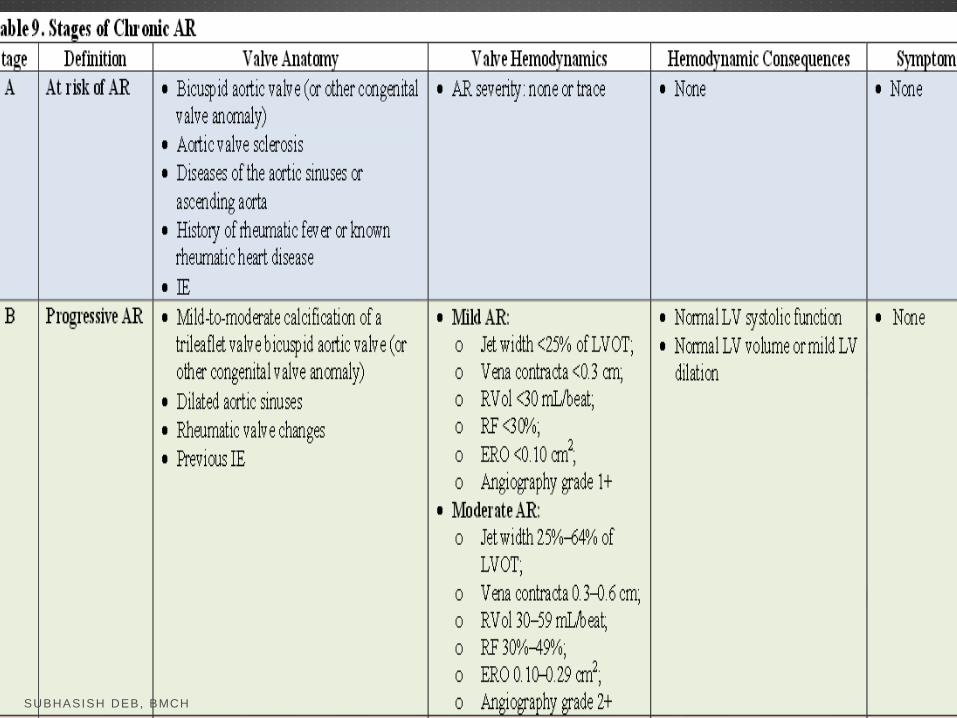
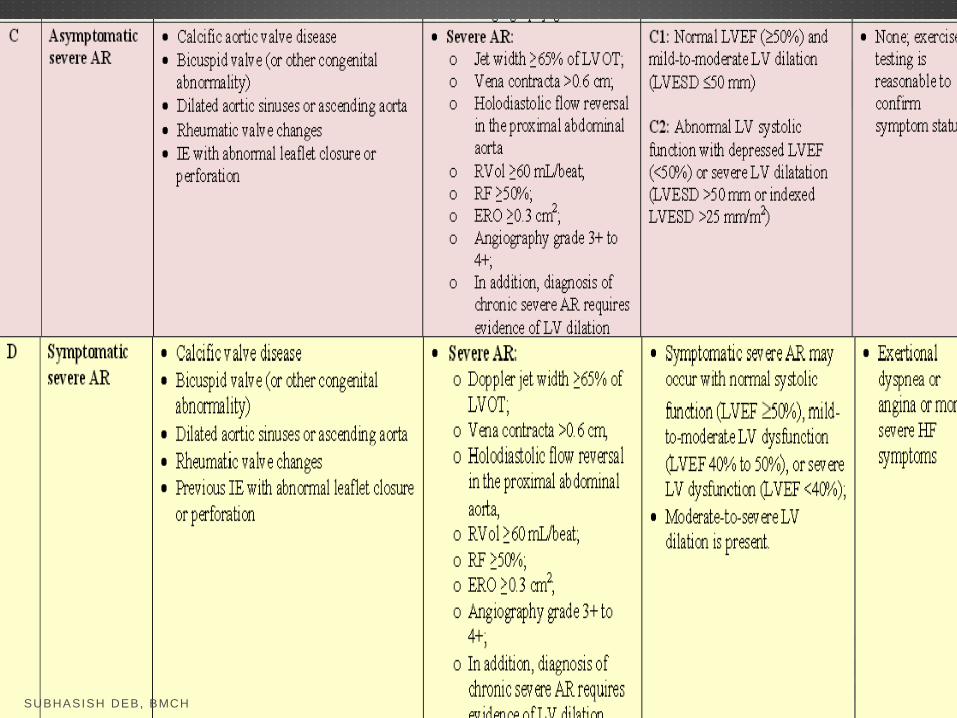
STAGING OF AR
SUBHASISH DEB, BMCH
SUBHASISH DEB, BMCH
SUBHASISH DEB, BMCH
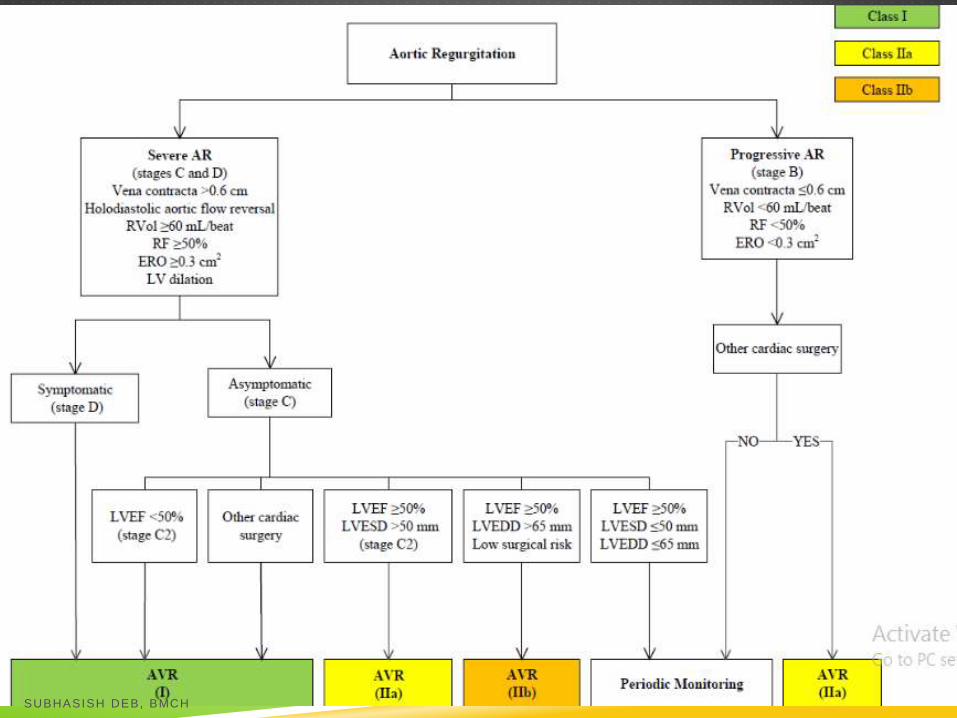
INTERVENTION IN AR
1. AVR indicated for SYMPTOMATIC pts with SEVERE AR regardless of LV systolic function. STAGE D
2. AVR indicated for ASYMTOMATIC pts with chronic SEVERE AR and LVEF < 50%. STAGE C2
