Embed Size (px)
Citation preview
Transradial approachTools and technique
1948
Radner demonstrated the feasibility of accessing thoracic aorta from the radial artery (RA) in 1948
Radner S. Thoracal aortography by catheterization from the radial artery; preliminary report of a new technique. ActaRadiol. 1948;29:178-180.
1992
Transradial access (TRA) was not used for performing CAG until 1989 and the first coronary stent was deployed in 1992
1. Campeau L. Percutaneous radial artery approach for coronary angiography. CathetCardiovasc Diagn. 1989;16:3-7.
2. Kiemeneij F, Laarman GJ. Transradial artery Palmaz-Schatz coronary stent implantation: results of a single-center feasibility study. Am Heart J. 1995;130:14-21.
Blood supply to hand
Arising from the brachial artery, the hand receives blood supply from the radial and ulnar arteries, both giving rise to superficial and deep palmar arches, from which digital branches perfuse the digits. Branches of the common interosseous artery that originate from the ulnar artery after the radial tuberosity play a crucial role in providing blood supply to the hand. The ulno-palmar arches in the hand are perfused from both the UA and RA, with a watershed point where flow from both sources meets under equal pressure. This watershed point is not static, implying that a dynamic flow volume and rate is required by the different parts of the hand at rest and upon exertion.This suggests if either the RA or UA are compromised, there is a rich network of vessels that maintains hand perfusion.
Understand the aortic arch
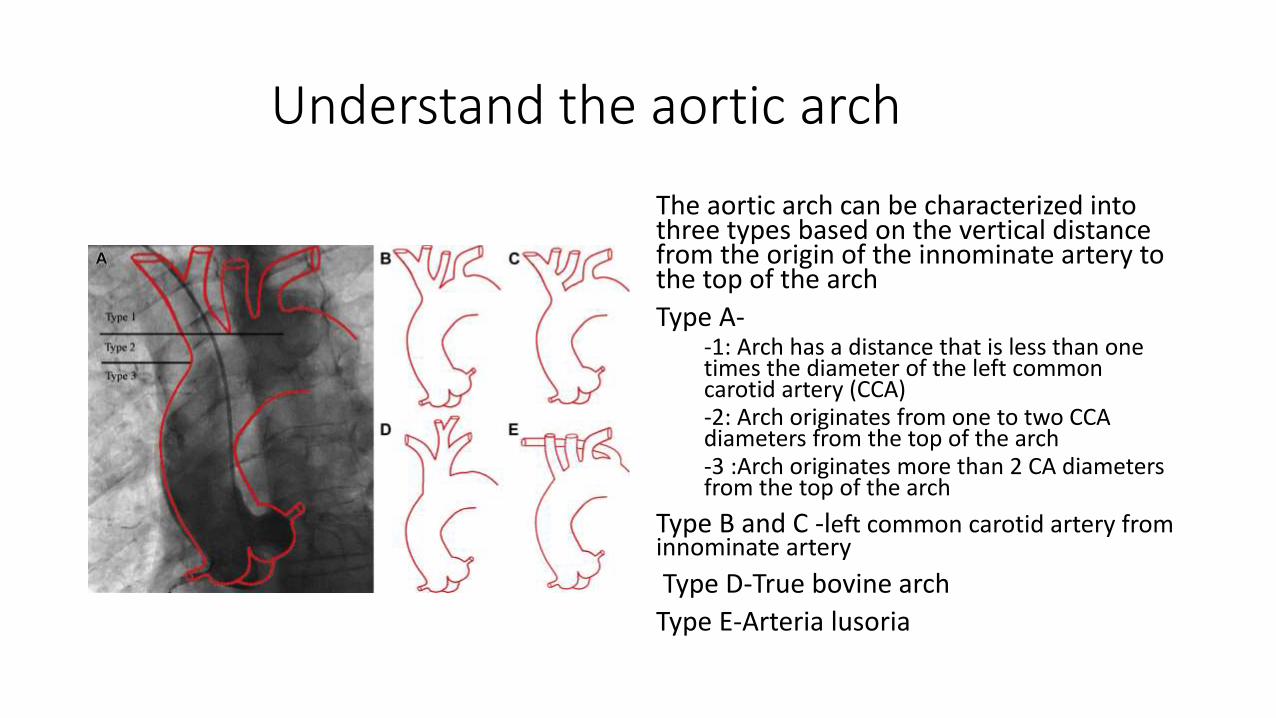
The aortic arch can be characterized into three types based on the vertical distance from the origin of the innominate artery to the top of the arch
Type A--1: Arch has a distance that is less than one times the diameter of the left common carotid artery (CCA)-2: Arch originates from one to two CCA diameters from the top of the arch-3 :Arch originates more than 2 CA diameters from the top of the arch
Type B and C -left common carotid artery from innominate artery
Type D-True bovine arch
Type E-Arteria lusoria
Barbeau test
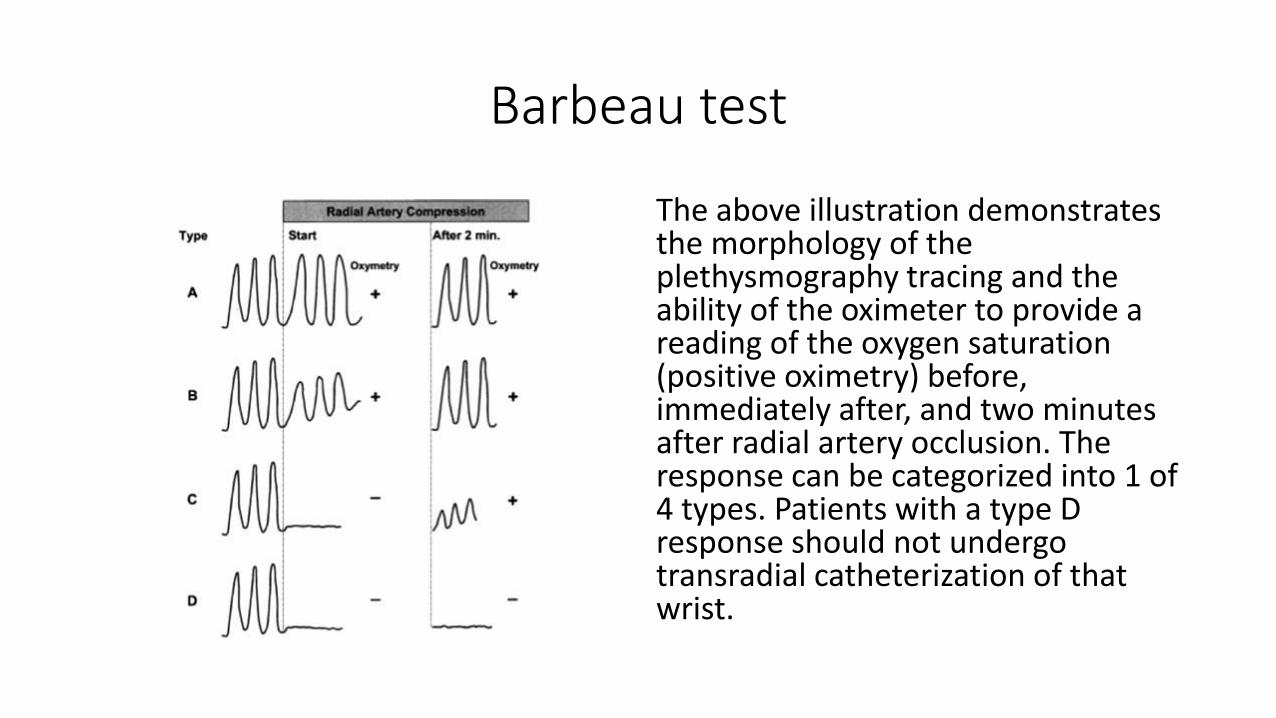
The above illustration demonstrates the morphology of the plethysmography tracing and the ability of the oximeter to provide a reading of the oxygen saturation (positive oximetry) before, immediately after, and two minutes after radial artery occlusion. The response can be categorized into 1 of 4 types. Patients with a type D response should not undergo transradial catheterization of that wrist.

