Embed Size (px)
Citation preview

DR. SHERIF ALY DR. SHERIF ALY Consultant (A) Nephrology
Assir central hospital Abha 10/10/10

OBJECTIVESOBJECTIVES : :
Introduction Concept of AKIIntroduction Concept of AKI Introducing RIFIE and AKIN staging Introducing RIFIE and AKIN staging
criteria for AKIcriteria for AKI Describe the need for Biomarkers in AKIDescribe the need for Biomarkers in AKI Describe the role of Biomarkers in AKIDescribe the role of Biomarkers in AKI Discuss examples of promising AKI Discuss examples of promising AKI
biomarkersbiomarkers Discuss pharmacological treatment of Discuss pharmacological treatment of
AKIAKI Discuss new anticoagulantsDiscuss new anticoagulants


IntroductionIntroductionA. ) A. ) AKI Versus ARFAKI Versus ARF- AKI reflects the entire spectrum of the disease and AKI reflects the entire spectrum of the disease and
recognizes that acute decline in kidney function is often recognizes that acute decline in kidney function is often secondary to an injury that causes functional or structural secondary to an injury that causes functional or structural changes in the kidneychanges in the kidney
B.) B.) HistoryHistory
- In 2002 , ADQI proposed RIFLE classification system- In 2002 , ADQI proposed RIFLE classification system
- Categorizes and stratifies a population of patients based - Categorizes and stratifies a population of patients based on their renal function.on their renal function.
- Three severity categories : - Three severity categories : RISKRISK , , INJURYINJURY & & FAILUREFAILURE
- Two outcome categories : - Two outcome categories : LOSSLOSS & & END-STAGE DISEASEEND-STAGE DISEASE
- In 2004 Acute Kidney Injury Network (AKIN) formed- In 2004 Acute Kidney Injury Network (AKIN) formed
- Prposed a diagnostic criteria for the definition of AKI- Prposed a diagnostic criteria for the definition of AKI
- In 2004 ADQI , ISN and ASN met and proposed the term of - In 2004 ADQI , ISN and ASN met and proposed the term of AKI.AKI.

AKI : A Common Serious AKI : A Common Serious ProblemProblem
AKI is present in 5% of all hospitalized AKI is present in 5% of all hospitalized patients , and up to 30% of patients in patients , and up to 30% of patients in ICUs.ICUs.
The incidence is increasing at an The incidence is increasing at an alarming rate.alarming rate.
Mortality rate > 50% in dialyzed ICU Mortality rate > 50% in dialyzed ICU patients.patients.
25% of ICU dialysis survivors progress 25% of ICU dialysis survivors progress to ESRD within 3 years.to ESRD within 3 years.

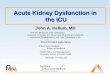
Green bars are unadjusted, blue bars are age and gender adjusted, and gray bars are multivariable adjusted. Multivariable analyses adjusted for age, gender, diagnosis-related group (DRG) weight, CKD status, and ICD-9-CM codes for respiratory, gastrointestinal, malignant, and infectious diseases; n = 1564, 885, 246, and 105 for change in SCr 0.3 to 0.4, 0.5 to 0.9, 1.0 to 1.9, and 2.0 mg/dl.
Chertow et al, JASN 2005
The Effect of AKI on The Effect of AKI on MortalityMortality

The Effects of AKI on The Effects of AKI on Hospital CostsHospital Costs
Green bars are unadjusted, blue bars are age and gender adjusted, and gray bars aremultivariable adjusted. Multivariable analyses adjusted for age, gender, diagnosis-related group (DRG) weight, CKD status, and ICD-9-CM codes for respiratory, GI, malignant, and infectious diseases; n = 1564, 885, 246, and 105 for change in SCr 0.3 to 0.4, 0.5 to 0.9, 1.0 to 1.9, and 2.0 mg/dl.
Chertow et al, JASN 2005

