Embed Size (px)
DESCRIPTION
Is the impedance index (ht2/R) significant in predicting total body water?13
Citation preview

ImJC/in iVi�tr 1992:56:835-9. Printed in USA. © 1992 American Society forClinical Nutrition 835
Is the impedance index (ht2/R) significant inpredicting total body water?13
Robert F Kushner, Dale A Schoeller, Carla R Fjeld, and Lynn Danford
ABSTRACT We investigated the general utility of bioelec-
tncal impedance analysis (BIA) and the implications of BIA
theory in populations ofvarious ages from infancy to adulthood
by developing a single impedance equation. Four subject data#{149}
sets representing 62 adults, 37 prepubertal children, 44 preschool
children, and 32 premature low-birth-weight neonates were
combined. Subjects were randomly divided into a development
group (n = 1 16) and a cross-validation group (n = 59). The
single best predictor of total body water (TBW) was height2,’
resistance (ht2lR), which explained 99% ofthe variation in TBW
(SEE = 1 .67 kg). The addition of weight reduced the SEE to
I .41 kg. A significant bias was only seen in the preschool children.
These results were confirmed in the cross-validation group and
the best prediction formula was TBW = 0.59 ht2/R + 0.065 wt
+ 0.04. We conclude that the impedance index (ht2lR) is a sig-
nificant predictor ofTBW and that there is some improvement
in prediction ofTBW by inclusion ofa weight term. Am J
C/in Nutr 1992:56:835-9.
KEY WORDS Bioelectrical impedance analysis, body corn-
position, anthropometry
Introduction
Bioelectrical impedance analysis (BIA) is based on the prim-
ciple that the impedance (Z) ofa cylindrical conductor is related
to its length (L), cross-sectional area, and applied signal fre-
quency. On the basis of this relationship, it was proposed that
the volume of a conductor is proportional to L2/Z. More than
30 y ago, Thomasset (1) and Hoffer et al (2) tested this hypothesis
in a biological system and demonstrated that the volume of total
body water (TBW) was indeed proportional to L2/Z. Thus, BIA
could be used to estimate TBW by applying a predictive equation
based on the measured bioelectncal impedance of the subject.
Using height as a measure of conductor length, Hoffer et al
showed that ht2lZ was a better predictor of 3H2O-denved TBW
than was the weight term alone in 20 normal volunteers (r = 0.92
vs r = 0.74). Subsequent regression analyses by several investi-
gators have also demonstrated that the impedance index (ht2l
R; where R is resistance) yielded larger correlation coefficients
than weight or height when used as predictors of TBW, densi-
tometrically determined fat-free mass (dFFM), or total body po-
tassium (3, 4).
Although the impedance index has been shown to be a strong
predictor of TBW, it has also been observed that the accuracy
of predicting TBW or dFFM by BIA is significantly improved
by the inclusion ofadditional variables such as weight, age, and
sex (4, 5). The selection of variables and their coefficients has
differed from one study to another because ofdissimilar subject
populations ranging in age from infants to elderly adults. Fur-
thermore, some investigators have observed that these anthro-
pometnc variables can be even stronger predictors ofTBW than
BIA. For example, Deurenberg et al (6) recently suggested that
the prediction of dFFM by the BIA method offered little or no
advantage over simpler anthropometric techniques that use
weight, height, sex, and age. Thus, it remains controversial
whether the high correlations reported for BIA prediction equa-
tions are primarily based on these additional independent subject
characteristics or whether they are due to BIA (7).
Despite this controversy, we have noted a striking similarity
ofthe various regression equations relating impedance to TBW
in a wide range of age groups studied by us and others (8- 1 1).
This suggested to us that there may be a single relationship re-
lating impedance to TBW. Therefore, the aims of this study
were to evaluate the underlying principle of BIA and develop a
single TBW-predictive equation, and to evaluate the importance
ofthe impedance term (ht2lR) as a predictor ofTBW compared
with other independent subject characteristics.
Subjects and methods
Four data sets from adults (group 1, n = 62), prepubertal
children (group 2, n = 37), preschool children (group 3, n = 44),
and premature low-birth.weight neonates (group 4, n = 32) were
used in this study. The subjects were previously enrolled in stud-
ies on body-composition measurement andlor energy metabo-
lism (8, 9, 12; L Danford, D Schoeller, R Kushner, unpublished
observations for group 2, 1990). All participating adult subjects
or guardians for the children gave informed written consent for
the study, which was approved by the Institutional Review Board
ofthe University ofChicago (groups 1 and 2) and ofthe Instituto
de Investigaci#{243}n Nutnci#{243}nal in Lima, Peru (group 3). Subjects
from group 4, taken from the study by Mayfield et al (12), were
studied during the first 24 h ofpostnatal life and at 4-7 d of age.