Allen test
• Instruct the patient to clench his or her fist; if the patient is unable to do this, close the person's hand tightly.
• Using your fingers, apply occlusive pressure to both the ulnar and radial arteries, to obstruct blood flow to the hand.
• While applying occlusive pressure to both arteries, have the patient relax his or her hand, and check whether the palm and fingers have blanched. If this is not the case, you have not completely occluded the arteries with your fingers.
• Release the occlusive pressure on the ulnar artery only to determine whether the modified Allen test is positive or negative.
• Positive modified Allen test – If the hand flushes within 5-15 seconds it indicates that the ulnar artery has good blood flow; this normal flushing of the hand is considered to be a positive test.
• Negative modified Allen test – If the hand does not flush within 5-15 seconds, it indicates that ulnar circulation is inadequate or nonexistent; in this situation, the radial artery supplying arterial blood to that hand should not be punctured.
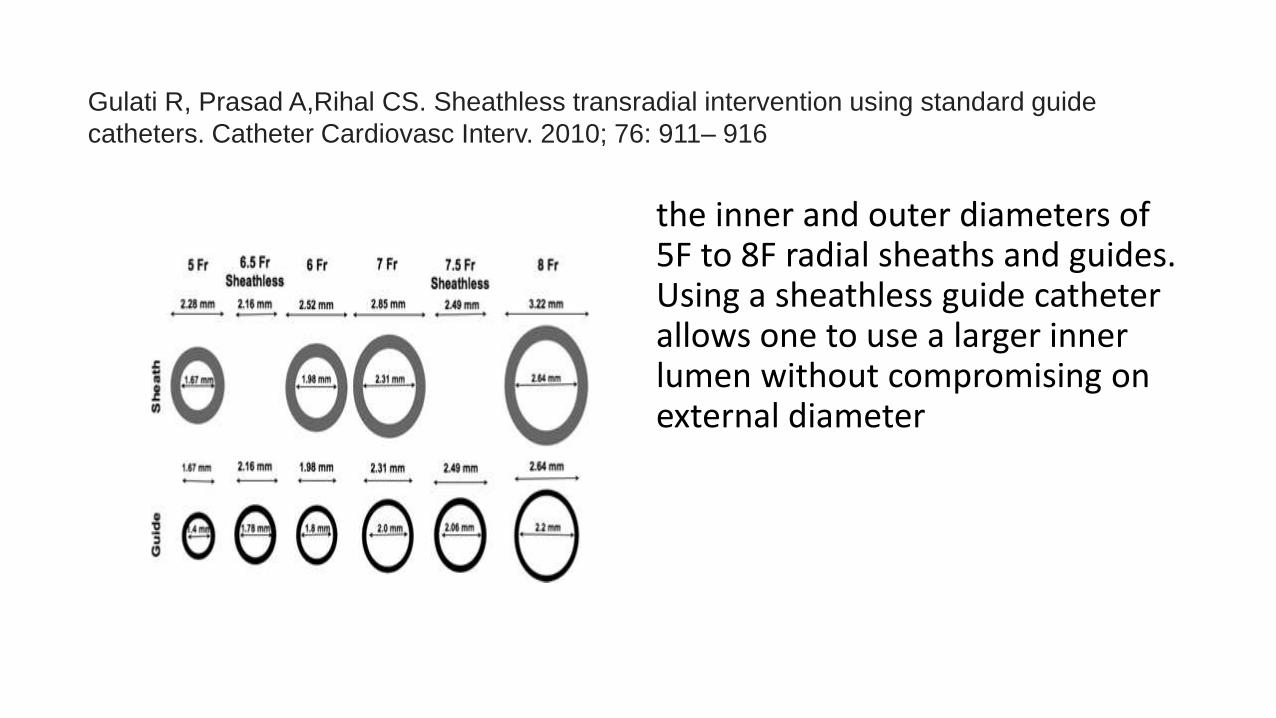
the inner and outer diameters of 5F to 8F radial sheaths and guides. Using a sheathless guide catheter allows one to use a larger inner lumen without compromising on external diameter
Gulati R, Prasad A,Rihal CS. Sheathless transradial intervention using standard guide
catheters. Catheter Cardiovasc Interv. 2010; 76: 911– 916
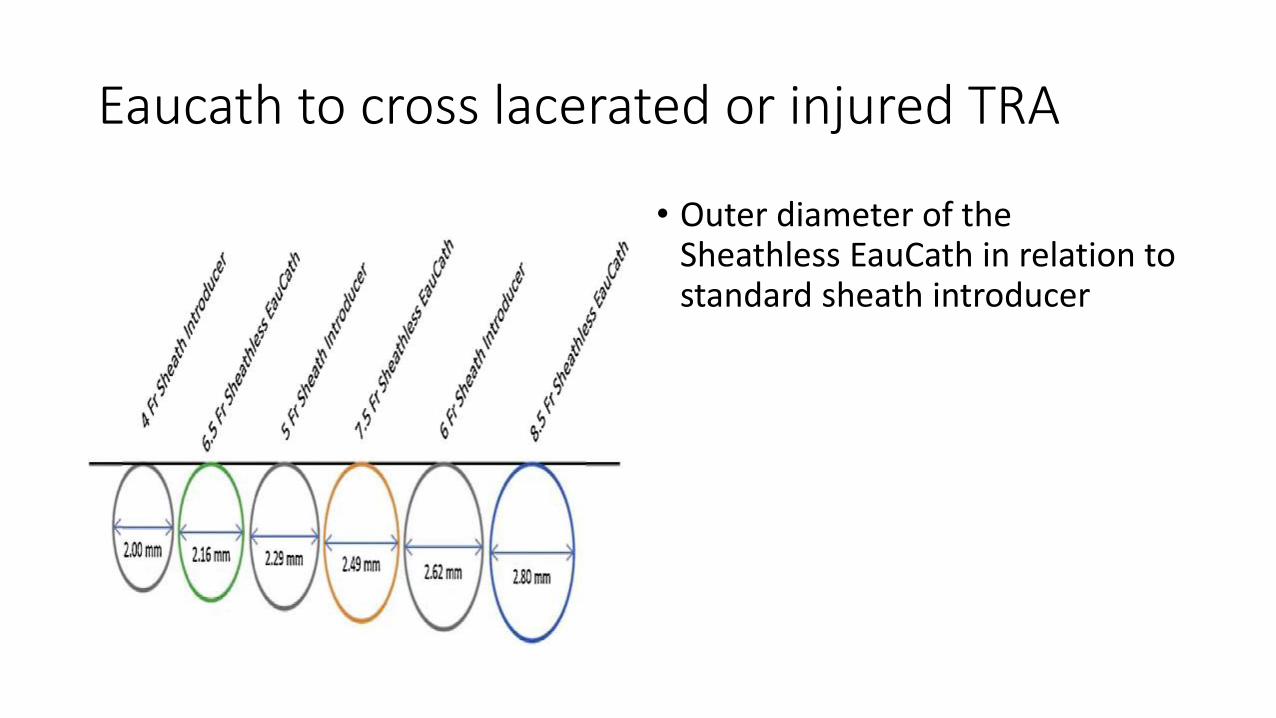
Eaucath to cross lacerated or injured TRA
• Outer diameter of the Sheathless EauCath in relation to standard sheath introducer
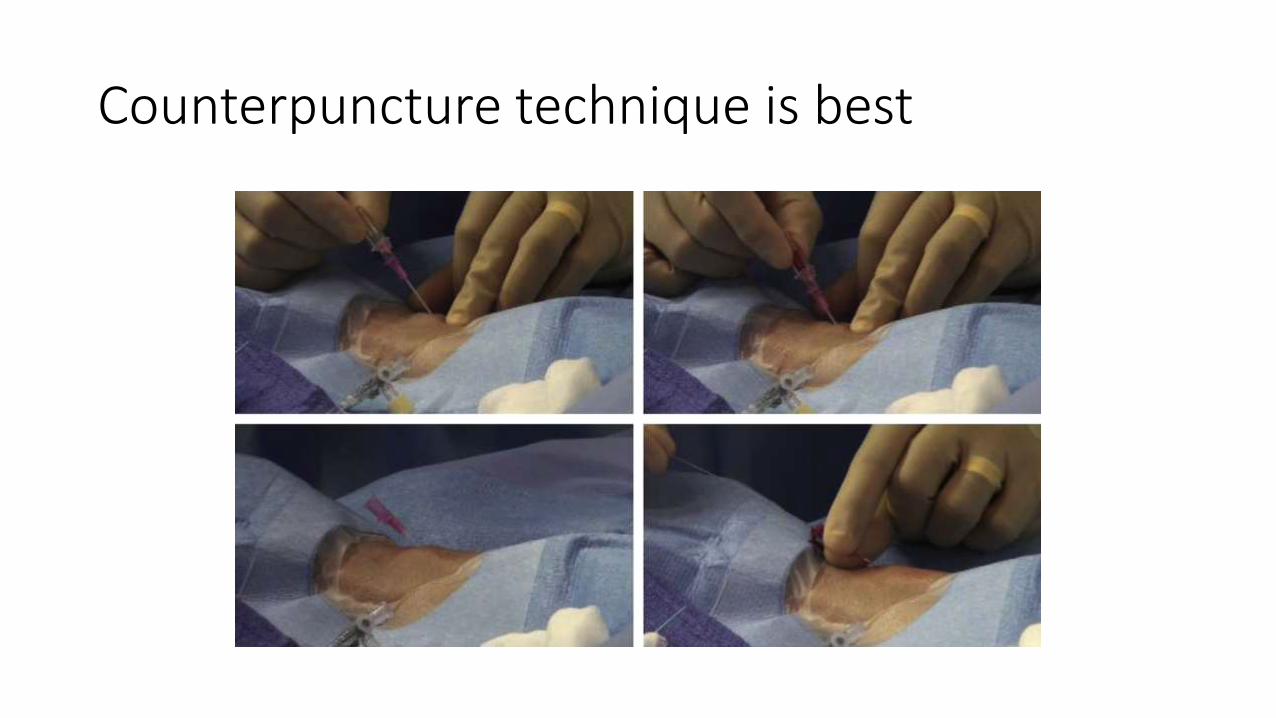
Counterpuncture technique is best
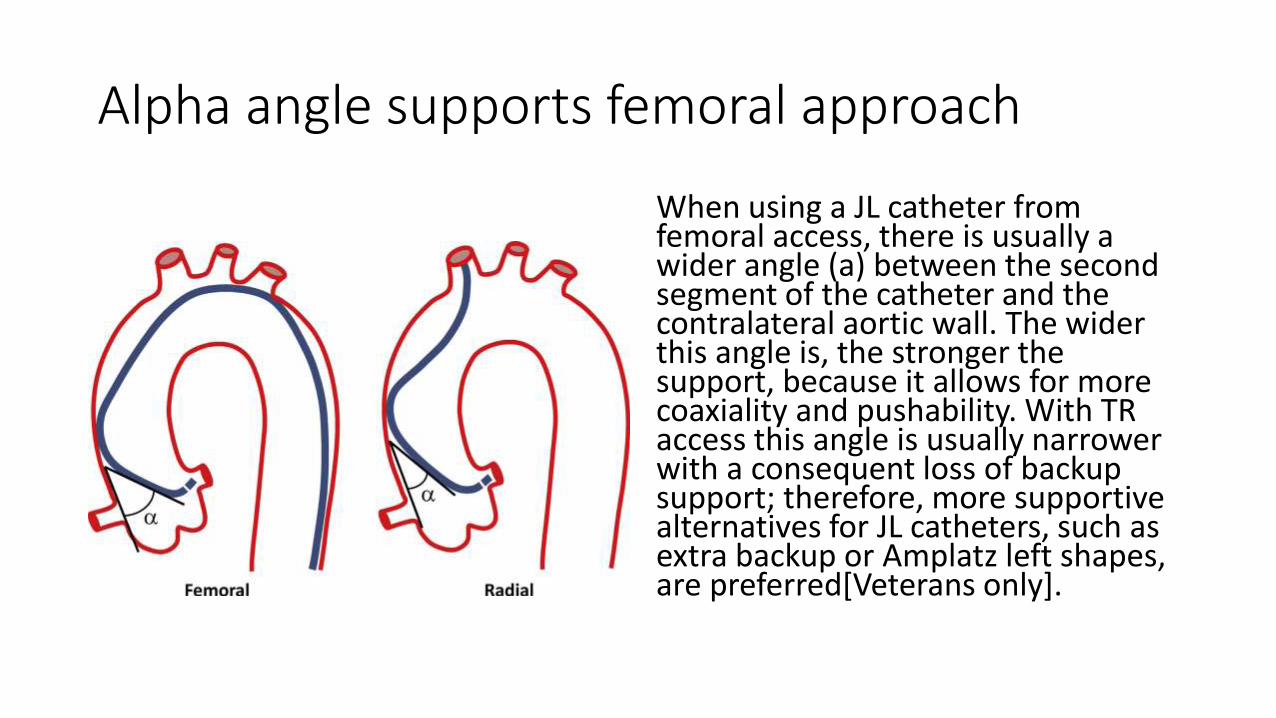
Alpha angle supports femoral approach
When using a JL catheter from femoral access, there is usually a wider angle (a) between the second segment of the catheter and the contralateral aortic wall. The wider this angle is, the stronger the support, because it allows for more coaxiality and pushability. With TR access this angle is usually narrower with