Embed Size (px)
Citation preview
Konstantinos Anastassakis MD, PhDHead & Neck Surgeon
Hair Transplant Surgeon
Trading Places!An FUE surgeon
becomes an FUE Patient
(and re-evaluates)

How I looked back in 2008, before my 1st
FUE session

Not THAT bad after all…

HOW my HT transformed my practice!
2004-2012: 80% FUE / 20% strip 2012>: 20% FUE / 80% strip

2 main HR techniques
The old (FUT, strip) and the young (FUE)

The only difference?
How we harvest the grafts
(BUT it makes ALL the difference!)
How I approached my decision:(as a Hair Transplant Surgeon)
1. I do NOT want a visible scar (in case I want I shaved look)
2. I do NOT want the “strip pain”
3. I do NOT want transected nerves-numbness, cut vessels-bleeding or stitches
4. I do NOT want a lengthy down-time from the gym
How I would have approached it (if I were not a surgeon)
1. Newer technique
2. No pain (!)
3. No stitches
4. Less time till the next session (!)
(THIS IS HOW OUR PATIENTS
MAKE A CHOICE!!!!)

Winner…FUE! (in both situations)
FUE drawbacks(at least the ones I knew as a surgeon…)
1. Donor area shaving
2. Larger scar surface (Not scarless but scarspreading)
3. Blind technique
4. Lower survival rate
5. Scared donor area left behind

1. Donor area shaving
Before my 2nd session
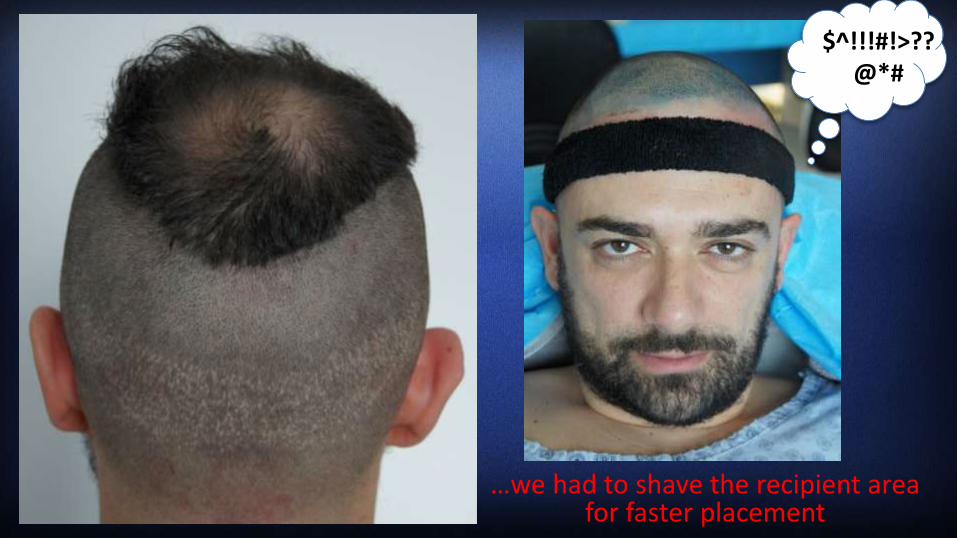
…we had to shave the recipient areafor faster placement
$^!!!#!>??@*#

This was my look for
manymonths…
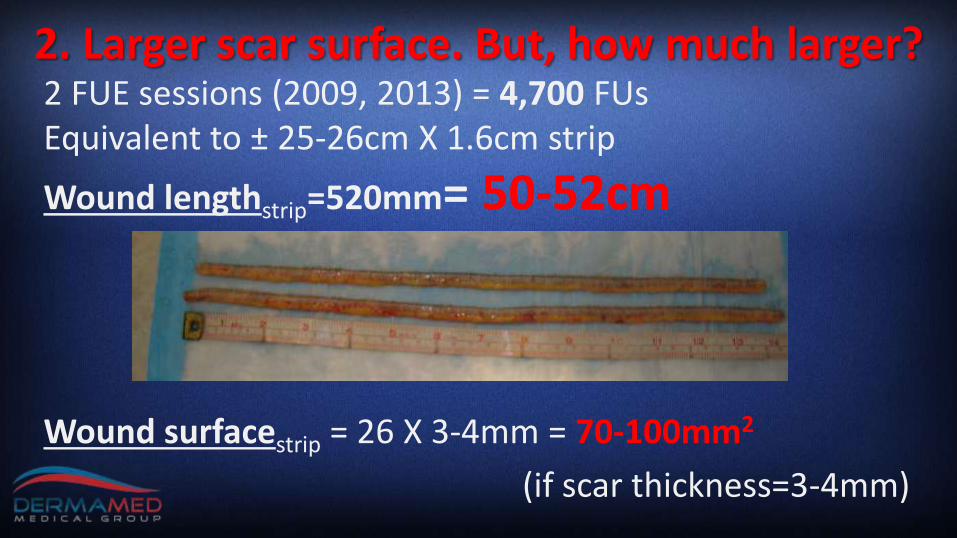
2 FUE sessions (2009, 2013) = 4,700 FUs Equivalent to ± 25-26cm X 1.6cm strip
Wound lengthstrip=520mm= 50-52cm
Wound surfacestrip = 26 X 3-4mm = 70-100mm2
(if scar thickness=3-4mm)
2. Larger scar surface. But, how much larger?