AKI Definition and Staging AKI Definition and Staging AKIN 2007AKIN 2007
* * An abrupt (within 48 hrs) reduction in An abrupt (within 48 hrs) reduction in kidney function defined as an kidney function defined as an absolute increase in serum creatinine absolute increase in serum creatinine level of ≥ 26.4 Mmol/L (0.3mg1dl) level of ≥ 26.4 Mmol/L (0.3mg1dl) oror a percentage increase in serum a percentage increase in serum creatinine level of ≥ 50% (1.5 fold creatinine level of ≥ 50% (1.5 fold from base line) from base line) or or a reduction in a reduction in urine output (documented oligurea of urine output (documented oligurea of < 0.5 ml/kg/ hr for > 6 hrs.)< 0.5 ml/kg/ hr for > 6 hrs.)

Acute Kidney Injury Network (AKIN) Acute Kidney Injury Network (AKIN) Staging SystemStaging System
for Acute Renal Failure for Acute Renal FailureModifiable RIFLE CriteriaModifiable RIFLE Criteria
AKIN StageAKIN Stage Serum Creatinine CriteriaSerum Creatinine Criteria UOPUOP
1)1) RiskRisk ↑↑S. Creat ≥ 26.4 Mmol/L S. Creat ≥ 26.4 Mmol/L or 50-100% above base or 50-100% above base lineline
< 0.5 < 0.5 ml/kg/mml/kg/m22
for > 6 hoursfor > 6 hours
2)2) InjuryInjury Increase of 2-3 folds over Increase of 2-3 folds over base linebase line
< 0.5 < 0.5 ml/kg/mml/kg/m22
for > 12 for > 12 hourshours
3)3) FailureFailure Increase of > 3 folds over Increase of > 3 folds over base line or S. Creat > base line or S. Creat > 354 Mmol/L acute increase 354 Mmol/L acute increase of at least 0.5 mg/dl (44 of at least 0.5 mg/dl (44 Mmol/L)Mmol/L)
Need RRTNeed RRT
< 0.5 < 0.5 ml/kg/mml/kg/m22
for > 24 for > 24 hourshours

Progression of Early Kidney Progression of Early Kidney DiseaseDisease
Hosle EAJ , etal Crit care 2006 , 10 : R 73Hosle EAJ , etal Crit care 2006 , 10 : R 73

Conceptual Model for AKI
NormalIncreased
riskDamage
↓GFR
Kidney Failure
Death

Mechanism of Ischemic Mechanism of Ischemic Acute Kidney InjuryAcute Kidney Injury
1)1) Tubular cell metabolismTubular cell metabolism
2)2) Tubular cell structureTubular cell structure
3)3) Microvasculature and Microvasculature and inflammationinflammation



PerioPeriodd
Acute Myocardial Acute Myocardial InfarctionInfarction
Acute Kidney Acute Kidney InjuryInjury
1960s1960s LDHLDH Serum creatinineSerum creatinine
1970s1970s CPK, myoglobinCPK, myoglobin Serum creatinineSerum creatinine
1980s1980s CK-MBCK-MB Serum creatinineSerum creatinine
1990s1990s Troponin TTroponin T Serum creatinineSerum creatinine
2000s2000s Troponin ITroponin I Serum creatinineSerum creatinine
Multiple Therapies
50% ↓ Mortality
Supportive CareHigh
MortalityNeed early biomarkers of AKI for improved understanding, early treatment and better
outcomes
Biomarkers: AMI versus AKIBiomarkers: AMI versus AKI

What is wrong with Serum What is wrong with Serum Creatinine?Creatinine?
The production of creatinine is highly The production of creatinine is highly variable (age, sex, muscle mass)variable (age, sex, muscle mass)
Serum creatinine may not show significant Serum creatinine may not show significant increased until 50% of kidney function is increased until 50% of kidney function is lost.lost.
Does not depict real-time changes in GFR Does not depict real-time changes in GFR that occur with acute reduction in kidney that occur with acute reduction in kidney function.function.
Require time to accumulate to prior to Require time to accumulate to prior to being detected.being detected.