The protocol for group 4 was approved by the Institutional Re-
view Board of the University of Texas Southwestern Medical
I From the Clinical Nutrition Research Unit, University of Chicago,and the Washington University School of Medicine, St Louis.
2 Supported by NIH grant DK 30031.
3 Address reprint requests to RF Kushner, 584 1 South Maryland Av-
enue, MC4080, Chicago, IL 60637.
Received December 31, 1991.Accepted for publication May 7, 1992.
by on Decem
ber 24, 2007 w
ww
.ajcn.orgD
ownloaded from

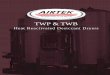
125
100
75
50
25
00 10 20 30 40 50 60 70 80
TBW, kg
FIG 1. Relationship between impedance index (ht2/R) and total bodywater (TBW) measured by stable-isotope dilution in the development
group (r = 0.996, SEE = 1.47 kg).
836 KUSHNER ET AL
Center. Physical characteristics and TBW measurements for all
175 subjects are shown in Table 1 . The combined data set was
rerandomized into a development group (n = 1 16) and a cross-
validation group (n - 59) by using a random number table.
Although each of these data sets has been previously reported,
the combination of the four data sets produced a unique pop-
ulation representing a broad range of ages (6 h-66 y), heights
(35.2- 183 cm), weights (0.82-200 kg), and TBW (0.68-74. 1 kg).
All subjects had height, weight, BIA, and TBW determined
on the same day. Prepubertal children and adults were asked to
fast from the previous evening. Height was measured without
shoes to the nearest 1 .0 mm. Supine crown-heel length was used
instead of standing height in groups 3 and 4. Weight was mea-
sured to the nearest 0. 1 kg with a standard balance-beam scale
in two groups and an electronic balance in the preschool children
and infants. BIA was performed with a body-composition an-
alyzer (model BIA-lOl RJL Systems, Detroit) with a right-sided
tetrapolar placement of electrodes as previously described (8).
Whole-body R was recorded as the mean of three to five con-
secutive measurements made in immediate succession. The
mean CV for within-day repeated measurements was previously
demonstrated to be 1.3% (8).
TBW was obtained by deuterium dilution (D2O-TBW) in
groups 1 and 2 and by 80 dilution (‘8O-TBW) in groups 3 and
4 as previously described (8, 9). For the D2O-TBW technique,
baseline saliva samples were obtained followed by oral admin-
istration of0.06 (group 1) and 0.08 g (group 2) D2O (99.8 atom
% excess) per kg estimated TBW (TBW was assumed to ap-proximate 60% of body weight). The D2O dilution space was
measured by repeat saliva sampling at 3 h. The ‘8O-TBW in
group 3 was determined by obtaining a baseline morning urine
sample followed by an oral dose of 0.08 g 180 (1 1.34 atom %
excess) per kg body weight given as H218O by syringe. Urine
samples were collected for at least three postdose voids, the last
� 5 h postdose. Group 4 subjects were given 10% enriched H218O
(0.6 mLlkg body wt) by gavage. After a 3-h equilibrium period,
1 .5 mL venous blood was obtained for 180 dilution. D20-TBW
and “O-TBW were both analyzed by isotope-ratio mass spec-
trometry as previously described (8, 9). TBW was assumed to
be 96% ofD2O- and 99% ofH2t8O-dilution spaces, respectively.
We previously demonstrated that these techniques for TBW do
not differ by > 1-2% (13).