2. Larger scar surface. But, how much larger?
1. Wound lengthFUE
2πR=2 X 3.14 X 0.5=
3.14mm X 4,700FUs=
14,800mm = 14.8meters!
2. Wound surfaceFUE
πR2=3.14 X 0.52=0.785mm2
0.785 X 4,700= 3,690mm2
= 6cm Χ 6cm

14.8m = 4 stories building
Not scar-less but scar spreading…
3,690mm2 = 6cm Χ 6cm =
5euros bill folded exactly in half!

3. Blind technique
Strip FUTAll steps are under high magnification vision
FUE

…but some grafts won’t make it at the end…
FUE is promising in theory…
4. Lower survival rate
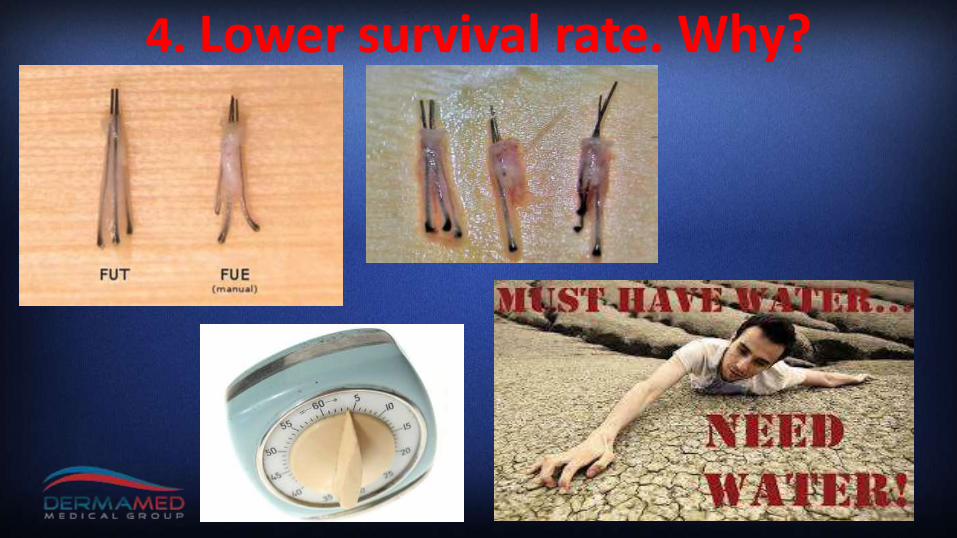
4. Lower survival rate. Why?

After an FUT session
Future FUE or FUT sessions are very hard after FUE
5. Scarred donor area is left behind
Donor area can be easily re-harvested after FUT
After an FUE session
So, what have I learned…
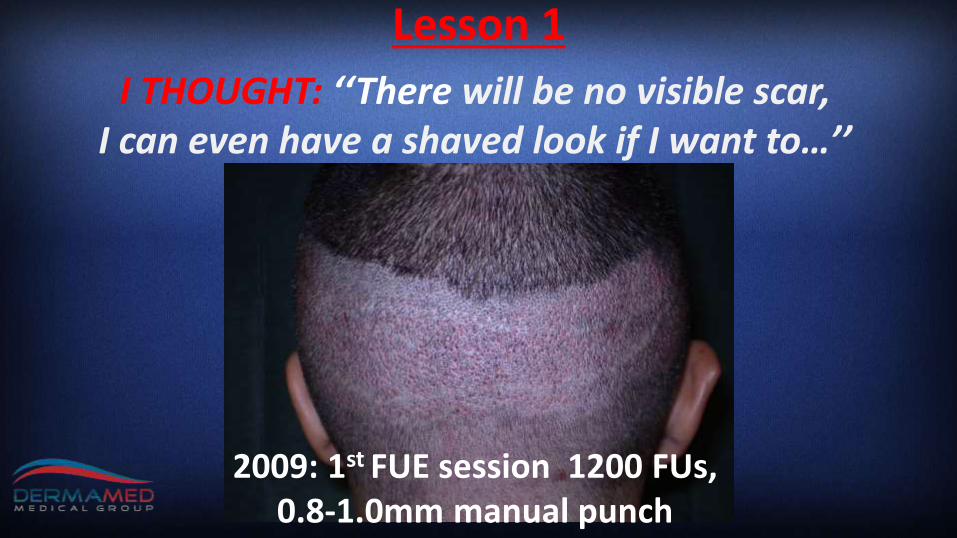
2009: 1st FUE session 1200 FUs, 0.8-1.0mm manual punch
I THOUGHT: ‘‘There will be no visible scar, I can even have a shaved look if I want to…’’
Lesson 1