The Ideal Biomaker of AKIThe Ideal Biomaker of AKI
Easy, rapid and inexpensive to Easy, rapid and inexpensive to measure.measure.
Precise and reliablePrecise and reliable Highly sensitive for AKI.Highly sensitive for AKI. It should be able to monitor the It should be able to monitor the
injury and predicts the severity.injury and predicts the severity. It should be specific.It should be specific.

Serum and Urinary Biomakers for AKI
SG Coca etal kid. International 2008 73 , 1008 -1016

Validity Criterion Validity Criterion Explanation Explanation Scoring Scoring Comments Comments
Participant recruitmentParticipant recruitmentWas recruitment based on presenting symptoms, results from Was recruitment based on presenting symptoms, results from previous tests, or fact that participants received index tests?previous tests, or fact that participants received index tests?
Presenting sx=1Presenting sx=1Previous tests or Previous tests or index tests=0index tests=0
Based on presenting symptoms in all 31 studies.Based on presenting symptoms in all 31 studies.
Participant samplingParticipant samplingWas it study population or a convenience sample or a consecutive Was it study population or a convenience sample or a consecutive series?series?
Consecutive series=1Consecutive series=1Convenience Convenience sample=0sample=0
Based on convenience sample in 5Based on convenience sample in 510, 19, 20, 22, 25, 3710, 19, 20, 22, 25, 37 studies. studies.
Data collectionData collectionWas data collection planned before the index test and reference Was data collection planned before the index test and reference standard were performed prospectively or retrospectively?standard were performed prospectively or retrospectively?
Prospective=1Prospective=1Retrospective=0Retrospective=0
Planned and performed prospectively in all 31 studies.Planned and performed prospectively in all 31 studies.
Reference standardReference standard Was the rationale for the reference standard stated?Was the rationale for the reference standard stated?Stated=1Stated=1Not stated=0Not stated=0
Not stated for twoNot stated for two12, 1812, 18 studies. studies.
Materials and methodsMaterials and methodsWere technical specifications of material and methods stated Were technical specifications of material and methods stated including how and when measurements were taken?including how and when measurements were taken?
Stated=1Stated=1Not stated=0Not stated=0
Stated in all but oneStated in all but one1919 of the articles. of the articles.
Index testIndex testWere the definitions of and rationales for the units, cutoffs, and/or Were the definitions of and rationales for the units, cutoffs, and/or categories of the results of the index tests stated?categories of the results of the index tests stated?
Stated=1Stated=1Not stated=0Not stated=0
Not stated in twoNot stated in two12, 1912, 19 of the 31 articles. of the 31 articles.
BlindingBlinding Were readers of index test and reference standard blinded?Were readers of index test and reference standard blinded?Blinded=1Blinded=1Not blinded or not Not blinded or not stated=0stated=0
Stated that the readers of index test and reference standard were Stated that the readers of index test and reference standard were blinded in 17blinded in 1710, 11, 19, 29, 30, 35, 36, 37, 38, 3910, 11, 19, 29, 30, 35, 36, 37, 38, 39 articles. articles.
CompletionCompletionWas the number of participants that did not undergo index tests (no. Was the number of participants that did not undergo index tests (no. of tests vs sample size) stated?of tests vs sample size) stated?
Stated=1Stated=1Not stated=0Not stated=0
Stated in all but oneStated in all but one1919 of the studies. of the studies.
Time intervalTime interval Was the time interval from index test to reference standard stated?Was the time interval from index test to reference standard stated?Stated=1Stated=1Not stated=0Not stated=0
The time interval between index test and reference standard (clinical The time interval between index test and reference standard (clinical diagnosis of AKI or severity end point such as dialysis or death) was diagnosis of AKI or severity end point such as dialysis or death) was not stated in fivenot stated in five19, 20, 25, 34, 3619, 20, 25, 34, 36 articles. articles.
Distribution of severity Distribution of severity of diseaseof disease
Was there a representative distribution of severity of disease? (mild, Was there a representative distribution of severity of disease? (mild, moderate, severe AKI; non-oliguric vs oliguric)moderate, severe AKI; non-oliguric vs oliguric)
Yes=1Yes=1No=0No=0
A broad distribution of disease severity was found in all but four A broad distribution of disease severity was found in all but four 12, 25, 12, 25,
27, 3727, 37 of the studies. of the studies.
Scoring system for validity used in this systematic review