a consequent loss of backup support; therefore, more supportive alternatives for JL catheters, such as extra backup or Amplatz left shapes, are preferred[Veterans only].
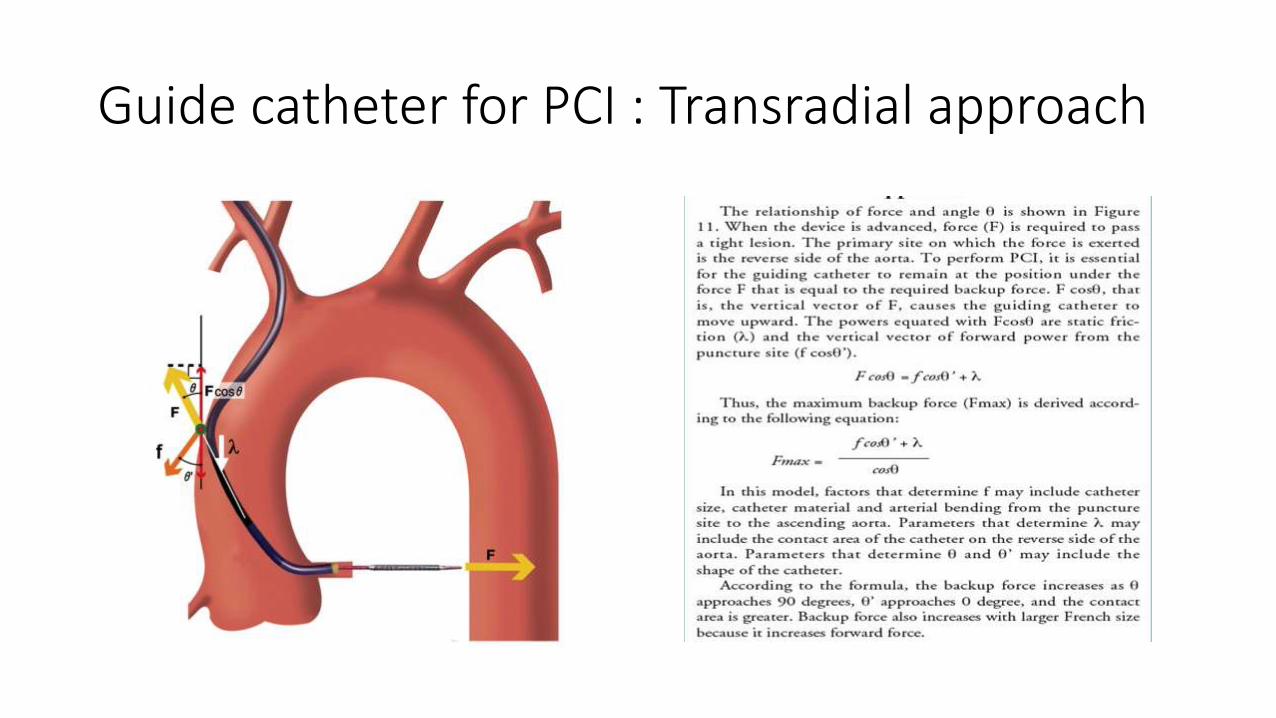
Guide catheter for PCI : Transradial approach
Sheath size for PCI
6 Fr is enough except for bifurcation stenting which needs 7 Fr sheath
Transradial cocktail
• Heparin 2500-5000 IU
• NTG 200 microgram
• Verapamil 2.5 mg
• Xylocaine 2ml of 2%
Judkin’s right
Most commonly used Easy engagement similar to TF. Weak backup support as it does not contact the contralateral aortic wall. Can be deep seated(Amplatzerisation by deep push).
AR-1
Provides some passive, but no active support.
Multipurpose
Universal catheter. Requires extensive manipulation. Ideal for right-sided bypass grafts and anomalous circumflex originating in the right coronary cusp.

Ikari left
Allows “single catheter” technique.Similar manipulation as JR, but contacts the contralateral aortic wall for support. May engage deeply at the power position.
