Embed Size (px)
Citation preview
UPPER GI BLEEDING
MOHD NASHRIQ MOHD YUNOS
VISHNU PRASHAD BHAKTHAVALSALAN
SUPERVISOR: DR KARTHIK
Date : 17 / 2 / 2014
LEARNING OBJECTIVES
To review the major causes of UGIB and the important elements of history taking
To understand the acute management of UGIB
To know the indications for blood transfusion in patients with UGIB
To know the modalities available to stop bleeding and the important post-endoscopic management and monitoring in patients with UGIB
OUTLINE
INTRODUCTION ETIOLOGY & RISK FACTORS CLINICAL PRESENTATION INITIAL ASSESSMENT & RESUSCITATION ENDOSCOPY POST ENDOSCOPY MANAGEMENT & FOLLOW UP INDICATIONS FOR SURGERY IN UGIB
INTRODUCTION
Potentially life-threatening abdominal emergency that remains a common cause of hospitalization.
Bleeding derived from a source proximal to the ligament of Treitz.
The underlying mechanisms of non variceal bleeding involve either arterial haemorrhage or low-pressure venous haemorrhage.
In variceal haemorrhage, the underlying pathophysiology is due to elevated portal pressure transmitted to esophageal and gastric varices and resulting in portal gastropathy.
ETIOLOGY
Non – variceal UGIB : Peptic ulcer disease
Mucosal erosive disease
Mallory – Weis tear
Malignancy
Miscellaneous (Dieulafoy lesion, GAVE, angiodysplasia)
Variceal UGIB : Oesophageal varices
Gastric varices
Peptic Ulcer Disease
The commonest cause of UGIB.
Duodenal ulcers are more common than gastric ulcers.
In approximately 80% of patients, bleeding from a peptic ulcer stops spontaneously.
Etiology/Risk factors:
Helicobacter pylori infection
Non steroidal anti-inflammatory drugs (NSAIDs)
Aspirin
Steroids
Cigarette smoking
Traditional medicine use
Oesophageal Varices
Accounts for 6.4% of UGIB in Malaysia.
Due to increase of hepatic venous pressure gradient >12mmHg
Most commonly seen in chronic hepatitis B with portal hypertension.
Only 30% of patient with varices will have variceal bleeding.
50% will stop spontaneously, but 70% will have re-bleeding especially in the first 5 days.
Risk factors: Hepatitis B &C, Alcohol consumption, Traditional medicine use
CLINICAL PRESENTATION
ACUTE
Hematemesis with / without melena
Melena with / without hematemesis
Hematochezia (massive bleed)
CHRONIC
Iron deficiency anemia with / without evidence of visible blood loss
Blood loss detected by positive Faecal Occult Blood Test
PATIENT ASSESSMENT
Look for signs of shock
Close monitoring of blood pressure, pulse rate, urine output
Look at mental status
Look for features of chronic liver disease
RESUSCITATION
AIRWAY AND BREATHING
A drowsy / comatose patient is at high risk of aspiration pneumonia.
Mental state maybe impaired:
Cerebral hypoperfusion
Hepatic encephalopathy
Alcohol / drug intoxication
Consider intubation if bleeding continuous in drowsy patient.
Patients should receive supplemental oxygen by nasal cannula and should be nil by mouth.
RESUSCITATION CIRCULATION
Insert at least 2 large bore branulla (16 G)
Consider central line in patient with profound shock or elderly with co-morbidities.
Fluid resuscitation with isotonic crystalloids – 20ml/kg bolus, 10ml/kg in patient’s with co-morbids
Blood tests: FBC, GXM, RP, LFT, Coagulation profile
Consider blood transfusion in:
Systolic BP < 110 mmHg
Postural hypotension
Pulse > 110/min
Initial Hb <8g/dL
Cardiovascular disease with Hb <10g/dL
Correct coagulopathy
Give FFP if INR > 1.5
Consider giving platelets if platelet < 50,000/mm3
ASSESSMENT OF ON-GOING BLEEDING
Continuous hematemesis
Persistent hypovolemia despite aggressive fluid resuscitation.