References References Biomarker Biomarker Clinical setting Clinical setting Subjects Subjects Sensitivity/specificity Sensitivity/specificity Area under ROC Area under ROC Positive LR Positive LR Quality score Quality score
SerumSerum
Herget-Rosenthal Herget-Rosenthal et al.et al. 99 Cystatin CCystatin C ICUICU 8585 0.82/0.950.82/0.95 NRNR 16.416.4 99
Ahlstrom Ahlstrom et al.et al. 2424 Cystatin CCystatin C ICUICU 202202 NRNR 0.9010.901 N/AN/A 99
Mazul-Sunko Mazul-Sunko et al.et al. 2525 Cystatin CCystatin C ICUICU 2929 0.5/0.50.5/0.5 NRNR 1.01.0 66
Mazul-Sunko Mazul-Sunko et al.et al. 2525 ProANP(1-98)ProANP(1-98) ICUICU 2929 NR/NRNR/NR NRNR N/AN/A 66
Mishra Mishra et al.et al. 1111 NGALNGAL Cardiac surgery in childrenCardiac surgery in children 7171 0.70/0.940.70/0.94 NRNR 11.611.6 1010
Rinder Rinder et al.et al. 2727 Neutrophil CD11bNeutrophil CD11b Cardiac surgeryCardiac surgery 7575 NRNR NRNR 62.662.6†† 88
UrineUrine
Mishra Mishra et al.et al. 1111 NGALNGAL Cardiac surgery in childrenCardiac surgery in children 7171 1.0/0.981.0/0.98 0.9980.998 50.050.0 1010
Wagener Wagener et al.et al. 2828 NGALNGAL Cardiac surgeryCardiac surgery 8181 0.73/0.780.73/0.78 0.80.8 3.33.3 99
Zappitelli Zappitelli et al.et al. 3838 NGALNGAL Critically ill childrenCritically ill children 140140 0.77/0.720.77/0.72 0.780.78 2.752.75 1010
Parikh Parikh et al.et al. 2929 NGALNGAL Post-transplantPost-transplant 6363 0.9/0.830.9/0.83 0.90.9 5.35.3 1010
Parikh Parikh et al.et al. 1010 IL-18IL-18 ICUICU 138138 0.5/0.850.5/0.85 0.730.73 3.33.3 99
Parikh Parikh et al.et al. 2929 IL-18IL-18 Post-transplantPost-transplant 6363 NRNR 0.90.9 N/AN/A 1010
Parikh Parikh et al.et al. 3030 IL-18IL-18 Cardiac surgeryCardiac surgery 7171 0.5/0.940.5/0.94 0.750.75 8.38.3 1010
Han Han et al.et al. 4040 IL-18IL-18 Critically ill childrenCritically ill children 137137 0.25/0.810.25/0.81 0.540.54 1.31.3 1010
Han Han et al.et al. 3737 KIM-1KIM-1 Cardiac surgeryCardiac surgery 4040 0.74/0.900.74/0.90 0.830.83 3.163.16 88
Han Han et al.et al. 3737 NAGNAG Cardiac surgeryCardiac surgery 4040 1.0/0.31.0/0.3 0.690.69 1.431.43 88
Han Han et al.et al. 3737 MMP-9MMP-9 Cardiac surgeryCardiac surgery 4040 NRNR 0.500.50 N/AN/A 88
Eijkenboom Eijkenboom et al.et al. 3131 GSTGST Cardiac surgeryCardiac surgery 8484 NRNR NRNR N/AN/A 99
Westhuyzen Westhuyzen et al.et al. 3232 -GT-GT ICUICU 2626 1.0/0.91.0/0.9 0.950.95 10.010.0 99
Westhuyzen Westhuyzen et al.et al. 3232 -GST-GST ICUICU 2626 1.0/0.91.0/0.9 0.9290.929 10.010.0 99
Westhuyzen Westhuyzen et al.et al. 3232 -GST-GST ICUICU 2626 0.75/0.90.75/0.9 0.8930.893 7.57.5 99
Westhuyzen Westhuyzen et al.et al. 3232 APAP ICUICU 2626 0.5/0.950.5/0.95 0.8630.863 10.010.0 99
Westhuyzen Westhuyzen et al.et al. 3232 NAGNAG ICUICU 2626 1.0/0.811.0/0.81 0.8450.845 5.35.3 99
Westhuyzen Westhuyzen et al.et al. 3232 LDHLDH ICUICU 2626 0.5/0.950.5/0.95 0.6880.688 10.010.0 99
Studies of biomarkers for the early diagnosis of AKI

