Embed Size (px)
Citation preview
Two Year Experience of VNS
Efficacy in Refractory Epilepsy in Iraq
(Neurosciences Hospital)
Mohammad A.S. Kamil, Zaki Nooh Hasan, Sajid Ibrahim Kadhim, Ahmed A Salam Al Atraqchi ,Aqeel
Kareem Hatim ,Moneer K. Faraj
“Patients who fail two AED medications used appropriately are likely to have a medically refractory seizure disorder and should be investigated for alternative forms of treatment.
Potential treatment options include experimental drug trials, surgical treatment, electrical stimulation and combination of the above.
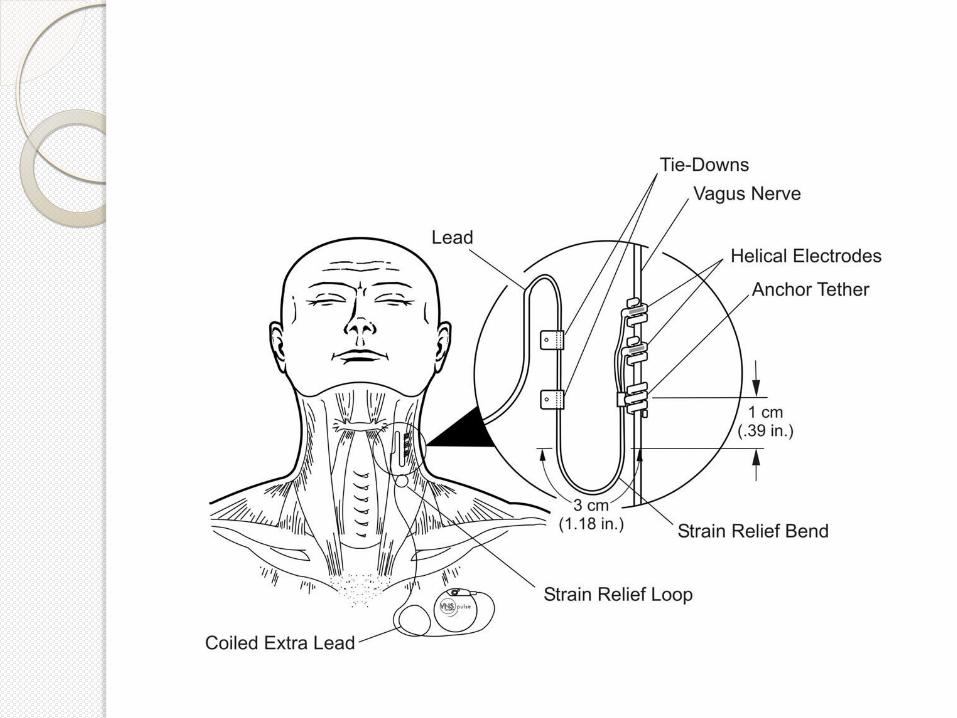
Vagus nerve stimulation (VNS) is approved by Food and Drug Administration
(FDA) for management of intractable epilepsy in 1997.
It is possible that VNS may interrupt the spread of epileptiform activity if delivered at a theoretically critical time; It is possible that VNS causes small changes in brain dynamics resulting in larger effects that inhibit the brain from becoming dynamically entrained, thus interrupting any progression towards a clinical seizure.

Patients and method:
A retrospective study evaluating ,
Thirty-four patients diagnosed as refractory epilepsy according to ILAE criteria who had been operated for VNS implantation by a team of neurologists and neurosurgeons in neurosciences hospital in Baghdad, they were interviewed at epilepsy center, by taking thorough history and revaluation of the epilepsy state, frequency and severity of the attacks, number of the anti-epileptic drugs (AEDs), duration of the epilepsy before and after the implantation of the device was assessed.
Twenty-one male thirteen females were enrolled in the study .
The first implant in Neurosciences hospital in Iraq was at 24-2-2008 and last one in 5-1-2009 which included in this study,all subjects consented to participate in the research prior to their inclusion in the study, and the local ethics committee approved the study protocol.
Two weeks after implantation
first programming was done and then periodic programming every two weeks depending on clinical assessment.