3. AVR indicated for SEVER AR (STAGE C or D) while undergoing cardiac surgery for other indications.
CLASS 1
SUBHASISH DEB, BMCH
SUBHASISH DEB, BMCH
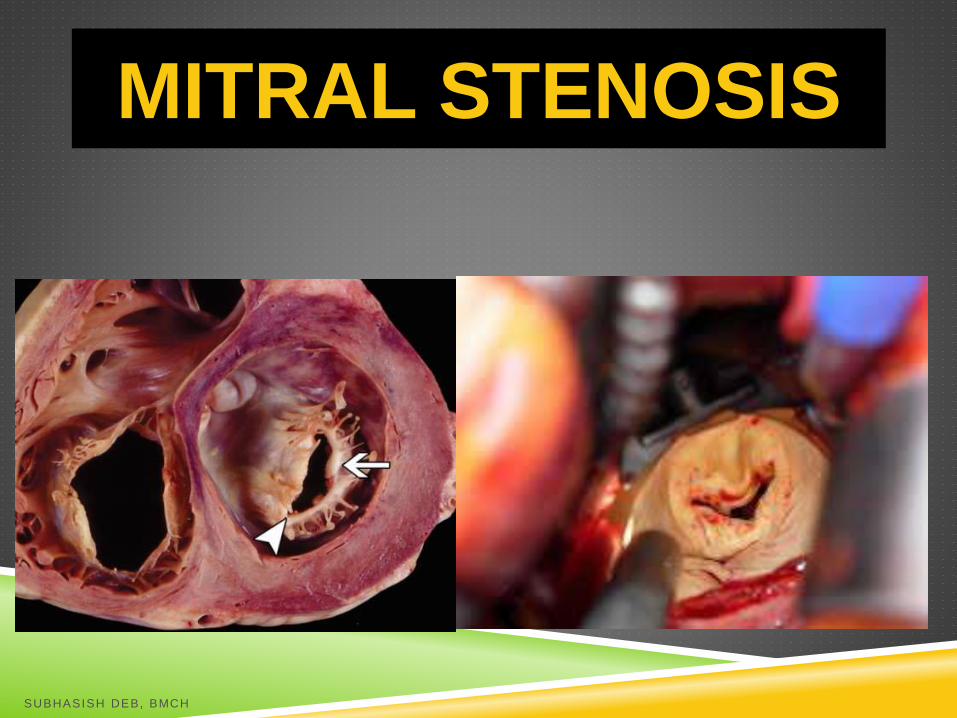
MITRAL STENOSIS
SUBHASISH DEB, BMCH
Diastolic pressure half time:
the time during diastole when the
transmitral gradient falls to 50% of initial
peak gradient.
More the DPHT, more sever the stenosis.
