Embed Size (px)
Citation preview

1
Undescended Testis
By L. Dehdehi
بسم الله الرحمن الرحیم

2
Undescended testis is the commonest genital malformation in boys.
Although the mechanism that regulates prenatal testicular descent is still partly obscure, there is persuasive evidence that endocrine, genetic, and environmental factors are involved.
Approximately 10% of the infertile men have a history of cryptorchidism and orchidopexy.
Azoospermia is evident in 13% of unilateral cryptorchidism and increase to 89% in untreated bilateral cryptorchid patients.
The risk of infertility in adulthood is more significant in patients with bilateral undescended testes.
Introduction
The main risk factors for the cryptorchid testis are infertility and testicular cancer (TC)

3
In both sexes, the descent of the gonad depends on the ligamentous gubernaculum.
Between the 7th and 12th weeks (the intra-abdominal phase), the extrainguinal portions of the gubernacula shorten and in males, pull the testes down to the vicinity of the deep inguinal ring. The testes remain in the vicinity of the deep ring from the 3rd to the 7th month but then enter the inguinal canal in response to renewed shortening and migration of the gubernacula (the inguinal-scrotal phase)
The testes remain within the subserous fascia of the vaginal process through which they descend toward the scrotum.
Testicular descent and maldescent
The process of testicular descent has two distinct phases: transabdominal and inguinal

4
By the 9th month, just before normal term delivery, the testes have completely entered the scrotal sac and the gubernaculum is reduced to a small ligamentous

5
Many undescended testicles are accompanied by patency of the vaginal process This like the simultaneous presence of inguinal hernia, is treated surgically during the orchidofuniculolysis procedure.

6
Prevalence Up to one third of premature boys are affected by
maldescensus testis, while about 2% to 5% of full-term boys have at least one undescended testicle.
Short-term postnatal endogenous testosterone secretion reduces this incidence to 1% to 2% after three months.
The pathology is bilateral in about 20% of the cases.
A birth weight below 2.5 kg and premature delivery are risk factors for maldescent.
About 80% of undescended testes are palpable and 20% are non-palpable
Palpable undescended testes are located along the inguino-scrotal region

7
Undescended testis can be categorized on the basis of physical examinationsUndescended testis : The testicle is located intra-abdominally or in the inguinal canal. It is located in the normal descent pathway and shows normal insertion of the gubernaculum.
Cryptorchidism: The testicle is not palpable and is located intra-abdominally (retentio testis abdominalis) or is not present (anorchia).
Ektopia testis: The testicle is located beneath the skin superfascially, perineally, on the thigh or shaft of the penis. The testicle shows abnormal insertion of the gubernaculum
Inguinal testicle: The testicle is palpable in the groin (retentio testis inguinalis)
Gliding testicle: The testicle is located at the scrotal entrance or above the scrotum. It can be drawn down into the scrotum, but immediately slides back into its initial position
Retractile (hypermobile testes): The physiological retractile (hypermobile) testicle is usually present in the scrotum or can be effortlessly pushed down into the scrotum, it retracts on induction of the cremasteric reflex but returns spontaneously into the scrotum. Recognizing the retractile (hypermobile) testicle is particularly important because it does not require treatment.

8
It is important to differentiate the true cryptorchidism from the retractile testis, which is a normal finding and usually it does not require surgical treatment
The anatomical classification of undescended testis :
Maldescended testes: (lying somewhere along the normal line of descent)
Ectopic testes: (lying outside that line
Retractile testes are when, on occasion, the muscle attached to the testis (the cremasteric muscle) pulls the testis up into the groin so that it cannot be felt or seen. If the testis can be moved back down to the scrotum, then no further treatment is needed. Retractile testes can stay higher in the scrotum over the years, but this usually corrects itself by puberty

9
During transabdominal descent, development of the gubernaculum and genitoinguinal ligament plays an important role.
The anti Müllerian hormone regulates the transabdominal descent of the testes. Induction of the gubernaculum depends on a functional Insl3 gene in mice
This gene is expressed in Leydig cells and its targeted deletion causes bilateral cryptorchidism with free-moving testes and genital ducts
Androgens play an important role in both phases of testicular descent, while other gene families, e.g. the homeobox (HOX) and GREAT/RXFP2 genes (G-protein-coupled receptor affecting testis descent), are important in the development of genital organs and may be associated with testicular maldescent.