Statistical analysis
Linear- and stepwise multiple-regression analyses were applied
to the data to determine the most significant variable or variables
TABLE ISubject characteristics
Sex
Group Age
y
(Male, Female) Height
cm
Weight
kg
TBW*
kg
Equation developmentNeonates
(n = 21) 0.02 NAt 41 (37-44)� 1.6 (0.8-2.1) 1.3 (0.07-1.6)
Preschool children
(n = 29) 1.1 (0.3-2.5) 18, 1 1 71 (58-84) 7.6 (3.9-14.4) 4.9 (2.8-9.1)Prepubertal children
(n = 24) 7.6 (4.8-9.8) 14, 10 129 (104-145) 31 (16-69) 16 (10-26)
Adults
(n = 42) 41 (23-66) 15, 27 170 (155-193) 85 (48-200) 38 (25-74)
Equation validationNeonates
(n = 1 1) 0.02 (0.6-2.5) NAt 41 (35-46) 1.6 (0.8-2.2) 1.3 (0.7-1.8)Preschool children
(n = 15) 1.3 (0.6-2.5) 12, 3 73 (60-86) 8.7 (5.2-1 1.6) 5.4 (4.1-7.4)Prepubertal children
(n = 13) 7.9 (6.4-9.9) 9, 4 129 (108-143) 31 (17-57) 16 (10-23)
Adults(n = 20) 39 (22-67) 1 1, 9 169 (150-180) 77 (58-144) 38 (27-5 1)
* Total body water.
t Not available.1: 1 (range).
by on Decem
ber 24, 2007 w
ww
.ajcn.orgD
ownloaded from

e� #{149} #{149} �#{149} . #{149}.#{149} #{149}. * #{149}#{149}� .#{149} #{149}#{149}
#{149}. .
10
FIG 2. Residual plot for prediction of total body water (TBW) byequation using impedance index (ht2/R) and weight. TBW is plotted on
a semilog scale for visual purposes.
TABLE 2
IMPEDANCE INDEX AND BODY WATER 837
5
4
3
.� 2
� I
� 0
(00� -2
-3
-4
-5
TBW, kg
to predict TBW and to yield the lowest SEE. Statistical calcu-
lations were performed by using Minitab (Minitab Inc. State
College, PA). The regression equations were then used to predict
TBW in the cross-validation group. The bias, or mean residual
(TBW predicted - TBW measured), was tested for significance
by using a Student’s t test with P < 0.01 to adjust for five com-
parisons. Precision, or SD ofthe residuals, ofthe various possible
predictive equations was tested for significance relative to the
impedance index plus weight equation by using the F test. A Pvalue < 0.0 1 was required for significance to adjust for five com-
parisons.
Results
Stepwise linear regression was performed by using height,
weight, age, ht2lR, height2, and llR for the 1 16 subjects in the
development group. Impedance index (ht2lR) was the strongest
predictor identified, explaining 99% of the variance in TBW (r
= 0.996, SEE - 1 .47 kg) (Fig 1). The only other predictor iden-
tified as significant was weight, which when combined with the
impedance index accounted for 99.5% ofthe variance (r = 0.997,
SEE= 1.24kg).
Cross validation of the predictive equations based on imped-
ance index plus weight (Fig 2), however, detected a significant
bias among the neonates (residual = 0.24 ± 0. 1 3 kg, P < 0.00 1)
and preschool children (residual = -0.37 ± 0.34 kg, P < 0.01).
Because of the bias detected in cross validation, the stepwise
regression was repeated without both the low-birth-weight-infant
and preschool-children groups. In this treatment impedance in-
dcx was identified as the most significant predictor and weight
as the only additional significant predictor. Again, residuals were
calculated for the cross-validation group. No significant bias was
detected for the neonatal group (residual = 0.05 ± 0. 1 3 kg, NS),
but bias was detected for the preschool group (residual = -0.54
± 0.34, P < 0.01), indicating that the preschool group was an
outlier. The preschool group was deleted from all further regres-
sion analysis of the development group.
Entering predictor variables from the neonates, prepubertal
children, and adults in the development group, stepwise regres-
I 00 sion identified impedance index as the strongest predictor (r= 0.995, SEE = 1 .67 kg) and weight as the only additional sig-
nificant predictor (r = 0.997, SEE = 1.41 kg). The developmental
equations based on impedance index alone and impedance index
and weight were tested in the cross-validation group (Table 2).
As expected, significant bias was detected in the preschool chil-
dren. Among the other three groups bias was detected for equa-
tions based on impedance index alone and then only in the
neonates. The prediction equation based on impedance index
and weight had better precision than that based on impedance
index alone; however, the improvement was only statistically
significant in the adult group. The recommended equation for
predicting TBW (in kg) is 0.59 ht2/R + 0.065 wt + 0.04: however,
we are uncertain of its applicability among preschool children
(ages 1-60 mo).