Amplatzer left
Deep engagement. Passive support. Fits well in “shepherd’s crook” configurations. Higher risk for coronary dissection
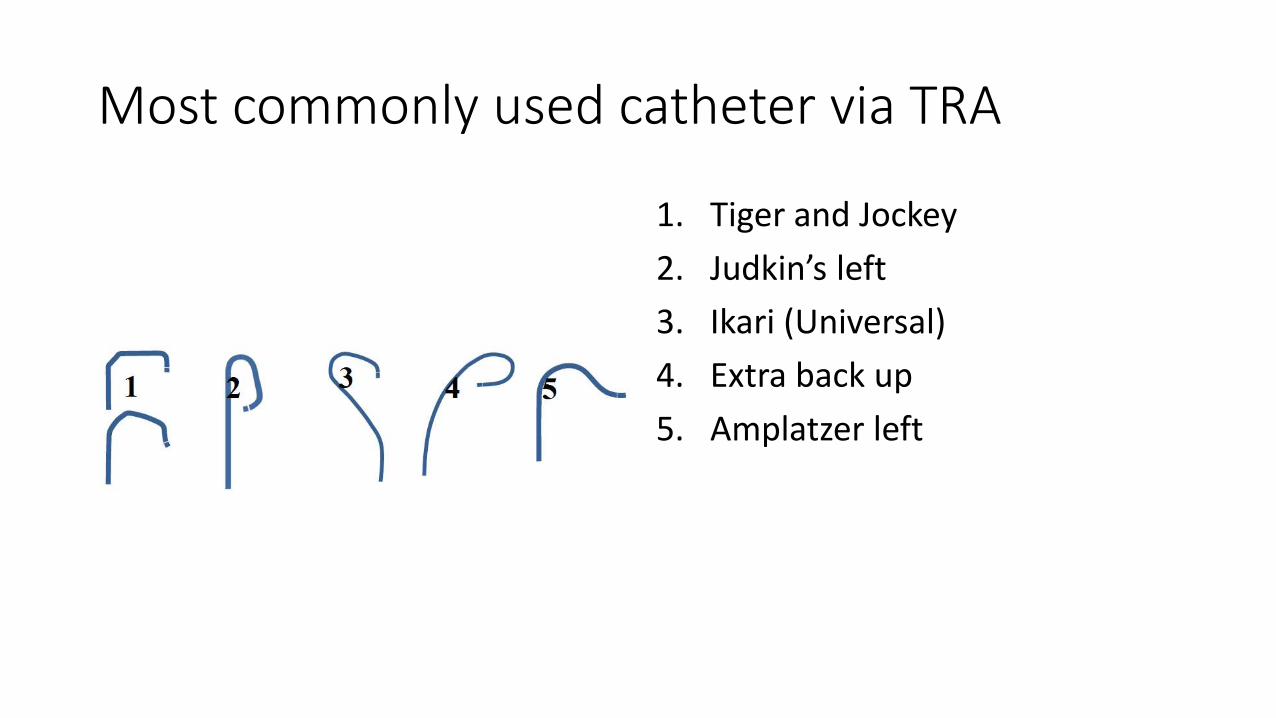
Most commonly used catheter via TRA
1. Tiger and Jockey
2. Judkin’s left
3. Ikari (Universal)
4. Extra back up
5. Amplatzer left
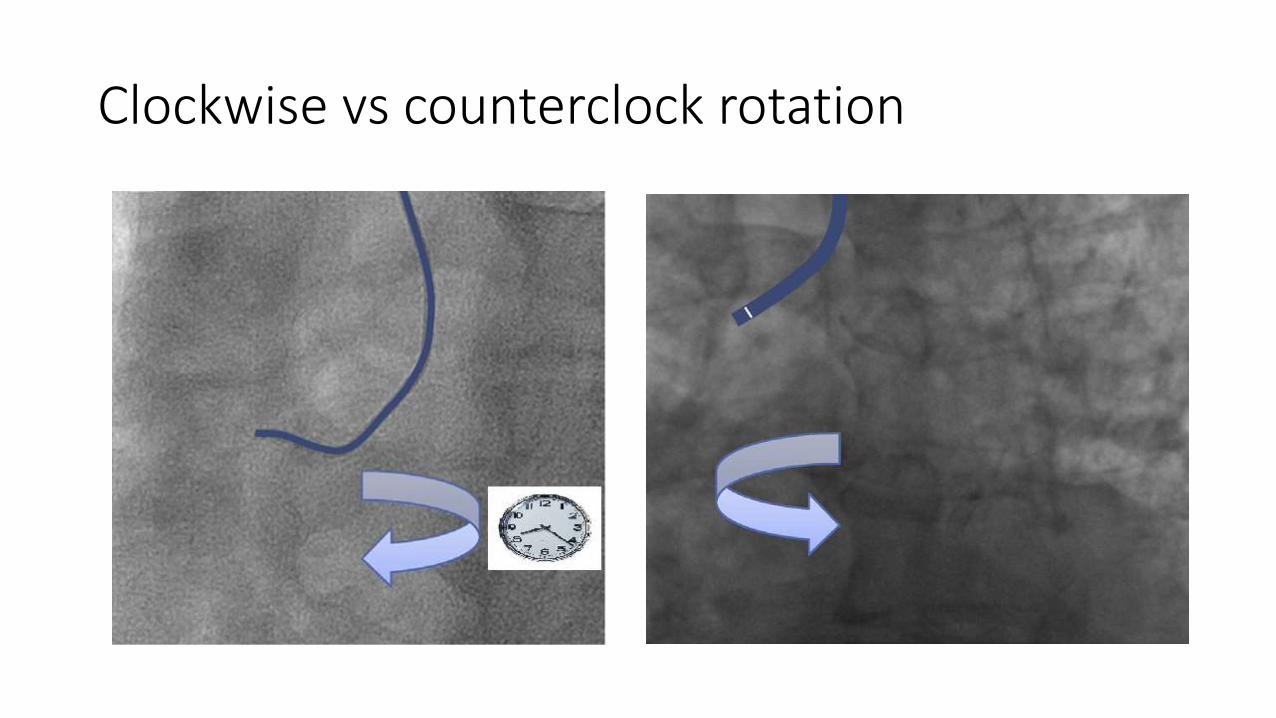
Clockwise vs counterclock rotation

Success
• Guide catheter support
Failure
• Arterial spasm
• Anatomic limitations(Loops ,tortuosity and etc.)
