Embed Size (px)
Citation preview

TuberculosisTuberculosis
Richard H. SimonRichard H. SimonPulmonary and Critical Care MedicinePulmonary and Critical Care MedicineDepartment of Internal MedicineDepartment of Internal Medicine
[email protected]@umich.edu
764-4554764-4554

Objectives: To UnderstandObjectives: To Understand
When TB belongs in the differential When TB belongs in the differential diagnosis of a patient presenting with diagnosis of a patient presenting with pulmonary symptomspulmonary symptoms
The tests used to diagnose TBThe tests used to diagnose TB
Isolation of patients with TBIsolation of patients with TB
Treatment of active TBTreatment of active TB
Diagnosis and treatment of latent TBDiagnosis and treatment of latent TB

Case History - 1Case History - 1
43 y.o. female with a 10 day history 43 y.o. female with a 10 day history of:of:– Cough, producing yellow sputumCough, producing yellow sputum– Fever and night sweatsFever and night sweats– Mild shortness of breathMild shortness of breath– FatigueFatigue– Loss of appetiteLoss of appetite

Diagnostic QuestionsDiagnostic Questions
Is the cause of symptoms likely to be Is the cause of symptoms likely to be infection?infection?
If so, could this be tuberculosis?If so, could this be tuberculosis?
Why is it important to make a decision if Why is it important to make a decision if tuberculosis belongs on differential tuberculosis belongs on differential diagnosis list?diagnosis list?

Common Symptoms of Pulmonary TBCommon Symptoms of Pulmonary TB
Cough and sputum productionCough and sputum production– Usually insidious onset, increasing over Usually insidious onset, increasing over
weeks to monthsweeks to months– Less commonly, acute onset with rapid Less commonly, acute onset with rapid
progressionprogression– Hemoptysis frequentHemoptysis frequent
Fever, night sweatsFever, night sweats Anorexia, weight lossAnorexia, weight loss

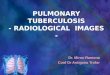
Common Radiological Common Radiological FeaturesFeatures of TB of TB
Primary diseasePrimary disease– Parenchymal infiltrateParenchymal infiltrate– Ipsilateral hilar node enlargementIpsilateral hilar node enlargement
Reactivation diseaseReactivation disease– Upper lobe (apical posterior)Upper lobe (apical posterior)
InfiltrateInfiltrate CavityCavity
Pleural diseasePleural disease In HIV, “atypical” appearances frequent, In HIV, “atypical” appearances frequent, e.g e.g
hilar/mediastinal lymphadenopathy onlyhilar/mediastinal lymphadenopathy only

Deciding Whether to Keep Tuberculosis in Deciding Whether to Keep Tuberculosis in the Differential Diagnosisthe Differential Diagnosis
Use demographic information to adjust Use demographic information to adjust probably that patient has tuberculosisprobably that patient has tuberculosis– Consider likelihood of prior contact with Consider likelihood of prior contact with
tuberculosistuberculosis– Consider likelihood of developing active Consider likelihood of developing active
disease, if previously infecteddisease, if previously infected

Incidence of Tuberculosis in USIncidence of Tuberculosis in US 1953 - 19991953 - 1999
00
1010
2020
3030
4040
5050
6060
19501950 19601960 19701970 19801980 19901990 20002000
Inci
den
ce /
100,
000
po
pu
lati
on
Inci
den
ce /
100,
000
po
pu
lati
on

Reported TB Cases Reported TB Cases United States, 1982-2002United States, 1982-2002
YearYear
No
. o
f C
ases
No
. o
f C
ases
1000010000
1200012000
1600016000
2000020000
2400024000
2800028000
8383 8585 8787 8989 9191 9393 9595 9797 9999 20012001

TB MorbidityTB MorbidityUnited States, 1998-2002United States, 1998-2002
YearYear Cases Cases Rate* Rate*
19981998 18,361 18,361 6.8 6.819991999 17,531 17,531 6.4 6.420002000 16,377 16,377 5.8 5.820012001 15,989 15,989 5.6 5.620022002 15,075 15,075 5.2 5.2
*Cases per 100,000*Cases per 100,000

TB Case Rates, United States, 2002TB Case Rates, United States, 2002
<< 3.5 (year 2000 target) 3.5 (year 2000 target)
3.6 - 5.23.6 - 5.2
> 5.2 (national average)> 5.2 (national average)
D.C.D.C.
Rate: cases per 100,000Rate: cases per 100,000