Promising BiomakersPromising Biomakers
Urinary BiomakersUrinary Biomakers
A.) Inflammatory BiomakersA.) Inflammatory BiomakersNGALNGAL IL - 18 IL - 18
B.) Tubular ProteinsB.) Tubular Proteins KIM - IKIM - I

NGALNGAL (Neutrophil Gelatiaase Associated (Neutrophil Gelatiaase Associated
Lipocalin)Lipocalin)
- - 25 kd protein up regulated in 25 kd protein up regulated in proximal tubule cells in response proximal tubule cells in response to Ischemic or nephrotoxic injury.to Ischemic or nephrotoxic injury.

• Mouse Ischemia
• 30 min ischemia
• S creat ↑ 24 h
• Kidney NGAL ↑ 3 h
• Colocalize with PCNA (proliferating cell nuclear antigen)
Kidney NGAL in Ischemic AKIKidney NGAL in Ischemic AKI
Mishra et al, JASN 14:2534-43, 2003Mishra et al, JASN 15:3073-82, 2004

Urine NGAL in Ischemic AKIUrine NGAL in Ischemic AKI• Mouse Ischemia
• 30 min ischemia
• S creat ↑ 24 h
• Urine NAG ↑ 8 h
• Urine B2M ↑ 8 h
• Urine NGAL ↑ 2 h
Mishra et al, JASN 14:2534-43, 2003Mishra et al, JASN 15:3073-82, 2004

* In development. Currently not for sale in US
® *
Phase 3 Transition: Plasma NGAL Kit

Urine NGAL PlatformUrine NGAL Platform
Abbott DiagnosticsAbbott Diagnostics ARCHITECT: Standardized clinical platformARCHITECT: Standardized clinical platform

IL - 18IL - 18 Pro inflammatory Cytokine induced and Pro inflammatory Cytokine induced and
cleared in proximal tubule after AKI.cleared in proximal tubule after AKI. 20 patient developed AKI post CPB20 patient developed AKI post CPB AKI defined as > 50% AKI defined as > 50% ↑ in serum creatinine↑ in serum creatinine 35 control who did not develop AKI35 control who did not develop AKI
Results :Results :
Using serum creatinine , AKI was detected Using serum creatinine , AKI was detected only 48 – 72 hrs. after CPB.only 48 – 72 hrs. after CPB.
Urine IL – 18 ↑ at 4 – 6 hrs. after CPB and Urine IL – 18 ↑ at 4 – 6 hrs. after CPB and peaked at 12 hrs.peaked at 12 hrs.
Parlikin CR Kid. Int. 2006 , 70 – 199 - 203Parlikin CR Kid. Int. 2006 , 70 – 199 - 203

Tubular ProteinTubular Protein
KIM – I (Kidney Injury Molecule – I)KIM – I (Kidney Injury Molecule – I) Trans membrane protein over Trans membrane protein over
expressed in proximal tubule cells I expressed in proximal tubule cells I ischemic or nephrotoxic AKIischemic or nephrotoxic AKI