Passage of fresh melena or bright red visible clot
HISTORY AND PHYSICAL EXAMINATION
Specific causes of upper GI bleeding may be suggested by the patient's symptoms :
Peptic ulcer: Epigastric or right upper quadrant pain
Esophageal ulcer: Odynophagia, gastroesophageal reflux, dysphagia
Mallory-Weiss tear: Emesis, retching, or coughing prior to hematemesis
Variceal hemorrhage or portal hypertensive gastropathy: Jaundice, weakness, fatigue, anorexia, abdominal distention
Malignancy: Dysphagia, early satiety, involuntary weight loss, cachexia
HISTORY AND PHYSICAL EXAMINATION
Past medical history:
History of liver disease (Hepatitis B / C, cirrhosis, ascites) or alcohol abuse
Previous history of UGIB, previous endoscopy findings
Co – morbids:
Renal disease / heart disease
Predispose patients to volume overload in the setting of fluid resuscitation or blood transfusions
Coagulopathies ( hemophilia, thrombocytopenia)- Result in bleeding that is more difficult to control
Medications history:
Aspirin and other non steroidal anti-inflammatory drugs (NSAIDs)
Anti-platelet agents and anticoagulants
Bismuth and iron, which can turn the stool black
Physical examination
Stigmata of any chronic liver disease
Features of portal hypertension
Any lymphadenopathy
Abdominal mass
Digital rectal examination: melena
ENDOSCOPY Endoscopy is the modality of choice following resuscitation
- Diagnostic