TB Case Rates by Age Group TB Case Rates by Age Group United States, 1992-2002United States, 1992-2002
0
5
10
15
20
1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002
<15 15-24 25-44 45-64 65+
Age Group (years)Age Group (years)
Ca
ses
per
10
0,0
00C
as
es p
er 1
00,
000

Number of TB Cases inNumber of TB Cases inU.S.-born vs. Foreign-born Persons U.S.-born vs. Foreign-born Persons 1992-20021992-2002
0
5000
10000
15000
20000
1992 1994 1996 1998 2000 2002
U.S.-born Foreign-born
No
. o
f C
ases
No
. o
f C
ases

>>50%50%25%-49%25%-49%<25%<25%
19921992 20022002
Percentage of TB Cases Among Percentage of TB Cases Among Foreign-born PersonsForeign-born Persons

Countries of Birth for Foreign-born Persons Countries of Birth for Foreign-born Persons Reported with TB Reported with TB United States, 2002United States, 2002
MexicoMexico(25%)(25%)
PhilippinesPhilippines(11%)(11%)
VietnamVietnam(8%)(8%)IndiaIndia
(7%)(7%)ChinaChina(5%)(5%)
HaitiHaiti(3%)(3%)
S. KoreaS. Korea(3%)(3%)
OtherOtherCountriesCountries
(38%)(38%)

Length of U.S. Residence Prior to TB Length of U.S. Residence Prior to TB Diagnosis, United States, 2002Diagnosis, United States, 2002
0%
20%
40%
60%
80%
100%
All Philippines Mexico Vietnam
<1 yr 1- 4 yrs >5 yrs

TB Incidence by IncomeTB Incidence by Income
00
1010
2020
3030
4040In
cid
ence
/ 1
00,0
00 /
yr
Inci
den
ce /
100
,000
/ y
r
$10,000$10,000 $20,000$20,000 $30,000$30,000
IncomeIncome

Use of Skin Test in Diagnosis of Use of Skin Test in Diagnosis of Active TBActive TB
Reactivity indicates:Reactivity indicates:
– Past exposure to TB, orPast exposure to TB, or
– False positiveFalse positive
Absence of reactivity doesn’t exclude active Absence of reactivity doesn’t exclude active TBTB
– < 10 mm induration seen in up to ~20% of active < 10 mm induration seen in up to ~20% of active TB patientsTB patients

Case History - 2Case History - 2
Patient recent immigrant Patient recent immigrant from Southeast Asiafrom Southeast Asia
History of 15 mm PPD History of 15 mm PPD reactionreaction
Chest x-ray shows right Chest x-ray shows right upper lobe cavitaryupper lobe cavitary
Therefore, tuberculosis Therefore, tuberculosis likely -- initiate treatmentlikely -- initiate treatment

Sputum Evaluation for Diagnosis of TBSputum Evaluation for Diagnosis of TB
SmearSmear– Techniques:Techniques:
Kinyon or Ziehl-Neelsen stainKinyon or Ziehl-Neelsen stain Auramine/rhodamine stainAuramine/rhodamine stain
– False negative smears commonFalse negative smears common– False positive smears can occurFalse positive smears can occur
Nucleic acid amplification testsNucleic acid amplification tests CultureCulture

Culture for M. tuberculosisCulture for M. tuberculosis
Organisms grow slowlyOrganisms grow slowly
Species identificationSpecies identification– Colony morphology (weeks)Colony morphology (weeks)– Nucleic acid probes after micro-colonies Nucleic acid probes after micro-colonies
appear (1-2 additional days)appear (1-2 additional days)– Biochemical analyses after macro-colonies Biochemical analyses after macro-colonies
appear (1 day)appear (1 day)

Case History - 3Case History - 3
Positive smear for acid fast bacillusPositive smear for acid fast bacillus
Positive nucleic acid amplification test for Positive nucleic acid amplification test for M. tuberculosisM. tuberculosis
Diagnosis confirmed, treatment continuesDiagnosis confirmed, treatment continues

Short Course Chemotherapy for Short Course Chemotherapy for Active TuberculosisActive Tuberculosis
First 2 months:First 2 months:– IsoniazidIsoniazid– Rifampin Rifampin (beware of complex interactions with drugs used to treat (beware of complex interactions with drugs used to treat
HIV)HIV)
– PyrazinamidePyrazinamide– EthambutolEthambutol or Streptomycin (if chance of drug resistant or Streptomycin (if chance of drug resistant
organisms >4%)organisms >4%)
Final 4 monthsFinal 4 months– IsoniazidIsoniazid– RifampinRifampin
A subset of patient should be extend their treatment A subset of patient should be extend their treatment of a total of 9 monthsof a total of 9 months