ConclusionConclusion Urinary biomakers allow diagnosis of Urinary biomakers allow diagnosis of
AKI earlier than a rise in serum AKI earlier than a rise in serum creatinine.creatinine.
Most of recently discovered biomakers Most of recently discovered biomakers are used to detect proximal tubular are used to detect proximal tubular injury.injury.
e.g – NGAL , 2-4 hrse.g – NGAL , 2-4 hrs
- IL - 18 , 4 – 6 hrs- IL - 18 , 4 – 6 hrs
- KIM – I , 12 – 24 hrs- KIM – I , 12 – 24 hrs

Management of AKIManagement of AKI
Indications for RRT in Patients with AKIIndications for RRT in Patients with AKI
BUN > 27 mmol/LBUN > 27 mmol/L RelativeRelative BUN > 35.7 mmol/LBUN > 35.7 mmol/L AbsoluteAbsolute Hyperkalemia > 6Hyperkalemia > 6 RelativeRelative Hyperkalemia > 6 with ECG changeHyperkalemia > 6 with ECG change AbsoluteAbsolute Acidosis pH > 7.15Acidosis pH > 7.15 RelativeRelative Acidosis pH < 7.15Acidosis pH < 7.15 AbsoluteAbsolute Fluid overload (diuretic sensitive)Fluid overload (diuretic sensitive)RelativeRelative Fluid overload (diuretic resistant)Fluid overload (diuretic resistant) AbsoluteAbsolute RIFLE (R.I.F) RIFLE (R.I.F)
RelativeRelative

Is Early Start of RRT Is Early Start of RRT Better ?Better ?
AA tend toward a better outcome with tend toward a better outcome with early RRT, however , the quality of this early RRT, however , the quality of this trials favoring early timing is poor.trials favoring early timing is poor.

Pharmacological Treatment of Pharmacological Treatment of AKIAKI
Recombinant human IGF–1 (rh IGF–I )Recombinant human IGF–1 (rh IGF–I )
- - Reduced kidney injuryReduced kidney injury
- Decrease apoptosis and - Decrease apoptosis and inflammationinflammation
Atrial naturitic peptideAtrial naturitic peptide
- Dilate afferent arterioles- Dilate afferent arterioles
- Constrict efferent arterioles- Constrict efferent arterioles
Duo to narrow therapeutic windowDuo to narrow therapeutic window
- Failed to reduce AKI in human trials.- Failed to reduce AKI in human trials.

Drugs on the HorizonDrugs on the Horizon Anti-apoptosis/necrosisAnti-apoptosis/necrosis * Caspas inhibitors* Caspas inhibitors
* PARP inhibitors* PARP inhibitors Anti-inflammatoryAnti-inflammatory * Activated protein C* Activated protein C
* L-MSH,anti PPAR-yr* L-MSH,anti PPAR-yr AntisepsisAntisepsis * Activated protein e* Activated protein e
* ethyl pyruvate* ethyl pyruvate Growth factorsGrowth factors * Erythroprotein* Erythroprotein
* HGF* HGF VasodilatersVasodilaters * ANP * ANP
* Co release* Co release New anti-coagulantsNew anti-coagulants * anti factor lla (r-hiridum) * anti factor lla (r-hiridum)
* Anti factor Xa (danaparoid)* Anti factor Xa (danaparoid)
Combination (nafamostat)To prevent Combination (nafamostat)To prevent HITinCVVH patients.HITinCVVH patients.

Conclusion :Conclusion : AKI is common complication in hospitalized AKI is common complication in hospitalized
patients.patients. AKI has strong impact on morbidity and AKI has strong impact on morbidity and
mortality.mortality. Even mild degree of renal dysfunction may Even mild degree of renal dysfunction may
have a negative impact on outcome.have a negative impact on outcome. RIFIE classification is a good outcome RIFIE classification is a good outcome
predictor.predictor. There are promising biomakers for early There are promising biomakers for early
diagnosis and outcome predictor.diagnosis and outcome predictor. Drugs on horizon (no effective Drugs on horizon (no effective
pharmacological therapy).pharmacological therapy).