- Therapeutic
Emergency Endoscopy unstable patients with severe acute UGIB following resuscitation
Early endoscopy (within 24H of presentation) is recommended for all other patients with acute UGIB
Before Procedure
Consent
PPI therapy
Routine use of prokinetics prior to endoscopy not recommended
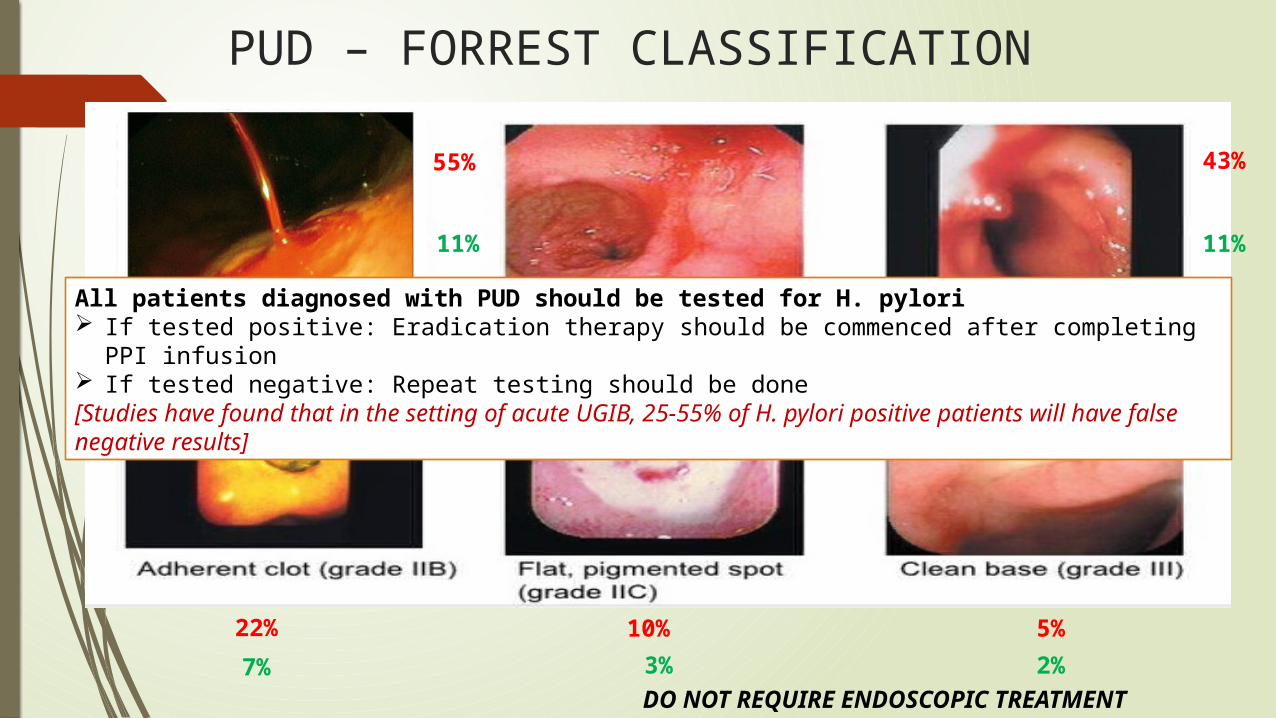
PUD – FORREST CLASSIFICATION
55%
11%
43%
22% 10% 5%
11%
7% 3% 2%DO NOT REQUIRE ENDOSCOPIC TREATMENT
All patients diagnosed with PUD should be tested for H. pylori If tested positive: Eradication therapy should be commenced after completing PPI infusion If tested negative: Repeat testing should be done[Studies have found that in the setting of acute UGIB, 25-55% of H. pylori positive patients will have false negative results]
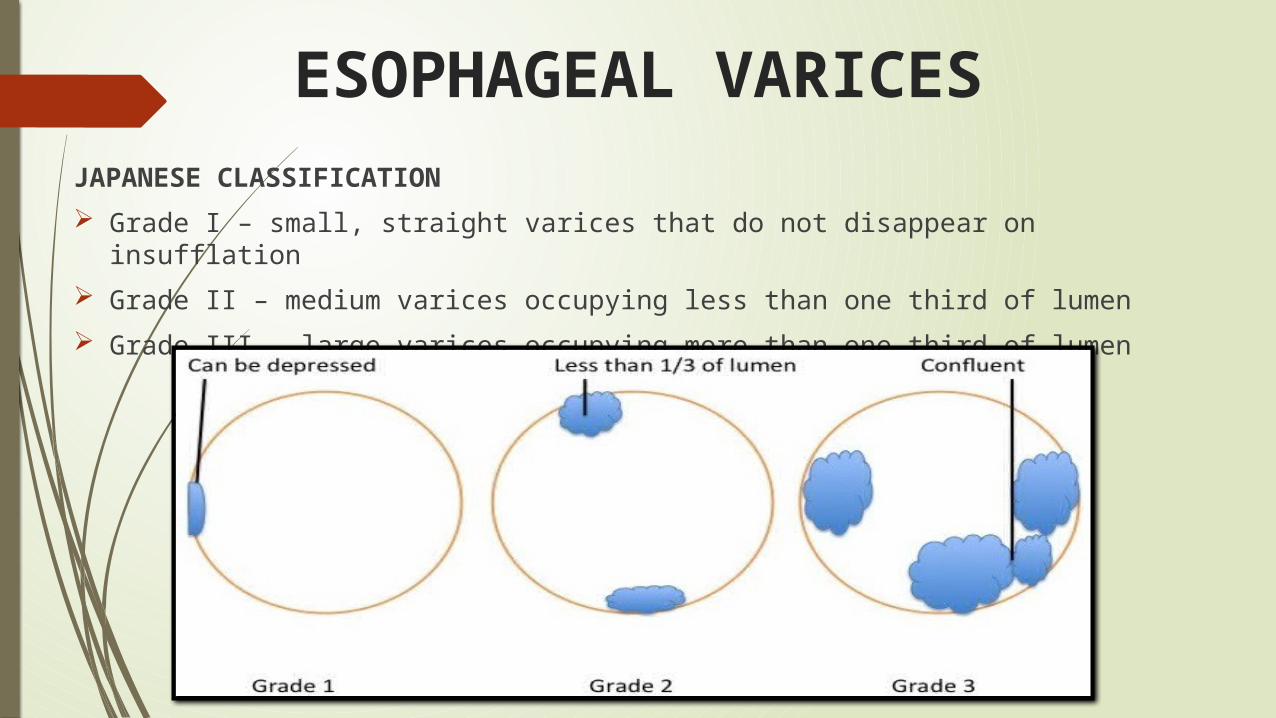
ESOPHAGEAL VARICESJAPANESE CLASSIFICATION
Grade I – small, straight varices that do not disappear on insufflation
Grade II – medium varices occupying less than one third of lumen
Grade III – large varices occupying more than one third of lumen
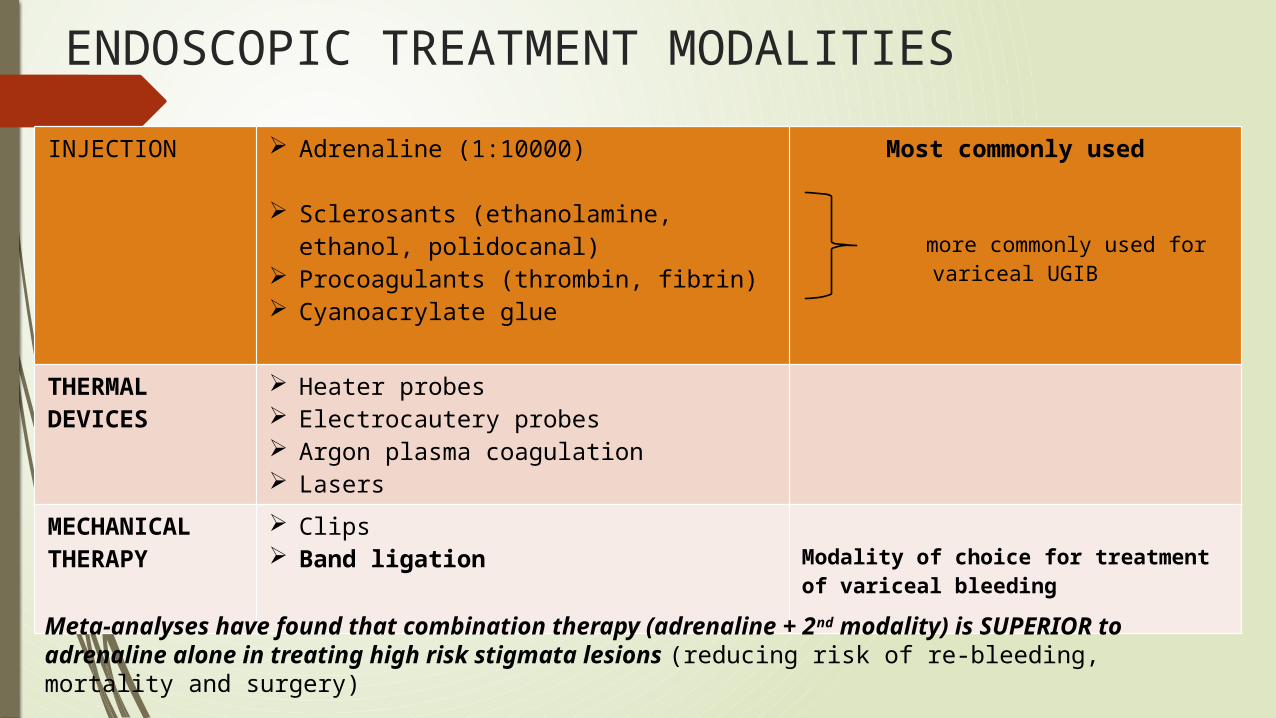
ENDOSCOPIC TREATMENT MODALITIES
INJECTION Adrenaline (1:10000)
Sclerosants (ethanolamine, ethanol, polidocanal)
Procoagulants (thrombin, fibrin) Cyanoacrylate glue
Most commonly used
more commonly used for
variceal UGIB
THERMAL DEVICES
Heater probes Electrocautery probes Argon plasma coagulation Lasers
MECHANICAL THERAPY