SUBHASISH DEB, BMCH
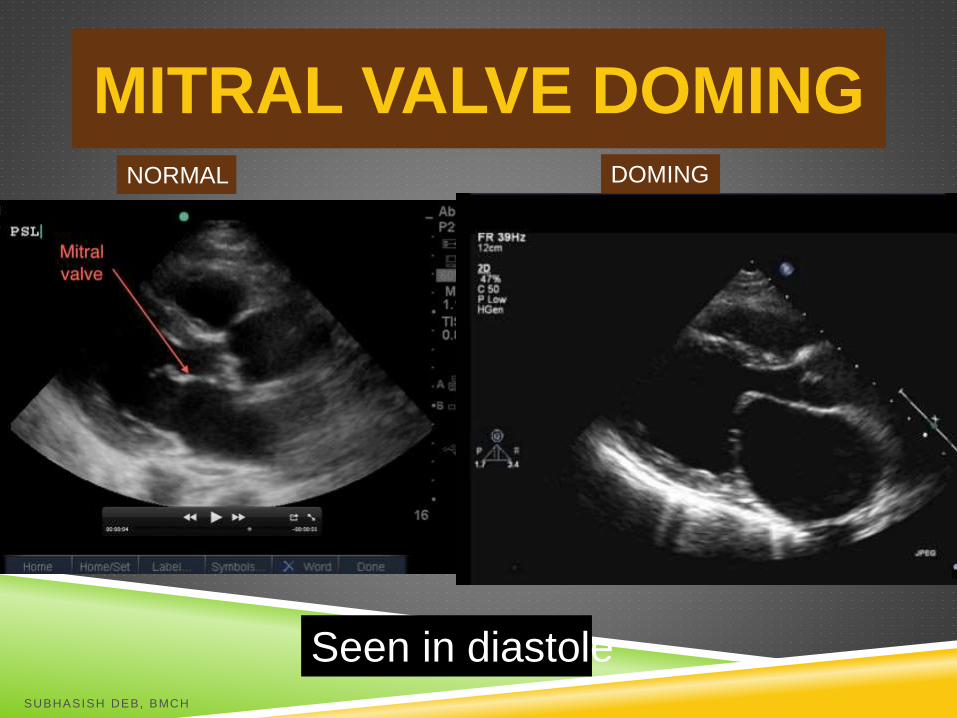
MITRAL VALVE DOMINGNORMAL DOMING
Seen in diastoleSUBHASISH DEB, BMCH
SUBHASISH DEB, BMCH
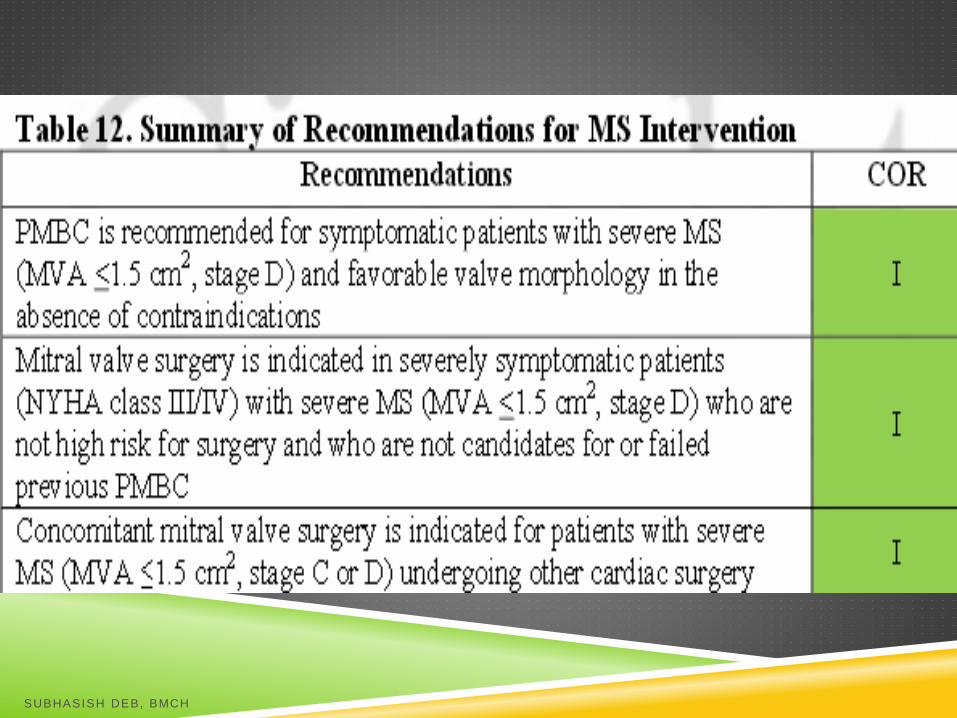
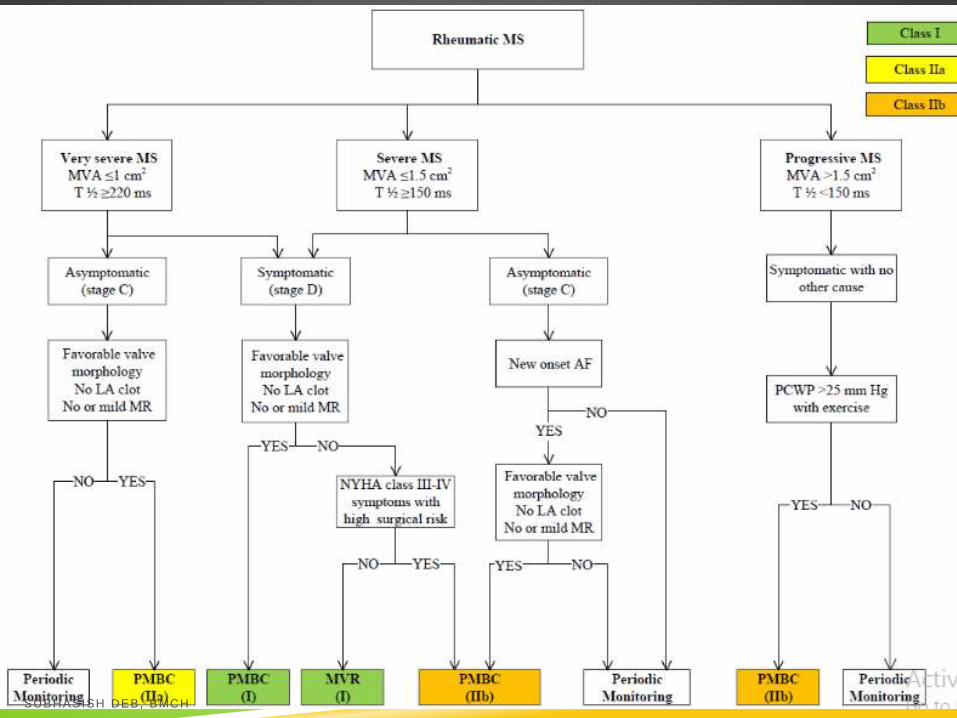
SEVERE MS – MVA < 1.5cm2
Transmitral pressure gradient > 5-10 mm