10Hormonal control of testicular descent
Maldescent can be caused by two hormonal factors: hypogonadism and androgen insensitivity.
Androgens and pituitary hormones clearly play essential roles in mediating the second stage of descent.
The increasing incidence of reproductive abnormalities in male humans can be explained by increased oestrogen exposure during gestation .
Some pesticides and synthetic chemicals act as hormonal modulators, often possessing oestrogenic activity (xeno-oestrogens). The oestrogenic and anti-androgenic properties of these chemicals may cause hypospadias, cryptorchidism, reduced sperm density, and an increased incidence of testicular tumours in animal models, via receptor-mediated mechanisms or direct toxic effects associated with Leydig cell dysfunction.

11
Pathophysiological effects in maldescended testes
Degeneration of germ cells Relationship with fertility Germ cell tumours
The degeneration of germ cells in maldescended testes is apparent after the first year of life.
Degenerative changes vary, depending on the position of the testis.During the second year, the number of germ cells declines.
In 10-45% of affected patients, the complete loss of germ cells can be detected

12
It starts during the first years after birthIn normal testes, germ cell development is an active process starting in the first months of life when the neonatal gonocytes transform into adult dark (AD) spermatogonia. These cells are now thought to be the stem cells useful to support spermatogenesis. Several researches suggest that AD spermatogonia form between 3 and 9 months of age. Not all the neonatal gonocytes transform into AD spermatogonia; indeed, the residual gonocytes undergo involution by apoptosis. In the undescended testes, these transformations are inhibited leading to a deficient pool of stem cells for post pubertal spermatogenesis.
Germ cell development
Gonocyte
adult dark (AD) spermatogonia
Adult pale(AP) spermatogonia
B spermatgnia
Primary spermatocyt
es
Data suggest that AD spermatogonia developmental cycle needs normal testicular hormones and the optimal scrotal temperature of 33°C

13
The failure of transformation of gonocytes into AD spermatogonia leads to a deficient pool of stem cells for post pubertal spermatogenesis and infertility.
in undescended testes, germ cells loss starts at 6 months of age
It is very interesting to note that the intra-tubular carcinoma in situ (CIS) in the second and third decade has enzyme markers similar to neonatal gonocytes as placental alkaline phosphatase expression, suggesting that these cells, that fail to develop in AD spermatogonia at 3–9 months of age, are the origin of cancer in cryptorchid men.
Testiclar cancer
(TC)

14
The etiology accepted for germ cell carcinoma remains unknown, although disturbances in the microenvironment provided by the Sertoli and Leydig cells may play an important role. In fact, spermatogenesis is strictly controlled and depends on a succession of signals supplied from the local environment and Leydig cells, next to their steroidogenic function, during development express the insulin-like-3 gene (INSL3), which is responsible for gubernaculum maturation and testicular descent.
A specific association of mutations in INSL3 with cryptorchidism has been described but its possible role in TC development and infertility needs to be clarified.
Leydig cell gubernaculum
maturation testicular descent
INSL3

15
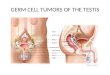
It is known that undescended testes, if untreated, lead to an increased risk of TC, usually seminomas, arising from mutant germ cells. TC is a solid neoplasm that has an incidence of 1% of all cancers in men and is the most common between 20 and 30 years of life.
Boys with an undescended testis have a 20-fold higher risk to develop a TC and about 10% of the cases of TC develop in men with a history of cryptorchidism.

16
Treatment of undescended testes
Hormonal treatment (Hormone therapy) Surgical treatment
The goals of treatment of cryptorchidism are mainly two: preserve fertility and reduce the risk of neoplastic disease. Last but not the least, treatment allows the testicular self-examination for an early diagnosis and detection of TC.
In the new guidelines, two goals of hormone therapy are pursued:
induction of descent of the retained testicle stimulation of germ cell maturation and proliferation to
contribute to improving fertility.
Hormonal treatment with human chorionic gonadotropin (hCG) or gonadotropin-releasing hormone (GnRH) may be initially administered for cryptorchidism because it should promote the testicular descent.
although 15-20% of retained testes descend during hormonal treatment, one-fifth of these re-ascend later

17
The theoretical basis for its use is to stimulate the Leydig cells to produce testosterone, inducing inguinal–scrotal testicular descent.
Potential harmful effects of hormonal treatment on the developing testes, including apoptosis, inflammation, and reduced number of germ cells are still under study.
In addition, there are reports which suggest that the hormonal stimulation in infancy may be damaging to the testes. These experimental data emphasize the possible negative outcome of hormone therapy on germ cell line and its main action on Leydig cells. The increased synthesis of vascular endothelial growth factor (VEGF), determined by hCG therapy also highlights the increased cell permeability causing interstitial edema.
Side effects of hCG therapy may include enlargement of the penis (3%), growth of genital hair, testicular enlargement, and aggressive behaviour of the child during the treatment (1%).