RESULTS
1) Improvement in the severity of the attacks.
2) Frequency of the seizure attacks before and after implantation of the device.
3) No. of the AED before and after implantation of the device.
4) Adverse effects of the device on the patients.
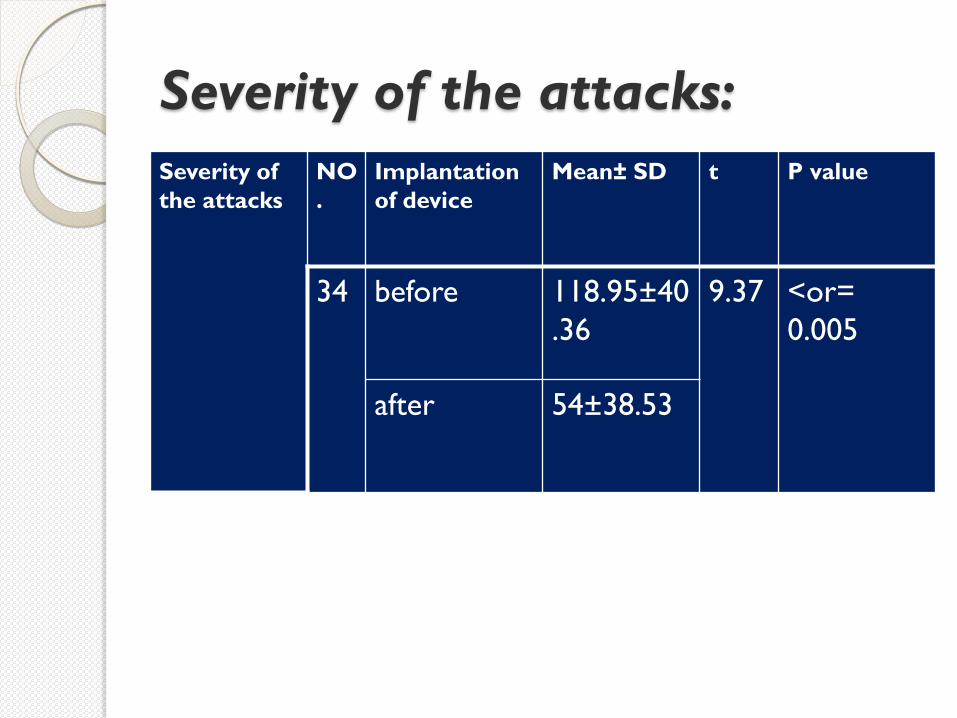
Severity of the attacks:
Severity of the attacks
NO.
Implantation of device
Mean± SD t P value
34 before 118.95±40.36
9.37 <or= 0.005
after 54±38.53
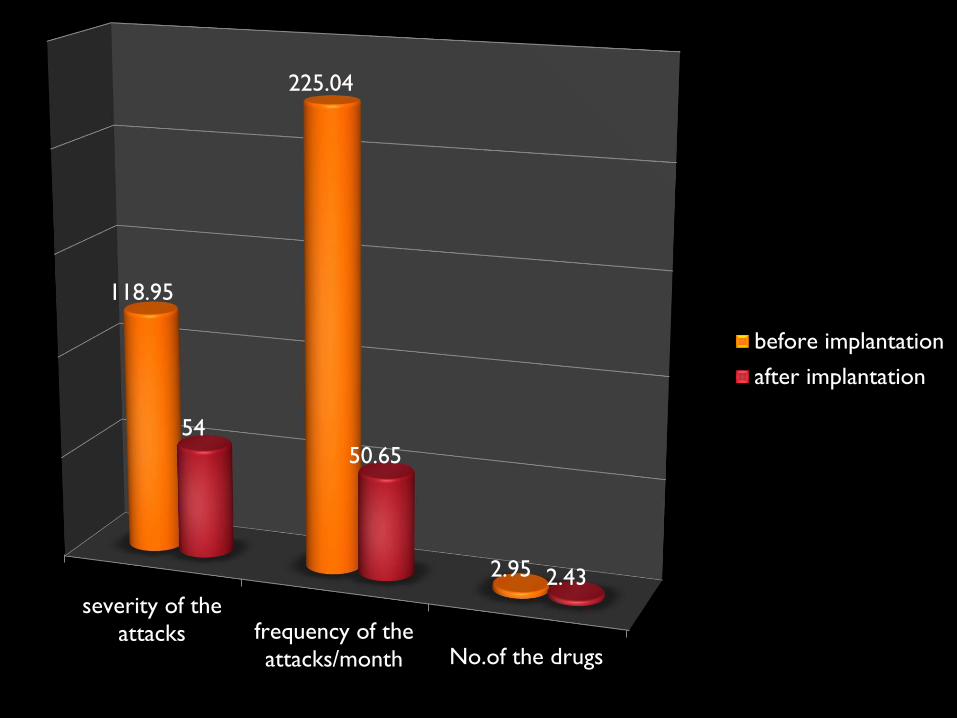
severity of theattacks frequency of the
attacks/month No.of the drugs
118.95
225.04
2.95
54 50.65
2.43
before implantation
after implantation

Improvement in the severity of the attacks
Severity
of the
attacks
100%
improvemen
t
50%-99%