Hg at normal heart rate
Doppler Haemodynamics (apical 4 C
view) – peak and mean TVG averaged
from 2-5 beats in SR and 5-10 beats in
AF
SUBHASISH DEB, BMCH
SUBHASISH DEB, BMCH
SUBHASISH DEB, BMCH
MITRAL
REGURGITATION
SUBHASISH DEB, BMCH
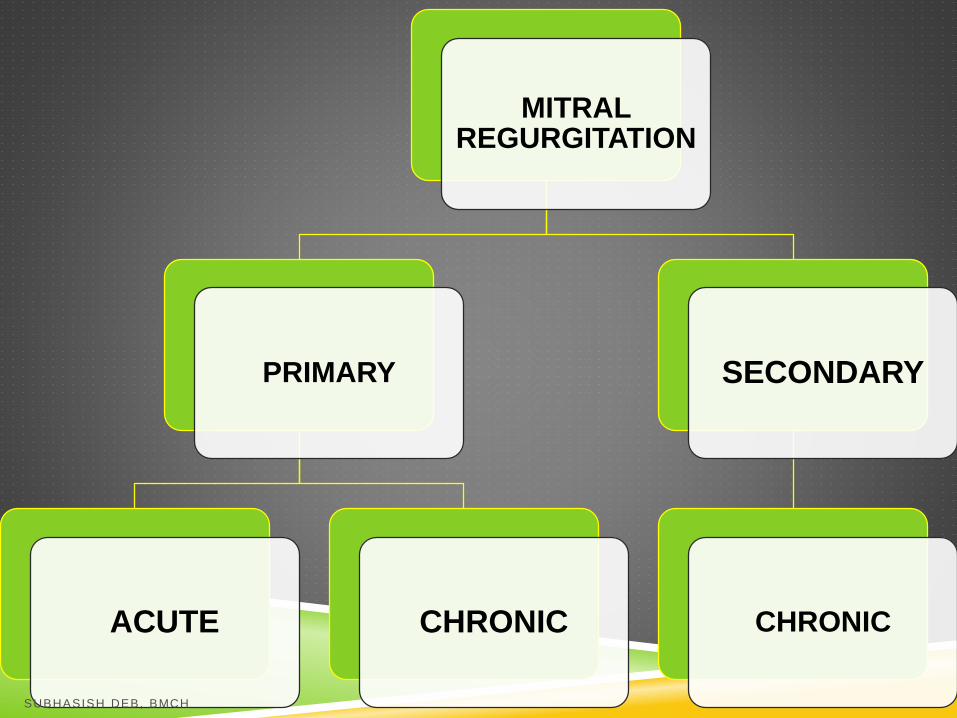