Adherence to TreatmentAdherence to Treatment
Nonadherence is a major problem in Nonadherence is a major problem in TB controlTB control
Use case management and directly Use case management and directly observed therapy (DOT) to ensure observed therapy (DOT) to ensure patients complete treatmentpatients complete treatment

Public Health Considerations - 1Public Health Considerations - 1
Has patient infected others?Has patient infected others?– Assume “yes”, and evaluate contacts (skin Assume “yes”, and evaluate contacts (skin
test)test)– Factors making transmission more likelyFactors making transmission more likely
Infectiousness of person with TBInfectiousness of person with TB Actively coughingActively coughing Cavitary diseaseCavitary disease Smear positiveSmear positive
Poorly ventilated environmentPoorly ventilated environment Duration of exposureDuration of exposure

Public Health Considerations - 2Public Health Considerations - 2
Where should patient be isolated?Where should patient be isolated?
– Goal of isolationGoal of isolation Minimize new contactsMinimize new contacts Minimize continuing exposure to children Minimize continuing exposure to children
or highly susceptible personsor highly susceptible persons
– Isolation at home permissible, if above Isolation at home permissible, if above goals are metgoals are met

Public Health Considerations - 3Public Health Considerations - 3
Patients no longer considered Patients no longer considered infectious if they meet infectious if they meet allall of these of these criteria:criteria:
– On adequate therapyOn adequate therapy
– Demonstrating a significant clinical Demonstrating a significant clinical response to therapyresponse to therapy
– Have had 3 consecutive negative sputum Have had 3 consecutive negative sputum smear resultssmear results

Preventing New Cases of Preventing New Cases of ActiveActive TuberculosisTuberculosis
Prevent new infections Prevent new infections
Prevent reactivation of latent Prevent reactivation of latent infectionsinfections

Preventing New InfectionsPreventing New Infections
Eliminate the source of infectious Eliminate the source of infectious organismsorganisms
– Identify and treat patients with active diseaseIdentify and treat patients with active disease
Implement effective TB control measures Implement effective TB control measures at high risk locationsat high risk locations
– Decrease chances that a non-infected person Decrease chances that a non-infected person inhales viable TB bacteria ( = good inhales viable TB bacteria ( = good ventilation)ventilation)

Preventing Reactivation of Latent Preventing Reactivation of Latent InfectionsInfections
Identify previously infected Identify previously infected individuals, particularly those most individuals, particularly those most likely to reactive their latent infectionlikely to reactive their latent infection
Treat latent TB infection when Treat latent TB infection when benefits outweigh risks of treatmentbenefits outweigh risks of treatment

Identifying Previously Infected Identifying Previously Infected Individuals -- PPD Skin TestIndividuals -- PPD Skin Test
Highly accurate in majority of peopleHighly accurate in majority of people
False positivesFalse positives
– Previous exposure to non-tuberculous mycobacteriaPrevious exposure to non-tuberculous mycobacteria
– Previous vaccination with BCGPrevious vaccination with BCG
False negatives False negatives (anergic to PPD antigen)(anergic to PPD antigen)
– CachexiaCachexia
– Immunosuppressed (particularly HIV infection)Immunosuppressed (particularly HIV infection)

Identify Previously Infected Individuals Identify Previously Infected Individuals -- PPD Skin Test-- PPD Skin Test
Use smaller induration cut-off when: Use smaller induration cut-off when:
– Likelihood of TB infection is higherLikelihood of TB infection is higher
– Likelihood of re-activating latent disease is higherLikelihood of re-activating latent disease is higher
Use larger induration cut-off when:Use larger induration cut-off when:
– Likelihood of infection is lowerLikelihood of infection is lower
– Likelihood of re-activation is lowerLikelihood of re-activation is lower

Incidence of Reactivating TB in Previously Incidence of Reactivating TB in Previously Infected Patients (+ PPD)Infected Patients (+ PPD)
TB cases / 1,000 person-yearsTB cases / 1,000 person-years
No additional risk factorsNo additional risk factors 0.80.8 HIV infectionHIV infection 35 - 16235 - 162 Recent TB infectionRecent TB infection
– Infection < 1 yr pastInfection < 1 yr past 25-3025-30– Infection 1-7 pastInfection 1-7 past 10-2010-20
IV drug usersIV drug users 1010 CXR evidence of old TBCXR evidence of old TB 2 - 142 - 14