Clips Band ligation Modality of choice for treatment of
variceal bleeding
Meta-analyses have found that combination therapy (adrenaline + 2nd modality) is SUPERIOR to adrenaline alone in treating high risk stigmata lesions (reducing risk of re-bleeding, mortality and surgery)
VARICEAL BLEEDING – OTHER MODALITIES
a) Balloon tamponade – only if endoscopic facilities unavailable (prior to transfer to tertiary centre) or as a temporary bridging measure until further definitive therapy can be instituted
b) Transjugular Intrahepatic Portosystemic Shunt (TIPS)**
c) Surgical therapy (includes oesophageal transection, portosystemic shunts, liver transplants)**
** Rescue/salvage therapy for uncontrolled variceal bleeding after combined pharmacological & endoscopic therapy
POST ENDOSCOPY
PPI INFUSION (for high risk stigmata PUD)
IV bolus 80mg, followed by high dose infusion (8mg/H) for 72H
Low risk stigmata = can be started on IV PPI after endoscopy
Once infusion completed switch to IV or oral PPI
Subsequent duration & dose of oral PPI depends on the underlying etiology
PHARMACOLOGICAL THERAPY (for variceal bleeding)
Octreotide (somatostatin analogue)
- causes splanchnic vasoconstriction, decreasing portal blood flow + pressure
- 50mcg bolus followed by 50mcg/H infusion for up to 5 days
Terlipressin (vasopressin analogue)
- 2mg bolus followed by 1mg every 4 hours
MAIN ISSUE: COST!!!!