• Failure to cannulate the target vessel
• Inadequate guide support
Hemostasis
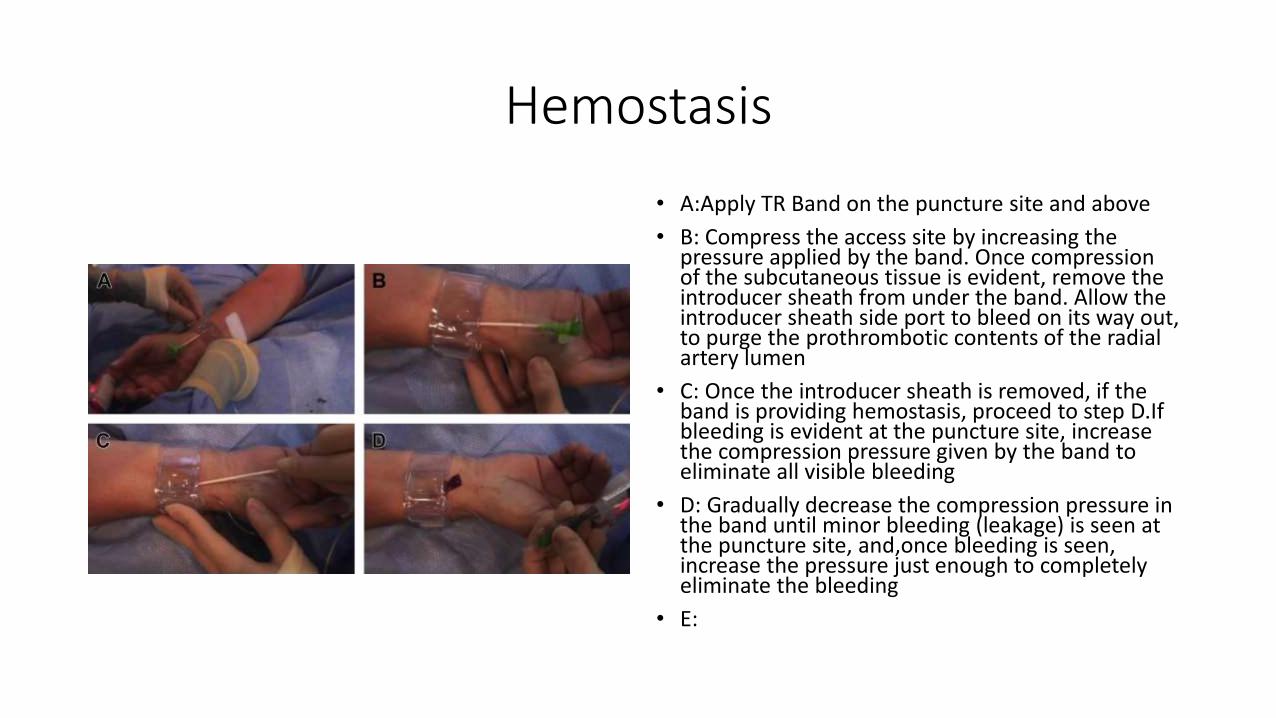
• A:Apply TR Band on the puncture site and above
• B: Compress the access site by increasing the pressure applied by the band. Once compression of the subcutaneous tissue is evident, remove the introducer sheath from under the band. Allow the introducer sheath side port to bleed on its way out, to purge the prothrombotic contents of the radial artery lumen
• C: Once the introducer sheath is removed, if the band is providing hemostasis, proceed to step D.Ifbleeding is evident at the puncture site, increase the compression pressure given by the band to eliminate all visible bleeding
• D: Gradually decrease the compression pressure in the band until minor bleeding (leakage) is seen at the puncture site, and,once bleeding is seen, increase the pressure just enough to completely eliminate the bleeding
• E:
Reverse Barbeau test
assess for presence of antegrade flow in the radial artery. If antegrade flow is present in radial artery (presence of plethysmographicwaveform on compression of ipsilateral ulnar artery), leave the band in place. If antegrade flow in radial artery is not present, titrate the pressure to the lowest needed pressure to achieve hemostasis.In the first 10 to 15 minutes of initiating hemostatic compression, due to changes in the dynamic balance of local nfluences, repeat attempts at achieving the balance of patency and hemostasis frequently succeed, even if the very initial attempt does not.
Once optimal hemostatic compression is achieved, continue to monitor the presence of radial artery patency periodically (every 15 minutes) by using reverse Barbeau test. The patient is instructed to report immediately if any bleeding is observed at the site. If radial artery patency is not achievable at the outset, despite continuous attempts, reevaluation at 15 minutes and reattempting establishment of patent hemostasis are advised.
?Routine use of Allen test is flawed
Randomized trials of TRA-PCI have excluded patients with abnormal Allen’s tests, whereas routine practice includes a large number of such patients. High-volume transradial centers worldwide document the extremely low, almost unheard of, incidence of hand ischemia after TRA without prior AT. Observations from the congenital heart disease and vascular surgery spheres lead us to conclude that AT is a misleading and inaccurate test of collateral blood supply to the hand. In our opinion, the case for its.
1. Hildick-Smith D. Use of the Allen’s test and transradial catheterization. J Am Coll Cardiol.2006;48:1287; author reply 1288.
2. Gilchrist IC. Is the Allen’s test accurate for patients considered for transradial coronary angiography? J Am Coll Cardiol. 2006;48:1287; author reply 1288.
3. Ghuran AV, Dixon G, Holmberg S, de Belder A, Hildick-Smith D. Transradial coronary intervention without pre-screening for a dual palmar blood supply. Int J Cardiol. 2007;121:320-322.