improvemen
t
<50% Improveme
nt
No improvemen
t
9(34) 26.5%
9(34) 26.5%
16(34) 47%
0(34) 0%
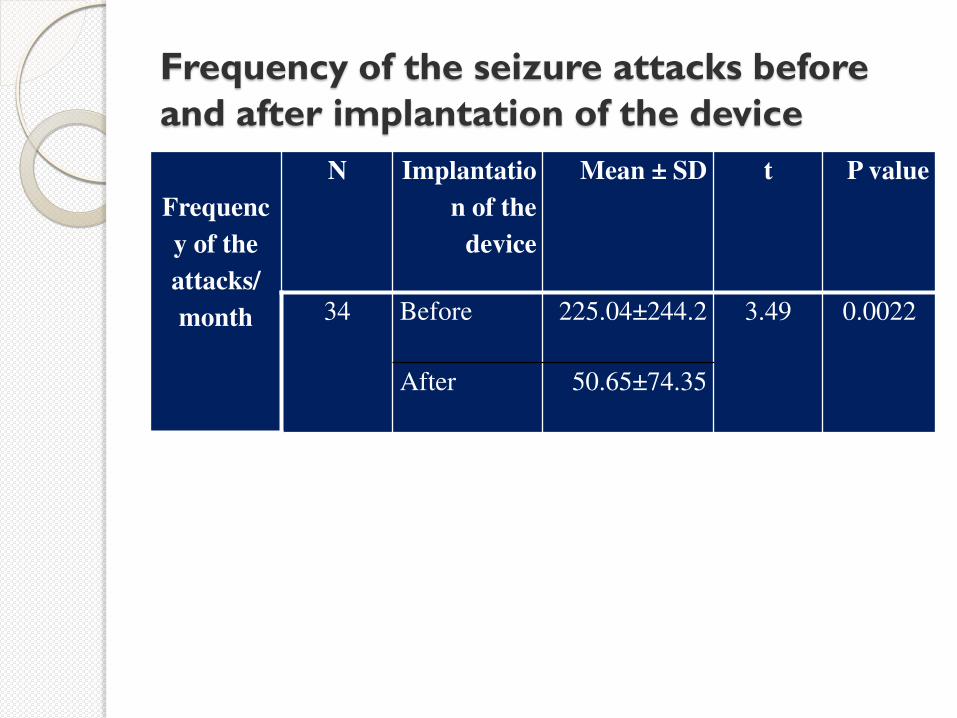
Frequency of the seizure attacks before and after implantation of the device
Frequenc
y of the
attacks/ month
N Implantatio
n of the
device
Mean ± SD t P value
34 Before 225.04±244.2 3.49 0.0022
After 50.65±74.35
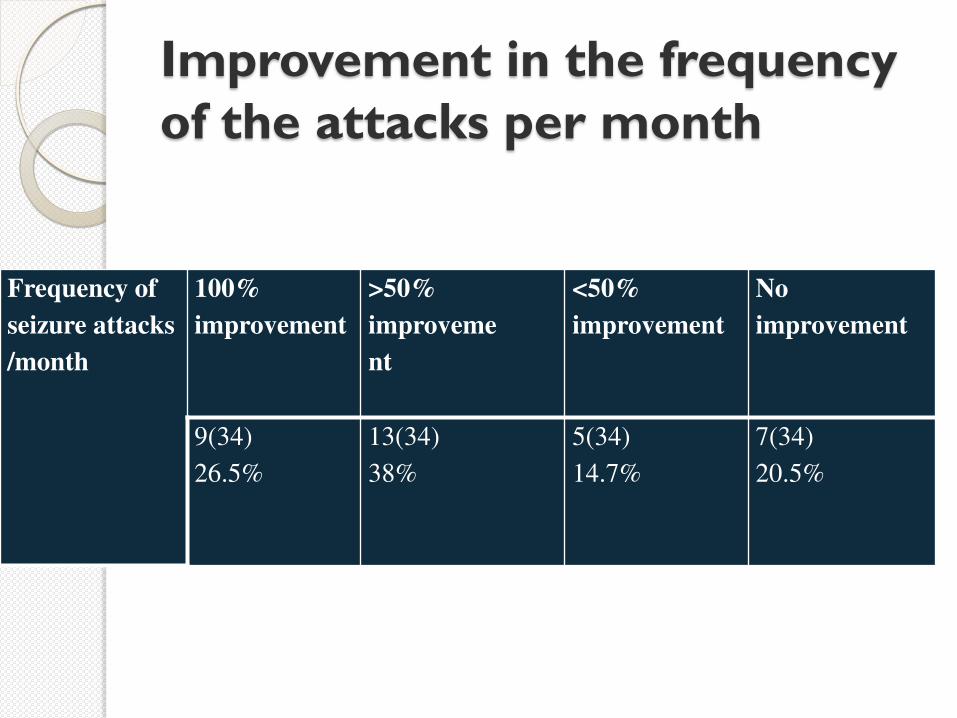
Improvement in the frequency of the attacks per month
Frequency of
seizure attacks
/month
100%
improvement >50%
improveme
nt
<50%
improvement No
improvement
9(34) 26.5%
13(34) 38%
5(34) 14.7%
7(34) 20.5%
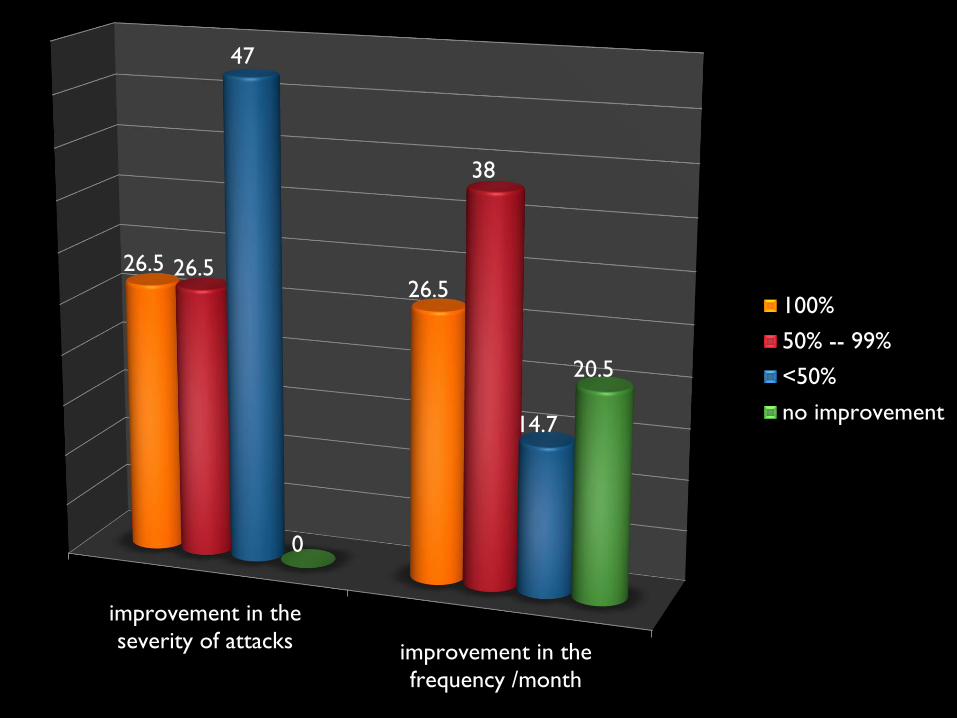
improvement in theseverity of attacks improvement in the
frequency /month
26.5 26.5
26.5
38