POST ENDOSCOPY
CLOSE MONITORING IN WARD
To look out for re-bleeding (risk of re-bleeding is highest in the first few days)
V/S monitoring – persistent tachycardia, hypotension
Pallor, lethargy (despite blood transfusion)
Per Rectal Examination – fresh melena
FBC – drop in Hb
REPEAT ENDOSCOPIC THERAPY
Only if re-bleeding occurs
Repeat 2nd look endoscopy in the acute setting no longer recommended
POST ENDOSCOPY (PUD)
PATIENTS WHO TEST POSITIVE FOR H. PYLORI
Eradication therapy (10 – 14 days)
First line (triple therapy) : PPI + Amoxicillin + Clarithromycin [Failure rate about 20%]
2nd line (quadruple therapy): PPI + Bismuth + Tetracycline + Metronidazole
NSAIDs & ASPIRIN
Studies have found that combination of PPI + COX-2 inhibitor had lower risk of re-bleeding compared to NSAIDs + PPI and COX-2 inhibitors alone
ASA therapy should be restarted as soon as risk of thromboembolic complications is thought to outweigh risk of bleeding
Restarting/withdrawing/changing anti-platelet should involve consultation with cardiologist or physician
POST ENDOSCOPY (Variceal Bleed)ANTIBIOTIC PROPHYLAXIS
Bacterial infection is seen in 20% of cirrhotic patients presenting with UGIB within 48 H
Guidelines recommend starting antibiotic prophylaxis in all cirrhotic patients who present with UGIB irrespective of type of bleeding or presence of ascites
Type of antibiotic: IV 3rd generation cephalosporin/oral quinolones for minimum 7 days
SECONDARY PROPHYLAXIS
70% of patients will experience re-bleeding (1/3 of these are fatal)
Non-selective beta blockers (titrated to max tolerable dose) ± nitrates
Surveillance OGDS & banding (every 2-3 weeks until varices eradicated)
TIPS/ Surgical therapy – for patients not compliant/refractory to above
GASTRO REFERRAL
For follow-up and management of underlying chronic liver disease
INDICATIONS FOR SURGERY IN UGIB
Failure of endoscopic haemostasis with persistent bleeding
Severe life threatening haemorrhage not responsive to resuscitation
Co-existing reason for surgery (obstruction, perforation, malignancy)
Alternative for patients who are not good candidates for surgery & in centres where such facilities are available INTERVENTIONAL RADIOLOGY (ANGIOGRAPHIC EMBOLIZATION)
TAKE HOME MESSAGES
1. ABC (Airway, Breathing, Circulation) is the first step in assessing a patient presenting with UGIB
2. All patients with UGIB must have at least 2 large bore branula (16G) inserted and resuscitated using crystalloids as first line
3. Blood transfusion should be considered in patients with SBP <110 mmHg, HR>110 bpm, initial Hb < 8g/dL (or < 10g/dL in patients with U/L cardiac disease)
4. Early endoscopy is recommended for all patients presenting with UGIB following resuscitation
5. All patients with high risk stigmata PUD must complete PPI infusion for 72 H post endoscopy to reduce the risk of re-bleeding
6. All patients must be monitored closely in the ward post endoscopy (V/S, UO, PR, Hb) to detect re-bleeding early
7. First line therapy for H.pylori eradication is PPI + Amoxicillin + Clarithromycin for 10-14 days
8. All patients with variceal bleeding must undergo surveillance OGDS & banding following bleeding episode to prevent re-bleeding
REFERENCES
1. [Guideline] Barkun AN, Bardou M, Kuipers EJ, et al. International consensus recommendations on the management of patients with nonvariceal upper gastrointestinal bleeding. Ann Intern Med. Jan 19 2010;152(2):101-13.
2. Hwang JH, Fischer DA, Ben-Menachem T, Chandrasekhara V, Chathadi K et al. ASGE guideline: The role of endoscopy in acute non-variceal upper-GI hemorrhage. Gastrointest Endosc. 2012;75(6):1132-1138
3. NICE Clinical Guideline. Acute upper gastrointestinal bleeding: management.
4. [Best Evidence] Leontiadis GI, Sharma VK, Howden CW. Proton pump inhibitor therapy for peptic ulcer bleeding: Cochrane collaboration meta-analysis of randomized controlled trials. Mayo Clin Proc. Mar 2007;82(3):286-96.
5. British Society of Gastroenterology. UK guidelines on the management of variceal haemorrhage in cirrhotic patients. June 2000.
6. Garcia-Tsao G, Sanyal AJ, Grace ND, Carey W et al. AASLD Practice Guidelines. Prevention and management of gastroesophageal varices and variceal haemorrhage in cirrhosis. Hepatology. 2007; 46(3): 922-938
7. Malaysian Clinical Practice Guidelines. Management of Acute Variceal Bleeding. 2007 May.
8. Kim J. Management & prevention of upper GI bleeding. Gastroenterology & Nutrition. PSAP-VII: 7-26
9. http://www.uptodate.com/contents/approach-to-acute-upper-gastrointestinal-bleeding-in-adults

THANK YOU….