Importantly, the residuals calculated by using the equation
based on impedance index and weight developed in the above
three groups were a relatively constant percentage of mean TBW
in each of the subject groups. The relative bias and CV for the
cross validation were neonates 0.8 ± 10.3%, prepubertal children
0.3 ± 3.2%, and adults -1.6 ± 4.5%.
To determine the relative importance ofthe impedance index
in predicting TBW, single- and multiple-regression analyses were
performed for height, weight, height2, and llR among the de-
velopment group and the results were compared with those ob-
tamed by using the impedance index (Table 3). Again, the pre-
school children were deleted from this comparison. Correlation
coefficients for all other variables were smaller than those of
impedance index plus weight. Similarly, SEEs were always larger
than those for impedance index plus weight.
To further investigate the predictive value of the impedance
index relative to height2 and llR, we calculated the residuals
among the cross-validation subjects (Fig 3A-D). Residuals for
the prediction ofTBW from either height2 or l,’R as single pre-
dictors were quite large and not consistent across the range of
subjects. Residuals using height2 and 1lR as independent van-
ables resulted in relatively constant residuals across the range of
Cross validation of predictive equations developed by using data from adults, children, and neonates*
Equation Adults Prepubertal children Preschool children Neonates
kg
TBW = 0.700 ht2/R - 0.32 -0.25 ± 2.53 0.21 ± 0.72 -0.74 ± 0.37t -0.25 ± 0.1StTBW = 0.593 ht2/R + 0.O6Swt + 0.04 -0.61 ± l.71f 0.05 ± 0.51 -0.58 ± 0.34t 0.01 ± 0.13
* Residual .� ± SD.
t Residual significantly different from 0, P < 0.01.� SD less than that predicted when only the impedance index was used, P < 0.05.
by on Decem
ber 24, 2007 w
ww
.ajcn.orgD
ownloaded from

KUSHNER ET AL
ht� A20 20
hR B
.� 10. : -� 10, ,v�,
-0
<�
(I)Lii�
0
-10
.#{149}#{149}.#{149}#{149}#{149}
.
.%.
%.
.
-Cl)
<�
(1)w�
0
-10
v�V �
� � TV
� V
y
,�,� y
V V �V
V V�V
V
#{149}#{149}�. #{149}%#{149}S#{149} . :#{149}
. .#{149}
-201
#{149}
-20
1
V
�
1010 100
20
TBW, kg
20
TBW, kg
ht2/R oht2 & hR C
.�, 10 .� 10
c/i’�
00
a#{163} #{163}�
A
#{163}*� #{163}ah
AAA
#{163}�
a aaaA
c#{244}’<
Q
U
#{149}#{149}
V� �
#{149}
�.#{149}#{149}y��#{149} �
#{149} #{149} #{149}
#{149}W.#{149}
,
aia‘�
#{232}A�
a t 1*a a
I a
C,)w�
a
-10
-201
a)w�
�
100
-10
-201
I
10 10010
838
TABLE 3Relative importance of the impedance index in predicting total bodywater in adults, children, and neonates
Predictor r SEE
kg
Height 0.897 7.59Weight 0.959 4.87Height + weight 0.98 1 3.36Height2 0.934 6.13Height2 + weight 0.986 2.841/resistance 0.907 7.24Height2 + 1/resistance 0.982 3.25Height2/resistance 0.995 1.67Height2/resistance + weight 0.997 1.41
subjects, but were still relatively large. Only when the ht2-R ratio
was used did the residuals become small enough (3-10%) for
this technique to be practically useful within the neonatal and
prepubertal-children groups.
Discussion
BIA has many advantages over other body-composition
methods in that it is safe, inexpensive, portable, rapid, and easy
to perform and it requires minimal operator training. Despite
these potential benefits, tojustify the use ofBIA it must be shown
to significantly improve the accuracy and precision of predictive
equations compared with those based on anthropometric mea-
surements alone.
In a recent review of validation studies involving adults and
children, which compared BIA with TBW or dFFM (14), the
impedance index was reported to be the best single predictor of
these compartments by multiple-regression analysis in 16 of 21
studies, accounting for 69% to 96% of the total predictive van-
ability (3- 10, 1 5-25). In five of the studies (7, 22-25), height
(or height2) and weight were more significant predictors than
were ht2/R or R alone.