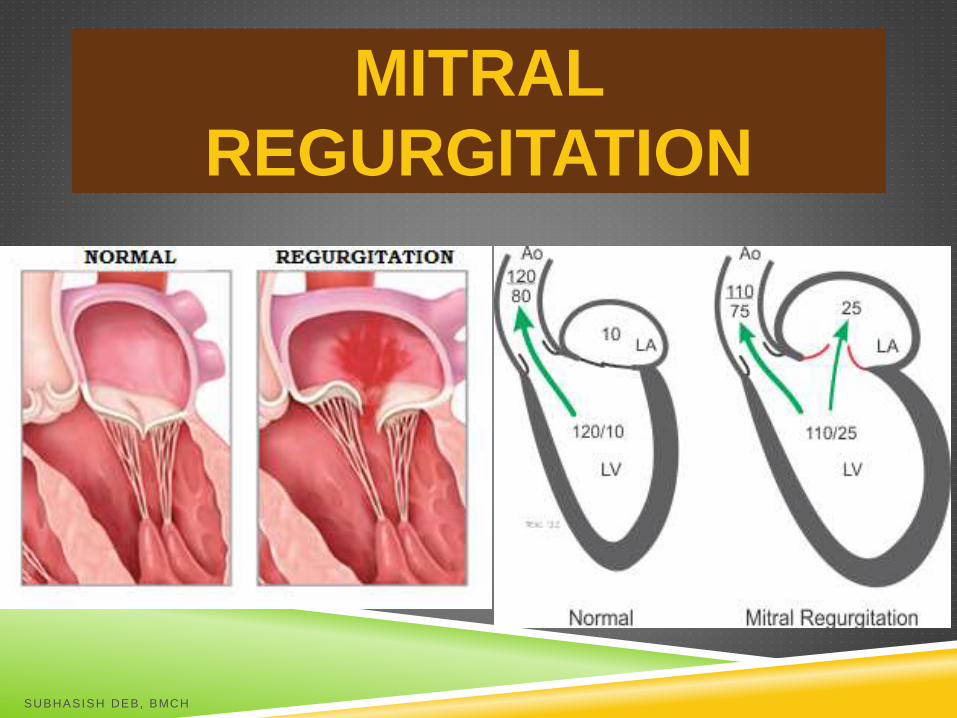
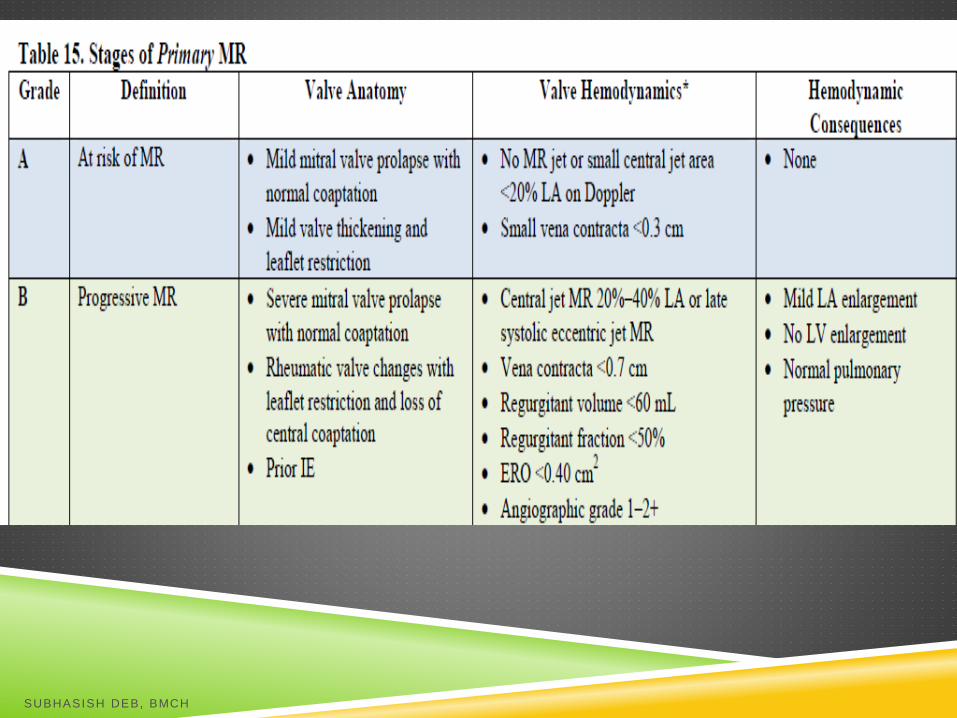
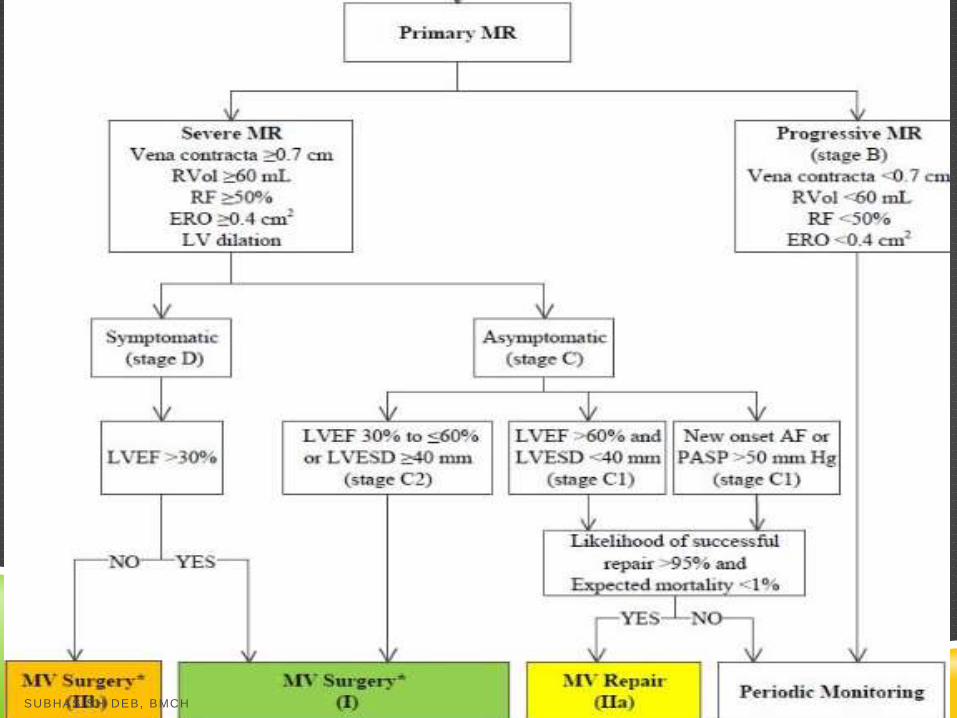
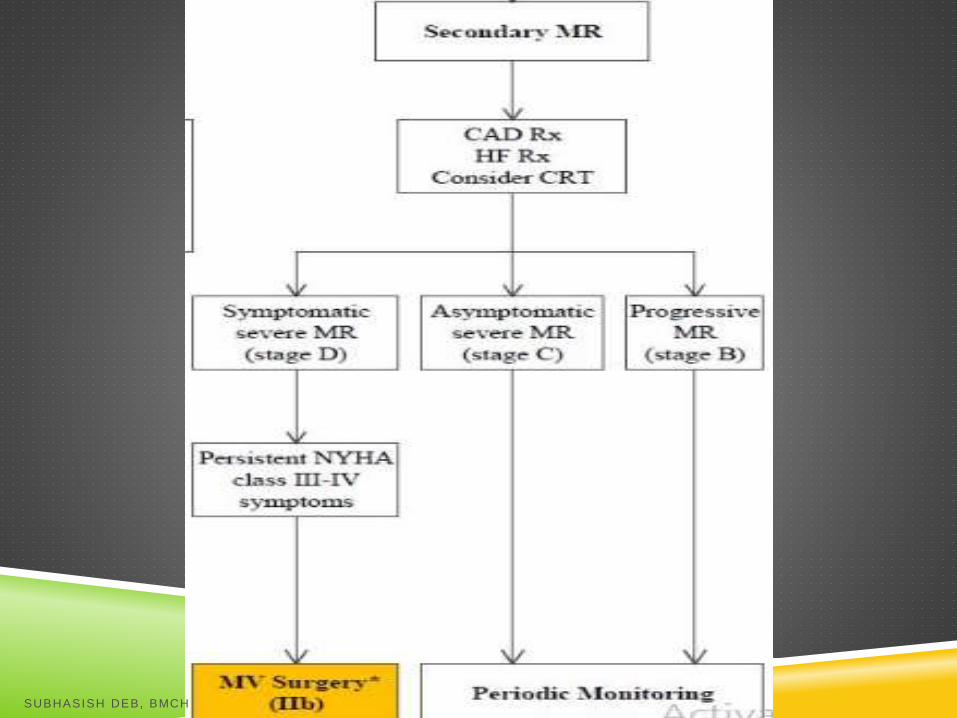
MITRAL REGURGITATION
PRIMARY
ACUTE CHRONIC
SECONDARY
CHRONIC
SUBHASISH DEB, BMCH
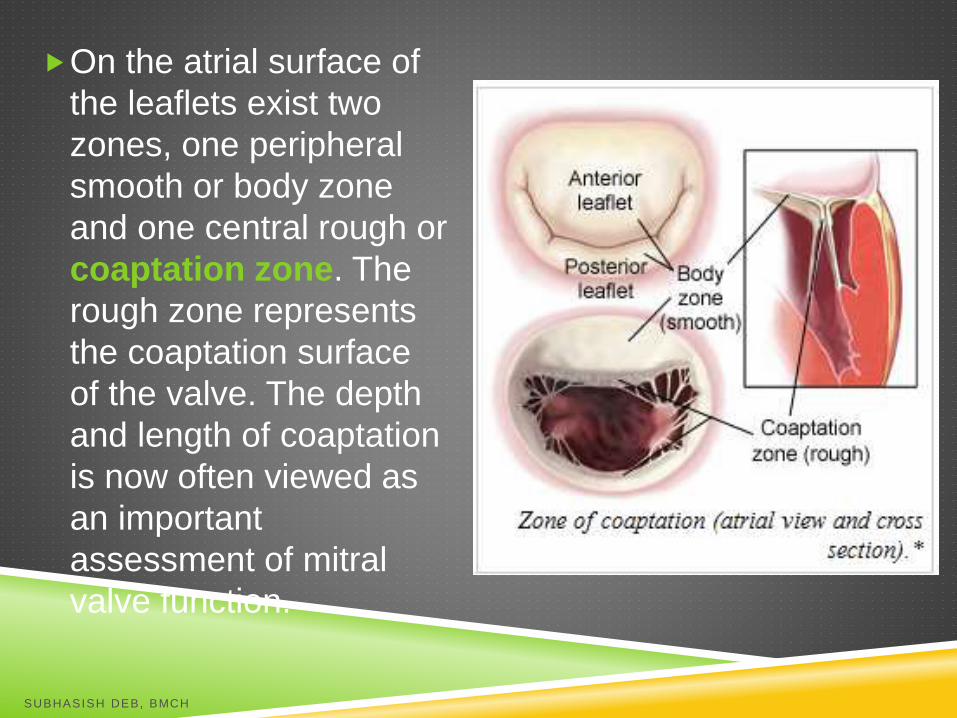
On the atrial surface of
the leaflets exist two
zones, one peripheral
smooth or body zone
and one central rough or
coaptation zone. The
rough zone represents
the coaptation surface
of the valve. The depth
and length of coaptation
is now often viewed as
an important
assessment of mitral
valve function.
