Embed Size (px)
Citation preview

Upper GIT bleeding
Prepared by:
Maryam abdulwahid
Tanya muhammad
Hewar jarjis
Sanaa fuad
Hedi Hamid
Hawrin Muhammad
Rawand Muhammad

• Its considers as medical emergencies.
• Any bleeding above the ligament of treitz is upper
GI bleeding and bellow the ligament of treitz is
lower GI bleeding.
This ligament is anatomic cut-off for upper GI
bleeding that connect the fourth part of duodenum
to the diaphragm near the splenic flexer of colon.

Clinical presentation
Hematamesis (coffee-ground emesis, Gross blood
and clots )
Melena ( black tarry stool and have distintive
odour)
Hematochezia(passage of bright red blood per
rectum)

Patient may also present complication of anemia
including chest pain, syncope, fatigue, shortness
of breath.
dyspepsia, heart burn, epigastric pain, dysphagia,
difuse abd.pain, wt loss……


Risk factors
1. alcohol abuse
2. Non-steroidal anti inflammatory
drugs.
3. Chronic renal failure
4.Age
5.Low socio economic class

Approach
1/Estimate severity of bleeding
2/ localize site of bleeding
3/ Resuscitation
4/ diagnosis
5/ Treatment
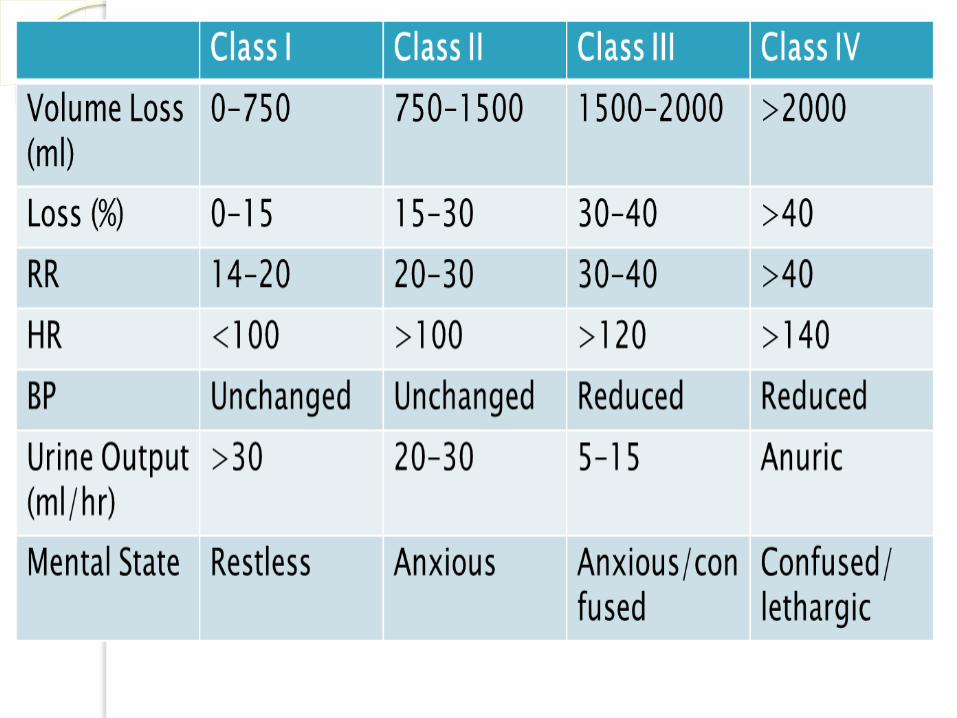
Assessment severity
Through history and examination initially
History includes abdominal or epigastric pain , weakness, dizziness, hematamesis, melena and syncope
History of recent drug ingestion (aspirin ,NSAID)
history of PU
EXAMINATION :
the extent of blood loss and signs of shock !!
By Pulse and blood pressure
pallor and signs of anamia
postural hypotension

Other signs of shock :
Cool extremities
Chest pain
Confusion
Delirium
Also evidence of dehydration
And urine output should be monitored

Resuscitation
Cannula
NG tube
Foley catheter
Blood sample
N/S
Transfer blood if:
Correct bleeding disorders
Iced normal saline.

Peptic ulcer
Peptic ulcer includes both duodenal ulcer and gastric ulcer
Incidence of gastric ulcer is equal in both male and female
but the population tend to be older
Incidence of duodenal ulcer is higher in males than in
females.
How to suspect PU ?
The signs and symptoms are suggestive of PU but the
definitive diagnosis of PU is by endoscopy

Common sites of peptic ulcer
First part of duodenum
Lesser curvature of the stomach

Etiology of peptic ulcer
high gastric acid level
helicobacter pylori
gastrinoma (zollinger-ellison syndrome)
NSAID
social stress, smoking and genetic factors
malignancy

Sites of the bleeding ulcer
- DU they tend to erode posteriorly causing
bleeding of gastroduodenal artery
- Left gastric artery is involved in 85% bleeding
sometimes is from splenic artery
precaution should be taken when a gastric
ulcer is seen
Diagnosis
-OGD is both diagnostic and therapeutic for PU,
early endoscopy allows estimation of the rate of
recurrent bleeding and enables various therapeutic
options.
-Barium contrast can also be used for diagnosis

Treatment
Anti-acids; h2 receptor antagonists (cimetidine and
ranitidine…) and PPI (omeprazole, pantoprazol,… )
Endoscopic electrocoagulation
Angiographic embolization
Surgery
-patient with a visible vessel on the ulcer base
-a spurting vessel
-an ulcer with clot in the base

Esophageal varices
esophageal varices are enlarged veins in the walls of the
lower part of the esophagus.
10% of UGIT bleeding
30% mortality rate
symptoms may include:
melena
hematoschezia
Light-headedness
Paleness
Symptoms of chronic liver disease
Vomiting
hematemesis

Treatment
Vasoactive drugs…terlipressin, or somatostatin
Endoscopy/Band ligation is the first choice of treatment.
Emergency sclerotherapy is still widely used as a first-line
therapy for variceal bleeding in patients with cirrhosis, especially
when band ligation is not available.
Balloon tube tamponade (Sengstaken-Blakemore
tube)
Transjugular intrahepatic portosystemic shunt
Surgery/Oesophageal transection and gastric
devascularisation are rare procedures but may
have a role for patients with portal and splenic vein
thrombosis

Gastritis Gastritis is an inflammation, irritation, or erosion
of the lining of the stomach.
1/3 of UGIT bleeding
Acute/ NSAID, steroid, alcohol & potassium.
Chronic/ H.pylori bacteria.

Rx
Lifestyle changes :
avoid or limit alcohol consumption
avoid spicy, fried, and acidic foods
eat frequent, small meals
reduce stress.
Antacids: H2rb, PPI
Eradication of H.pylori
Vassopressin infusion.
Endoscopic electrocoagulation
Surgery
MALLORY WEISS SYNDROME
A condition characterized by upper gastrointestinal bleeding secondary to longitudinal mucosal lacerations at gastroesophagealjunction.
accounts of about 15% UGIT bleeding .
More common in male than female.
Risk factors: repeated vomiting, alcohol intake, coughing, blunt abdominal trauma, hiatal hernia.
Presentation:
hematemesis
melena
hematochezia
abdominal pain

Diagnosis:Esophagogastric duodenoscopy ( by active bleeding, clot , fibrin crust over mucosa within or near gastroesophageal junction).
Treatment:_may stop spontaneously.
Endoscopic therapy: coagulation and epinephrine injection Angiotherapy: Elective vasopressin infusion or embolization of the left gastric artery.
Surgery

Thank you