Three of the latter studies incorporated a select group of sub-
jects for their analysis and we postulated that this might reduce
the importance of ht2lR. For example, Diaz et al (7) studied a
small group of young adults consisting of postpartum women,
farm laborers, and institute staffwhose body weights and heights
were smaller than those in other validation studies involving
adults. Diaz et al found that after height and weight were entered
into the multivariate equation, ht2lR contributed � 5% to the
prediction ofdFFM. In a study by Helenius et al (22) ofa group
of overweight middle-aged men and women, it was observed
that ht2/R did not contribute to the estimation of densitometry-
determined percent body fat when added to other selected an-
TBW, kg TBW, kg
FIG 3. Residual plots for total body water (TBW) predicted from various combinations of resistance (R) and heightindicate that the impedance index (ht2/R) is a better predictor than are other combinations of R and height in the
cross-validation group. A, TBW = -3.4 + 0.00140 ht2; B, TBW = -35.8 ± 37400/R; C, TBW = -23.7 + 19300/R+ 0.000871 ht2; and D, TBW = -0.3 + 0.70 ht2/R. Regression coefficients and SEEs are given in Table 3. TBW isplotted on a semilog scale for visual purposes.
by on Decem
ber 24, 2007 w
ww
.ajcn.orgD
ownloaded from

IMPEDANCE INDEX AND BODY WATER 839
thropometric variables. Gray et al (23) found that weight and
height2 were selected into a stepwise regression to explain a
greater portion ofthe variability by the statistical computer pro-
gram before ht2lR was used in a group of 87 adults, 75% of
whom were obese. Only Jackson et al (24) and Van Loan and
Mayclin (25) observed that standard anthropometnc measure-
ments were more powerful predictors of dFFM than was bio-
electrical impedance in a broad sample of adult subjects.
The present study was therefore performed to determine
whether a single BIA equation could be generated from a large,
heterogenous population, and to reinvestigate the significance
of the impedance term (ht2lR) as a predictor of TBW. The useof a large, heterogenous data set with a wide range of heights,
weights, and TBWs gave us the opportunity to statistically assess
the relative importance of measuring whole-body R compared
with simple anthropometric variables in a mixed population.
Furthermore, using TBW as the reference method instead of
dFFM, we eliminated the inherent errors in assuming a constant
density and hydration factor for fat-free mass across age groups.
We also included a cross-validation group to assess the predictive
value of the derived equations.
First, our results show that ht2/R is the single best predictor
of TBW (it results in the lowest SEE) and explains 99% of the
variance in TBW. In comparison, the combination of the an-
thropometric variables weight and height alone yield an SEE
that is twofold higher than ht2/R. The SEE is reduced slightly
by the substitution of height2 for height, as it is used in the
impedance term. Second, the impedance index is a superior pre-
dictor of TBW compared with either 1lR, height2, or both hR
and height2, demonstrating the importance of the impedance
term as suggested by the model originally described by Hoffer
et al (2).
The finding that weight improves the precision ofthe equation,
ie, reduces the SEE, most likely stems from the fact that the
human body does not behave as the ideal conductor proposed
during the development ofthe theory of BIA. BIA assumes that
the body is a geometrical isotropic conductor with uniform length
and cross-sectional area. However, the body more closely re-
sembles a series offive cylinders (two arms, two legs, and trunk),
each with a different geometry and resistivity. The addition of
weight, sex, and age probably adjusts for differences between
individuals and the relative underrepresentation ofthe trunk by
whole-body impedance.
The -7% underestimate ofTBW by BIA in the Peruvian pre-
school children (group 3) cannot now be fully explained. How-
ever, we do not believe that it results from the inclusion of mal-
nourished subjects in this group because the bias was observed
in both the well-nourished and malnourished subgroupings.
In summary, we conclude that the measurement of bioelec-
trical impedance significantly improves the prediction of TBW
as validated in a large heterogenous group ofadult and pediatric
subjects. The method should be useful in estimating the body
composition ofpopulation groups such as those in epidemiologic
studies. B
References
1 . Thomasett A. Bio-electrical properties of tissue impedance mea-surements. Lyon Med l962;207:l07-18.
2. Hoffer ED, Meador CK, Simpson DC. Correlation of whole-bodyimpedance with total body water volume. I Appl Physiol 1969;27:
53 1-4.
3. Lukaski HC, Johnson PE, Bolonchuk WW, Lykken GI. Assessmentof fat-free mass using bioelectrical impedance measurements of the
human body. Am J Clin Nutr l985;41:8l0-7.4. Segal KR, Gutin B, Presta E, Wang I, Van Itallie TB. Estimation
of human body composition by electrical impedance methods: acomparative study. J AppI Physiol l985;58: 1�6�-71.