47
14.7
0
20.5
100%
50% -- 99%
<50%
no improvement
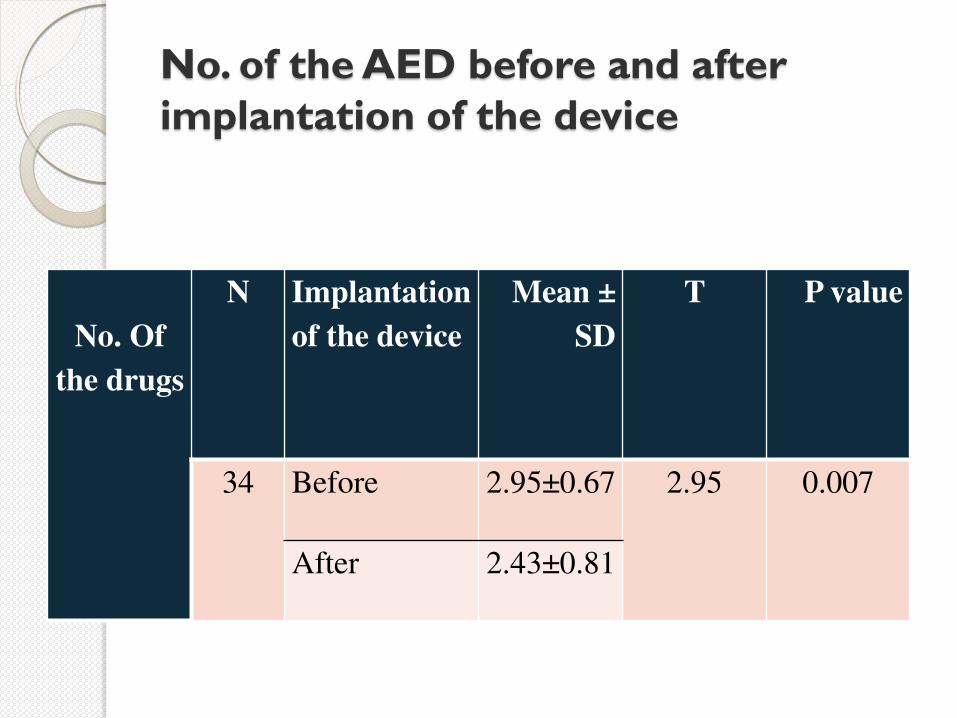
No. of the AED before and after implantation of the device
No. Of
the drugs
N Implantation
of the device Mean ±
SD T P value
34 Before 2.95±0.67 2.95 0.007
After 2.43±0.81
Adverse effects of the device on the patients Statistical analysis of the side
effects observed by the patients after implantation of the device shows hoarseness of the voice the most common side
effect 55.8%. Followed by dysphagia 41%, cough, dyspnea,
palpitation 14.7%, and headache5.8%. The device were removed in 4 patients because
of the Infection at the site of the device in one patient; Aspiration pneumonia in one, Suicidal attempt in one and Loss of contact in one.
Conclusions
Vagal nerve stimulation is a good adjunctive tool of therapy added on drug therapy for patient with refractory epilepsy.
It is effective safe and well tolerated in our patient.

THANK YOU

![Clinical efficacy of tolvaptan for treatment of refractory ascites in ...€¦ · Ascites is one of the most common complications of liv-er cirrhosis[1]. Refractory ascites occur](https://img.pdfslide.us/doc/110x75/5f0c3caf7e708231d43468bd/clinical-efficacy-of-tolvaptan-for-treatment-of-refractory-ascites-in-ascites.jpg)



















![Vns fashion logistics [compatibility mode]](https://img.pdfslide.us/doc/110x75/555c6d98d8b42ab6748b556c/vns-fashion-logistics-compatibility-mode.jpg)