18
In a comparative randomized double-blind study, clinical success was observed in 6% of the boys treated with hCG and in 19% after GnRH treatment.
Increases in luteinizing hormone (LH), follicle stimulating hormone (FSH) and the non-measurability of Mullerian inhibiting substance (MIS) are
suggestive of anorchia. Elevated gonadotropins and a negative intramuscular human chorionic gonadotropin (hCG) stimulation test without evidence of testosterone production reinforce this assumption. Final proof of anorchia, however, is provided by surgical exploration.
For bilateral nonpalpable testicles, a pediatric endocrinological assessment is indicated, among other things in order to rule out other syndromes.

19
Stimulated testosterone values are compared before and 32 hours after an intramuscular dose of 5000 IU hCG. If functional testicular tissue is present, the testosterone values increase to twice the baseline value after hCG administration. Increased baseline FSH and LH values associated with an absent testosterone increase after stimulation demonstrates the absence of functional testicular tissue. With a normal phenotype and normal 46-XY karyotype, the diagnosis anorchia can be regarded as certain.
The hCG stimulation test is used to demonstrate the presence of functional testicular tissue. It is therefore only useful in bilateral cryptorchidism.

20
The following factors increase child’s chance of having undescended testes:
Prematurity Low birth weight Twin gestation Down syndrome (fetus) or other chromosomal abnormality Gestational diabetes mellitus Prenatal alcohol exposure Hormonal abnormalities (fetus) Toxic exposures in the mother Mother younger than 20 A family history of undescended testes
Risk Factors

21
Surgical treatment
The purpose of the operation is to search for the retracted testicle and, after adequate orchidolysis, to achieve tension-free transfer to and fixation in the scrotum. For intra-abdominal testicle, this is possible using either an open surgical or laparoscopic technique.
An incision is made into the abdomen, the site of the undescended testicle, and another is made in the scrotum (A). The testis is detached from surrounding tissues (B) and pulled out of the abdominal incision attached to the spermatic cord (C). The testis is then pulled down into the scrotum (D) and stitched into place (E).

22
The reasons for performing an operation include:
Fertility: men with undescended testicles have a higher rate of infertility
Hernia:An undescended testicle is associated with a connection between the abdomen and scrotum called a “hernia”. During repair of the testicle, the hernia sac is closed
Tumor: Undescended testicles have a higher risk of developing a testicular tumor, periodically examine the testicle. This is very important for early detection of tumors.
Torsion: Undescended testicles have a higher risk of spontaneously twisting and stopping the blood flow to the testicleOne complication of orchidopexy is testicular atrophy. Division of
the testicular vessels and/or postoperative swellings and infections can result in testicular ischemia and cause (partial) atrophy of the testicle

23

24
High scrotal unilateral cryptorchid gliding testis. Shown is a biopsy specimen from a 17-year-old Patient. The biopsy specimen shows a maturation arrest of spermatogenesis ( asterisks ). The other tubules are lined by Sertoli cells only

25
High scrotal unilateral cryptorchid testis. The seminiferous tubules are lined by Sertoli cells and degenerated spermatogonia with some maturation to the primary spermatocyte stage ( asterisk ).

26
high scrotal unilateral cryptorchid gliding testis from a 20-year-old man. This sample allows comparison of immature ( stars ) with mature (crosslet ) Sertoli cells. The immature cells within nodules are smaller; they contain minor nuclei without a clear nucleolar complex and have scanty cytoplasm. Hyaline deposits ( H ) in the middle of the nodules may originate from an increased production of basement membrane material. In contrast, mature Sertoli cells havea well-de fi ned nucleolar complex and plentiful cytoplasm.

27
high scrotal unilateral cryptorchid gliding testis in a 19-year-old man. The cytoplasm of the Sertoli cells is granulated. The nuclei of these cells may be wrinkled ( arrowheads )

28
Biopsy specimen from a 21-year-old man with a high scrotal unilateral cryptorchid gliding testis. The tubule is lined by mature Sertoli cells only. In the Sertoli cell cytoplasm, many slender spindle-shaped Charcot-Böttcher crystals are present ( arrowheads ). The tunica propria is thickened( arrow )

Thanks for your attention