SUBHASISH DEB, BMCH
SUBHASISH DEB, BMCH
SUBHASISH DEB, BMCH
SUBHASISH DEB, BMCH
SUBHASISH DEB, BMCH
SUBHASISH DEB, BMCH
MITRAL CLIP
In October 2013, the FDA approved the MitraClip valve
repair system for patients with symptomatic
degenerative MR with a prohibitive risk for mitral-valve
surgery. Approval was based on registry data and the
Endovascular Valve Edge-to-Edge Repair Study
(EVEREST II), in which percutaneous repair of the
mitral valve was less effective in reducing MR but was
associated with similar improvement in clinical
outcomes and with superior safety
SUBHASISH DEB, BMCH
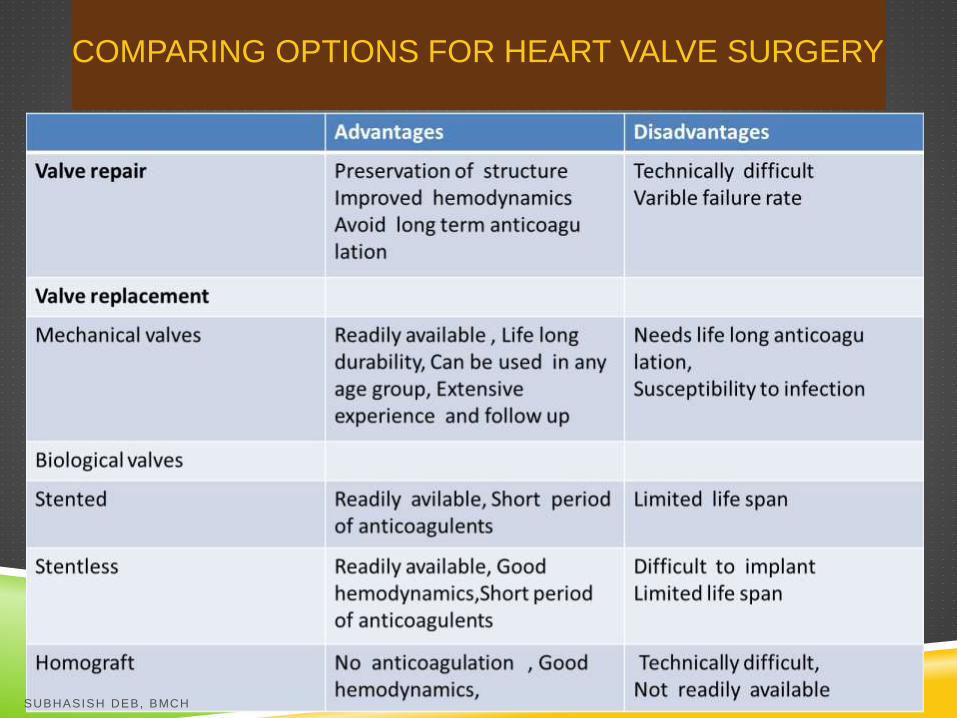
COMPARING OPTIONS FOR HEART VALVE SURGERY
SUBHASISH DEB, BMCH
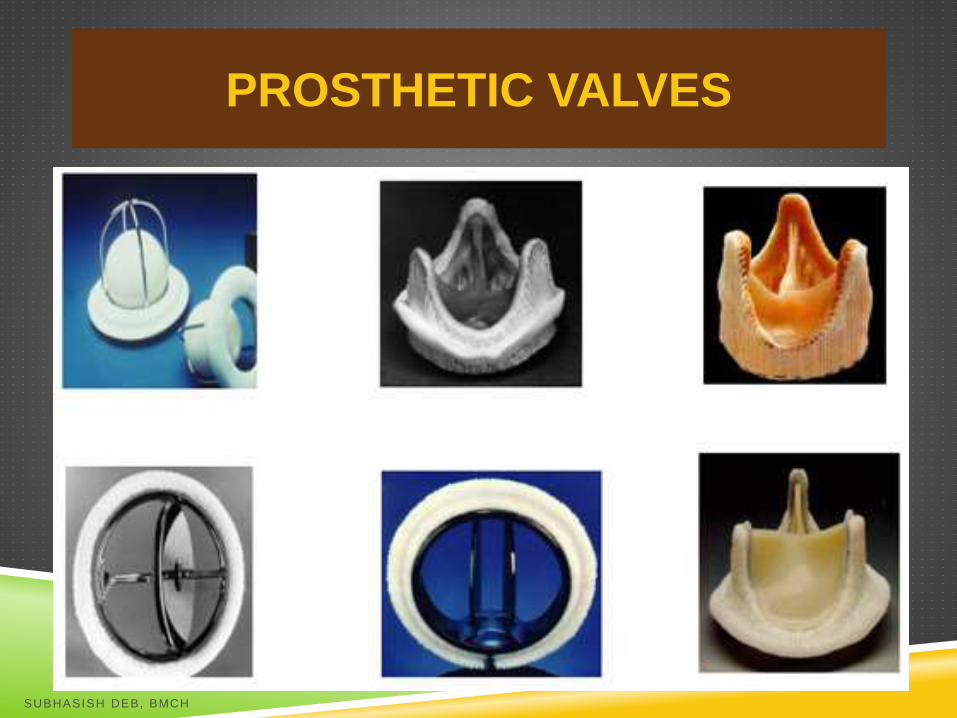
PROSTHETIC VALVES
SUBHASISH DEB, BMCH
TYPES OF PROSTHETIC VALVES
Mechanical valves-
A. Ball and Cage valve- first generaion valves . A
spherical occuluder ( barium coated silastic ball)
is retained within a metal cage Starr Edwards
valve belonged to this class
B.Tilting disc valve- The best known examples
are Bjork –Shiley model ( now withdrawn) and
TTK valve (Indian).It has single disc which is
restrained by struts
C.Bileaflet valve- It has two cusps (disc