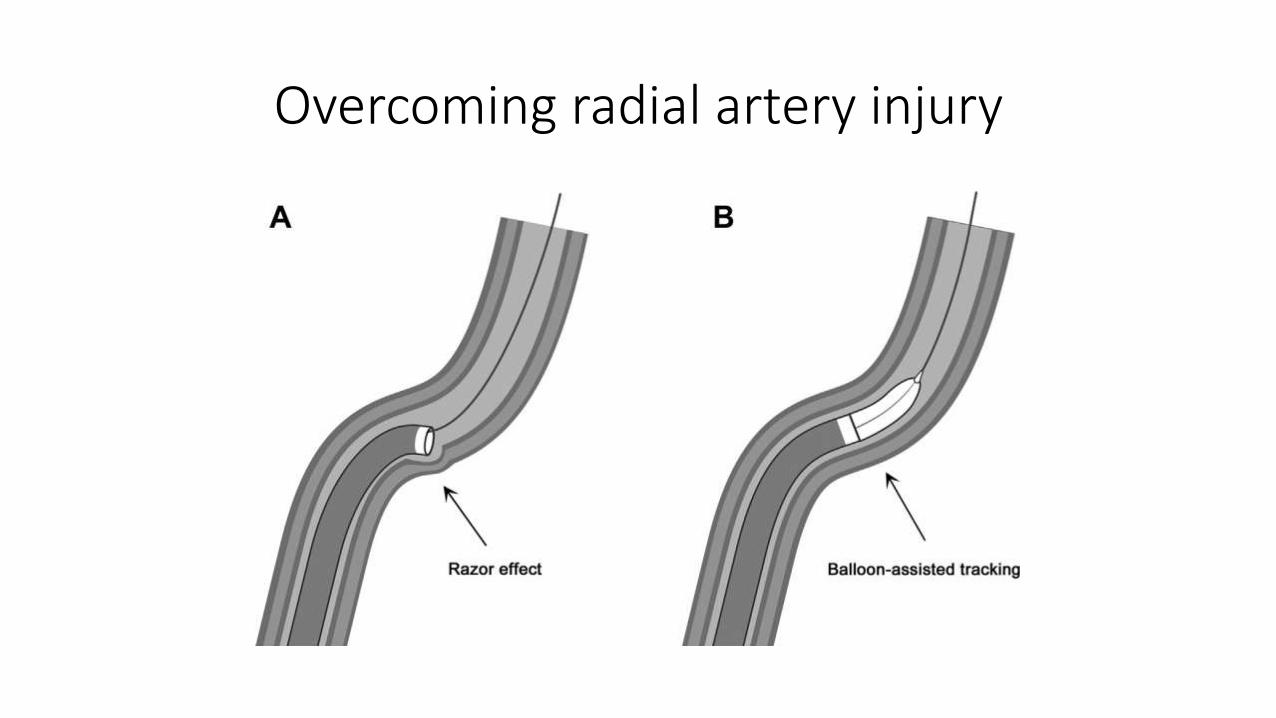
Overcoming radial artery injury
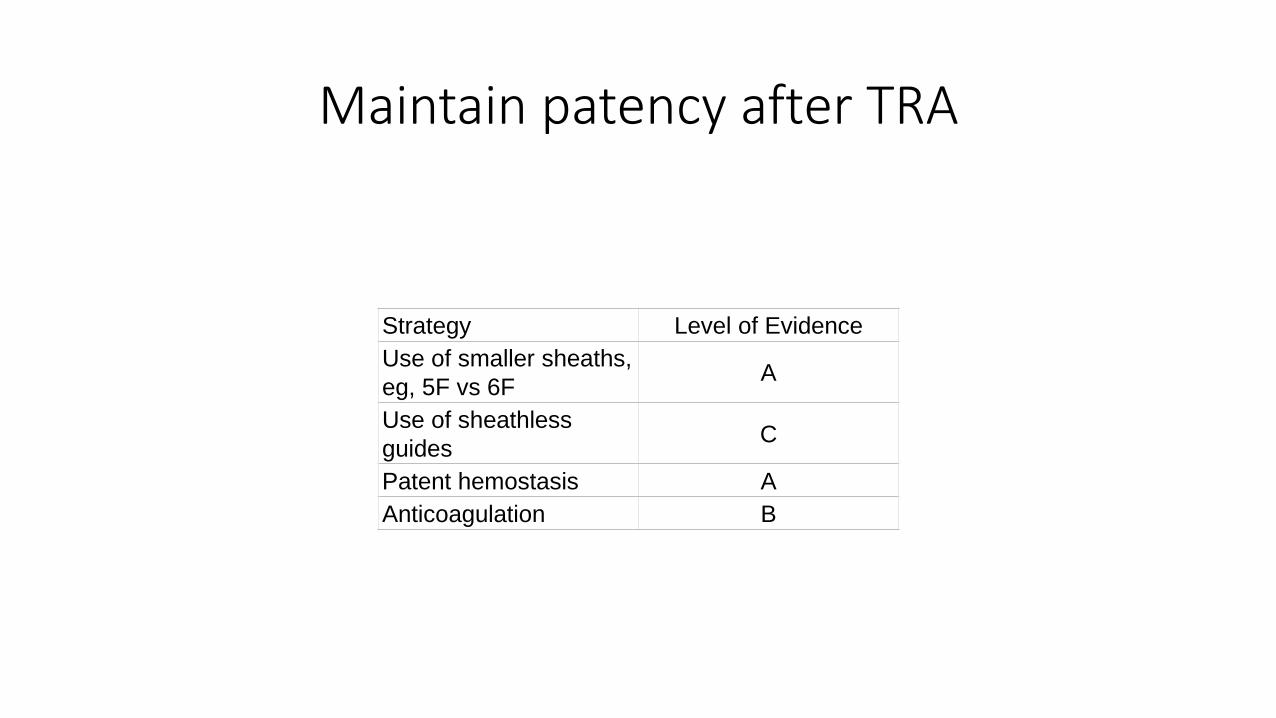
Maintain patency after TRA
Strategy Level of Evidence
Use of smaller sheaths,
eg, 5F vs 6FA
Use of sheathless
guidesC
Patent hemostasis A
Anticoagulation B
Strategies for Reducing Radial Artery Thrombosis
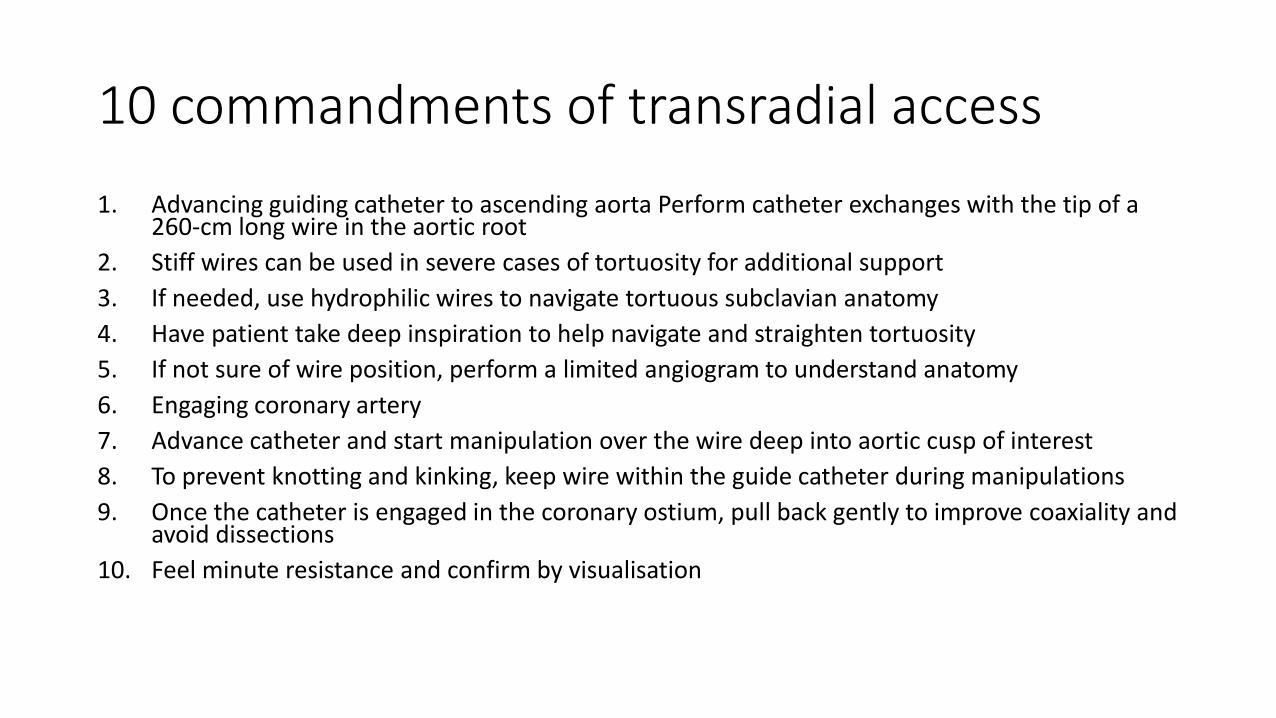
10 commandments of transradial access
1. Advancing guiding catheter to ascending aorta Perform catheter exchanges with the tip of a 260-cm long wire in the aortic root
2. Stiff wires can be used in severe cases of tortuosity for additional support
3. If needed, use hydrophilic wires to navigate tortuous subclavian anatomy
4. Have patient take deep inspiration to help navigate and straighten tortuosity
5. If not sure of wire position, perform a limited angiogram to understand anatomy