Treatment Regimens for Latent Tuberculosis Treatment Regimens for Latent Tuberculosis InfectionInfection
IsoniazidIsoniazid 6 - 6 - 99 months months
Rifampin and pyrazinamideRifampin and pyrazinamide 2 months2 months(Higher incidence of liver toxicity(Higher incidence of liver toxicityin non HIV-infected patients)in non HIV-infected patients)
RifampinRifampin 4 months4 months

Treatment of Latent TB InfectionTreatment of Latent TB Infection
Highly effective at killing bacteriaHighly effective at killing bacteria
Major side effect: Hepatitis (age related for INH)Major side effect: Hepatitis (age related for INH)
Guidelines for decision to treat based on:Guidelines for decision to treat based on:
– Likelihood that a positive skin test is a true positiveLikelihood that a positive skin test is a true positive
– Likelihood that the patient will progress to active Likelihood that the patient will progress to active diseasedisease
– Likelihood that patient will develop hepatitisLikelihood that patient will develop hepatitis

Candidates for Treatment of Latent TB InfectionCandidates for Treatment of Latent TB Infection
Based on PPD ResultBased on PPD Result
>> 5 mm 5 mm
– HIV- positive personsHIV- positive persons
– Close contacts of persons known or Close contacts of persons known or suspected of having TBsuspected of having TB
– Fibrotic changes on chest x-ray suggesting Fibrotic changes on chest x-ray suggesting past TBpast TB
– Patients with organ transplantsPatients with organ transplants
– Immunosuppressed patientsImmunosuppressed patients

Candidates for Treatment of Latent TB InfectionCandidates for Treatment of Latent TB InfectionBased on PPD ResultBased on PPD Result
>> 10 mm 10 mm– Immigrants ( Immigrants ( w/i 5 yrsw/i 5 yrs) from high prevalence countries) from high prevalence countries– Intravenous drug usersIntravenous drug users– Residents and employees of high risk settingsResidents and employees of high risk settings
PrisonsPrisons Nursing homesNursing homes Health care facilitiesHealth care facilities
– Mycobacteriology laboratory personnelMycobacteriology laboratory personnel– Children < 4 years of ageChildren < 4 years of age– Children and adolescents exposed to adults at high riskChildren and adolescents exposed to adults at high risk– Persons with medical conditions that increase risk of TB Persons with medical conditions that increase risk of TB
reactivationreactivation

Medical Conditions Associated Medical Conditions Associated with TB Reactivationwith TB Reactivation
SilicosisSilicosis Gastrectomy or jejunoileal bypassGastrectomy or jejunoileal bypass Body weight 10% or more below ideal levelBody weight 10% or more below ideal level Chronic renal failureChronic renal failure Diabetes mellitusDiabetes mellitus Prolonged use of corticosteroid or other Prolonged use of corticosteroid or other
immunosuppressive drugsimmunosuppressive drugs Certain hematological conditions, e.g. leukemia Certain hematological conditions, e.g. leukemia
and lymphomasand lymphomas Other malignanciesOther malignancies

Candidates for Treatment of Latent TB InfectionCandidates for Treatment of Latent TB InfectionBased on PPD Result (?)Based on PPD Result (?)
>> 15 mm 15 mm
– Persons with no risk actors*Persons with no risk actors*
– Controversial whether this group Controversial whether this group benefits from therapybenefits from therapy
* Don’t skin test this group* Don’t skin test this group

Before Treatment for LTBI Is Started...Before Treatment for LTBI Is Started...
Rule out possibility of active TB diseaseRule out possibility of active TB disease– Screen for fever, cough, sputum production, Screen for fever, cough, sputum production,
weight lossweight loss
– Check chest x-ray for evidence of active diseaseCheck chest x-ray for evidence of active disease
Obtain information about current and Obtain information about current and previous drug therapy previous drug therapy
Determine contraindications to treatmentDetermine contraindications to treatment Recommend HIV testing if risk factors are Recommend HIV testing if risk factors are
presentpresent

Reference:Reference:
http://www.cdc.gov/nchstp/tb/http://www.cdc.gov/nchstp/tb/pubs/mmwrhtml/maj_guide.htmpubs/mmwrhtml/maj_guide.htm