occuluders) in a sewing ring .St Jude medical
valve is the best example. SUBHASISH DEB, BMCH
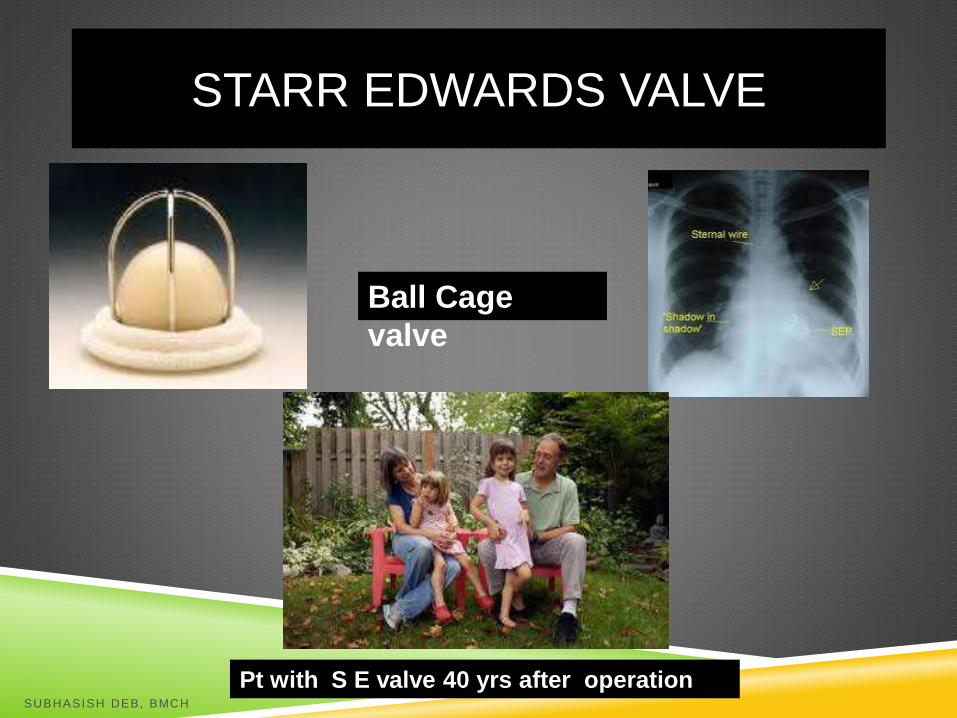
STARR EDWARDS VALVE
Ball Cage
valve
Pt with S E valve 40 yrs after operationSUBHASISH DEB, BMCH

PROSTHETIC VALVES (MECHANICAL)
SREE CHITRA TTK VALVE (PRIDE OF
INDIA)
Tilting Disc
valve
SUBHASISH DEB, BMCH

BILEAFLET VALVES
SUBHASISH DEB, BMCH
TYPES OF PROSTHETIC VALVES
Biological valves-
a.Autograft –Pulmonary valve of pt is removed and
put in aortic position and replacing pulmonary valve
with aortic homograft ( Ross procedure ). It is
technically demanding operation
b.Homograft or allogaft –removed from cadavers,
antibiotic sterlised,cryo preserved.
C.Heterograft or xenograft- from animal tissue like
glutaraldehyde treated porcine (pig valves) mounted
on stents.
Homo and Heterografts are indicated in pts over 60
yrs age or where anticoagulants are contraindicated (
bleeding diathesis, uncontroled hypertension , GIT
ulcers etc) SUBHASISH DEB, BMCH
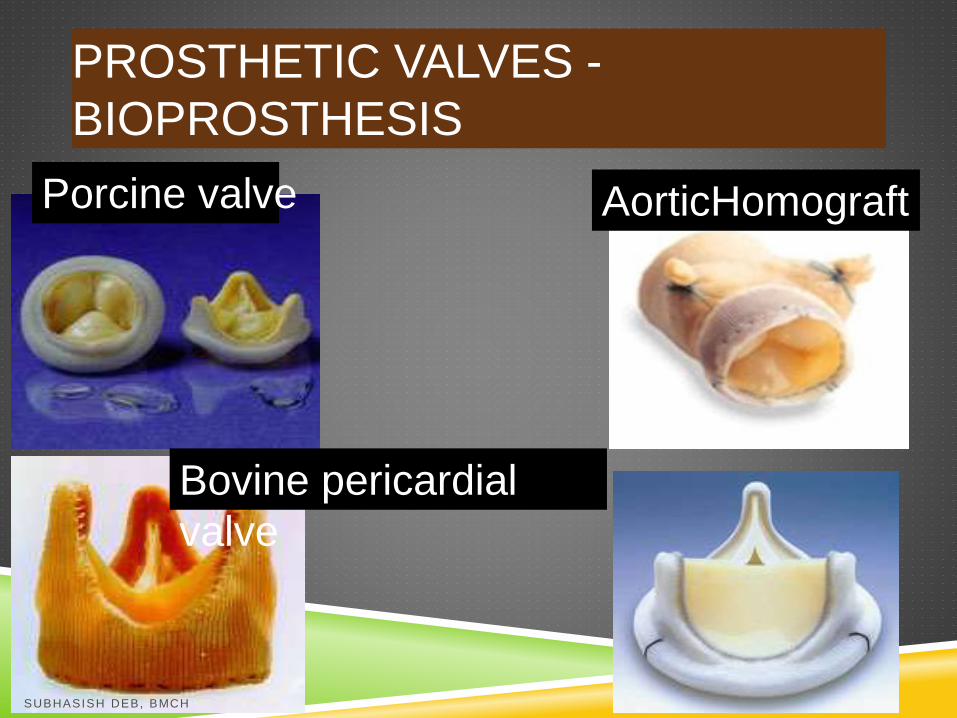
PROSTHETIC VALVES -
BIOPROSTHESIS
Bovine pericardial
valve
AorticHomograftPorcine valve
SUBHASISH DEB, BMCH
SUBHASISH DEB, BMCH

SUBHASISH DEB, BMCH





