6. Engaging coronary artery
7. Advance catheter and start manipulation over the wire deep into aortic cusp of interest
8. To prevent knotting and kinking, keep wire within the guide catheter during manipulations
9. Once the catheter is engaged in the coronary ostium, pull back gently to improve coaxiality and avoid dissections
10. Feel minute resistance and confirm by visualisation
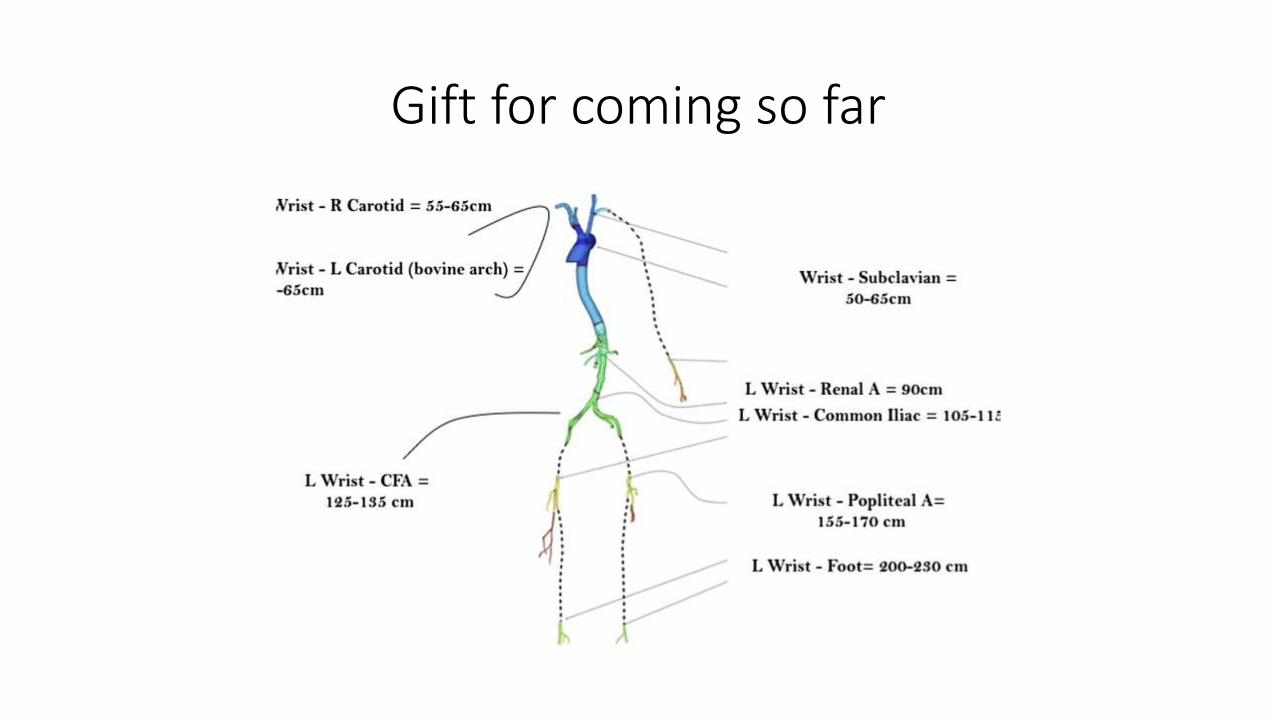
Gift for coming so far

Your health is my health
• Eat healthy
• Drink water in place of soft drink
• Walk more
• No to sugar reach drink



![Transradial Approach [LEft vs right] aNd procedural Times during percutaneous coronary procedures: TALENT study ALESSANDRO SCIAHBASI, MD UO Cardiologia,](https://img.pdfslide.us/doc/110x75/5697bff01a28abf838cba5c8/transradial-approach-left-vs-right-and-procedural-times-during-percutaneous.jpg)