5. Lukaski HC, Bolonchuk WW, Hall CB, Siders WA. Validation oftetrapolar bioelectrical impedance method to assess human body
composition. J Appl Physiol l986;60: 1327-32.6. Deurenberg P, van der Kooy K, Leenen R, Weststrate JA, Seidell
JC. Sex and age specific prediction formulas for estimating body
composition from bioelectrical impedance: a cross-validation study.IntiObes 199h;l5:l7-25.
7. Diaz EO, Villar J, Immink M, Gonzales T. Bioimpedance or an-thropometry? Eur J Gin Nutr l989;43: 129-37.
8. Kushner RF, Schoeller DA. Estimation oftotal body water by bio-electrical impedance analysis. Am J Chin Nutr 1986;44:4h7-24.
9. Fjeld CR, Freundt-Thurne J, Schoeller DA. Total body water mea-
sured by 80 dilution and bioelectrical impedance in well and mal-nourished children. Pediatr Res 1990;27:98-l02.
10. Davies PSW, Preece MA, Hicks Ci, Halhiday D. The prediction oftotal body water using bioelectncal impedance in children and ad-olescents. Ann Hum Biol l988;l5:237-40.
1 1. Lukaski HC, Bolonchuk WW. Estimation of body fluid volumes
using tetrapolar bioelectrical impedance measurements Aviat SpaceEnviron Med 1988;59:l 163-9.
12. MayfIeld SR. Vauy R, Waidelich D. Body composition of low-birth-weight infants determined by using bioelectrical resistance and re-
actance. Am J Chin Nutr 199l;54:296-303.13. Schoeller DA, Kushner RF, Taylor P, Dietz WH, Bandini L. Mea-
surement oftotal body water� isotope dilution techniques. In: RocheAF, ed. body composition assessments in youth and adults. Colum-
bus, OH: Ross Laboratories, 1985:24-9.14. Kushner RE. Bioelectrical impedance analysis: a review of principles
and applications. J Am Coll Nutr 1992;l 1:199-209.
15. Segal KR, Van Loan M, Fitzgerald P1, Hodgdon JA, Van Italic TB.
Lean body mass estimation by bioclectrical impedance analysis: afour-site cross-validation study. Am J Gin Nutr 1988;47:7-l4.
16. Heitmann BL. Prediction ofbody water and fat in adult Danes from
measurement ofelectrical impedance. A validation study. Int J Obes
l990;l4:789-802.
17. Deurenberg P, van der Kooy K, Evers P, Hulshofl. Assessment ofbody composition by bioelectrical impedance in a population aged> 60 y. Am J Clin Nutr l990;5 1:3-6.
18. Cordain L, Whicker RE, Johnson JE. Body composition determi-nation in children using bioelectiical impedance. Gmwth Dev Aging
1988;52:37-40.
19. Deurenberg P, van der Kooy K, Paling A, Withagen P. Assessment
of body composition in 8-I 1 year old children by bioelectricalimpedance. Eur J Gin Nutr l989;43:623-9.
20. Houtkooper LB, Lohman TO, Going SC, Hall MC. Validity of bio-
electric impedance for body composition assessment in children. J
Appl Physiol l989;66:8h4-2l.21. Deurenberg P, Kusters CSL, Smit HE. Assessment of body corn-
position by bioelectrical impedance in children and young adults is
strongly age-dependent. Eur J Gin Nutr l990;44:26l-8.22. Helenius MYT, Albanes D, Micozzi MS, Taylor PR, Heinonen OP.
Studies ofbioelectnc resistance in overweight, middle-aged subjects.Hum Biol l987;59:27l-9.
23. Gray DA, Bray GA, Gemayal N, Kaplan K. Effect of obesity on
bioelectrical impedance. Am J Gin Nutr 1989;50:255-60.
24. Jackson AS, Pollock ML, Graves JE, Mahar MT. Reliability andvalidity ofbioelectncal impedance in determining body composition.
J Appl Physiol l988;64:529-34.25. Van Loan M, Mayclin P. Bioelectrical impedance analysis: is it a
reliable estimator of lean body mass and total body water? Hum
Biol l987;59:299-309.
by on Decem
ber 24, 2007 w
ww
.ajcn.orgD
ownloaded from