White spots from the 1st session were visible!
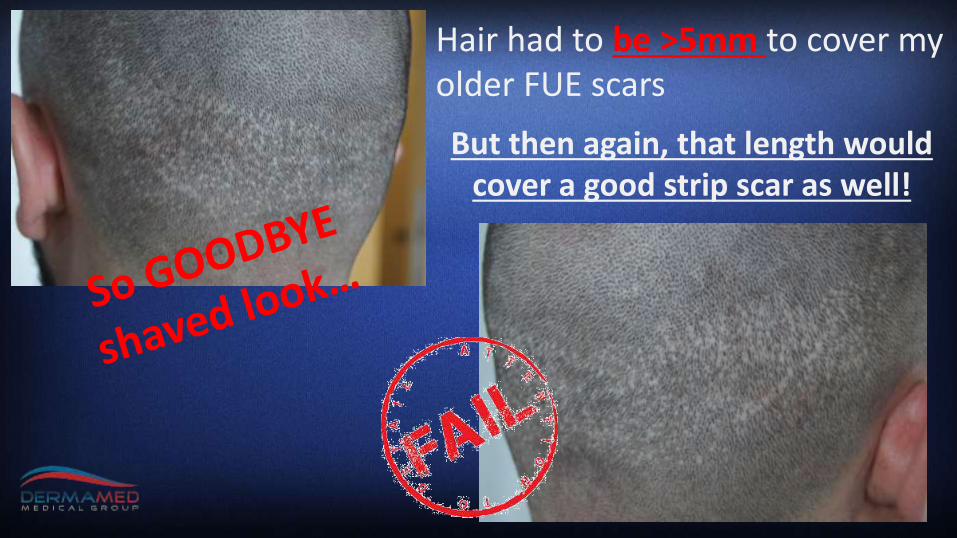
Hair had to be >5mm to cover my older FUE scars
But then again, that length would cover a good strip scar as well!

10 days
5 days
Lesson 2I THOUGHT: ‘‘Healing is faster…’’
30 days

Itching, pain,
redness for >60 days!

Numbness and very “touchy” for >3 months!
(WHOLE occipital area vsjust on the strip scar
edges)
I THOUGHT: ‘‘No transected nerves-numbness…’’
Lesson 3

Lesson 4I THOUGHT: ‘‘There are no complications…’’
Graft extraction is not always successful…
In grown hairs, multiple cysts for weeks!

Lesson 5The RIGHT criteria MUST be STRICTLY MEDICAL!
Maximum graft survival • All steps under direct vision • Shorter session duration• Easier for the surgeon (and patient)• One session, even one pass!

Strip + Scalp Micropigmentation if scar was ugly!
What would I do today, with what I know now?
Lesson 6My (re-evaluated) FUE indications
1. Only for limited lifetime needs (<1500FUs)
2. ONLY if FUT is impossible or contraindicated or if patient insists!
• for exhausted “safe” donor area
• for “rock rigid” donor area
• for repair of scars or for graft redistribution
• for certain professionals (athletes, etc.)
• Ehler-Danlos syndrome (or similar)
3. For cherry picking of grafts (hairline refinement, eyelashes, eyebrows, etc.)
A FACT for virgin scalps• If >1500FUs are extracted from the whole donor area
(safe+…unsafe), white-spots will be VISIBLE, no matter how well you spread the spots!
• A patient who needs <1500FUs will not shave his head ANYWAY to cover thinning, he has plenty of
hair! • So FUE scar-spreading advantage beats its own
purpose even on people who ARE candidates!

QUESTIONWHAT IS THE MEDICAL REASON for using a technique with less graft- survival (all other things equal), with 10X larger scar surface and worse downtime on patients with a virgin scalp and lifetime needs of
>1500FUs, if they will not be able to shave their heads ANYWAY due to spots?

Take home messages1. Working for years in a field does not make you
immune in taking non-optimal decisions in that SAME field!
2. I believe FUE megasessions (>1500FUs) ALWAYS compare unfavorably to FUT (all other things equal)
3. I advice you to avoid FUE if present (or lifetime needs) >1500FUs or if at least one MEDICALindication is not met.

Konstantinos Anastassakis MD, PhDHead & Neck Surgeon
Hair Restoration Surgeon