Embed Size (px)
Citation preview

THYROID CANCERS
KANISHK DEEP SHARMAROLL NO. 50

CLASSIFICATION OF THYROID CANCERS
FOLLICULAR
DIFFERENTIATED
PAPILLARY
FOLLICULAR
MIXED
UNDIFFERENTIATED ANAPLASTIC
PARAFOLLICULAR MEDULLARY
NON-THYROID CELL ORIGIN
MALIGNANT LYMPHOMA
SARCOMA
METASTATIC CARCINOMA


UNDIFFERENTIATED

ANAPLASTIC CARCINOMA OF THYROID
10-15% of malignant tumors of thyroid

AETIOPATHOGENESIS
• Mostly Elderly Women• May develop from nodular goitre or pre-existing well
differentiated carcinoma• MACROSCOPICALLY– not encapsulated, can extend even to adjacent structures

• MICROSCOPICALLY– variable from spindle shaped, small cells to
multinucleate giant cells– Characteristic mitotic areas seen
• EARLY FEATURE– Local infiltration
• SPREAD BY– Lymphatics– Blood stream

CLINICAL FEATURES
• Thyroid gland often fixed• Poor movement on swallowing• Consistency hard to very firm• Berry’s sign positive• At time of diagnosis invasion to trachea, oesophagus
or adjacent structures of neck present• Tracheal, oesophageal obstruction• Regional lymph nodes frequently enlarged• Metastasis to bones & lungs common

STAGING
• All anaplastic thyroid cancers are considered stage IV


MANAGEMENT
• Diagnosis is by fine needle aspiration biopsy

• If confined to thyroid(minority of patients)– Complete resection of thyroid– Strap muscles resection
• ADVANCED STAGES– Tracheal obstruction
• Urgent tracheal decompression• Tissue obtained for histology by isthmusectomy• Tracheostomy avoided
• External Radiotherapy in all cases– Provides period for palliation

PROGNOSIS
• Maximum survival of 6 months• Average survival of 3 months

FOLLICULAR
DIFFERENTIATED
PAPILLARY
FOLLICULAR
MIXED
UNDIFFERENTIATED ANAPLASTIC
PARAFOLLICULAR MEDULLARY
NON-THYROID CELL ORIGIN
MALIGNANT LYMPHOMA
SARCOMA
METASTATIC CARCINOMA

• A solid mass of cell : ‘medullary’• Tumour of parafollicular C-cells• Secrete calcitonin– 32 amino acid polypeptide– Lowers serum calcium levels

ETIOPATHOGENESIS
• C-cells derived from neural crest cells(part of Amine Precursor Uptake Decarboxylase cells)

• C-cells concentrated superolaterally in thyroid lobes
• C-cell hyperplasia considered precursor of medullary carcinoma

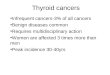
U/S medullary carcinoma with calcifications

• Characteristic amyloid stroma present


• High levels of serum calcitonin & carcinoembryonic antigen produced
• Diarrhea present– 30% cases– Presence of 5-hydroxytryptamine/ prostaglandin
produced by tumour cells– Increased motility & impaired absorption of water
& electrolyte

1. Familial (10-20% cases) non MEN2. MEN IIA (Sipple Syndrome)3. MEN IIB (Wagenmann–Froboese syndrome)

MEN IIA
• Affects children & young adults• Variation in RET proto-oncogene• Thyroid Medullary carcinoma with adrenal
pheochromocytoma & hyperparathyroidism• pheochromocytoma– Adrenal medullary cells part of APUD cells
• Due to low serum calcium levels parathyroid stimulated causing hyperplasia

MEN IIB
• Thyroid medullary carcinoma with – Prominent mucosal neuroma(involve lips, tongue
& inner aspects of eyelids)– Marfinoid habitus(long bones disproportionally
elongated)

CLINICAL FEATURES
• Neck mass• Pain referred to ear or jaw• Local invasion– dysphonia,– Dyspnea– Dysphagia

• cervical lymphadenopathy(50-60%)– Central Neck(level VI)– Superior mediastinum(level VII)
• Blood born metastasis common– Liver– Bone (characteristically osteoblastic)– Lung
• Diarrhea• May present with kidney stone due to hyperparathyroidism• Symptoms of pheochromocytoma

DIAGNOSIS AND SPECIAL INVESTIGATIONS
• Serum calcitonin levels by radioimmunoassay• Calcitonin levels
– In basal state– After stimulation test by inj. Pentagastrin i.v. bolus (0.5 mcg/Kg)– Successful in detecting early MEN cases without clinical signs or radiological evidence
• Not TSH dependent therefore doesn’t take up radioactive iodine• In Familial cases genetic screening
– RET gene mutation– Supplemented by serum calcitonin estimation
• Dx of pheochromocytoma– 24hr urinary catecholamine, metanephrine & VMA levels confirms diagnosis
• Hyperparathyroidism detected on serial measurements of blood Ca levels• Even small tumour confined to thyroid may spread by time of dx• Progression may have indolent course and long survival even without cure



TREATMENT• Total thyroidectomy due to multi-centricity with
prophylactic/therapeutic resection of central & B/L cervical lymph nodes
• Fall of calcitonin levels after resection & rise with recurrence, therefore, valuable tumor marker
• Prophylactic surgery recommended for infants(1yr) with genetic trait of MEN

• All family members of patients should be evaluated for serum calcitonin, If high then prophylactic total thyroidectomy
• Chemotherapy with adriamycin has lead to remission

• If hyperthyroidism present– Subtotal parathyroidectomy(90% gland excision)
• All cases, before thyroidectomy, pheochromocytoma must be excluded
• Pheochromocytoma– B/L total adrenalectomy due to multicentricity & B/L nature of
lesion– Preoperatively
• Phenoxybenzamine(50-200mg/day)• Propranolol(40mg/day)
– Postoperatively• Long term glucocorticoid & mineralocorticoid therapy

PROGNOSIS
• Varies with stage of diagnosis• Nodal involvement virtually eliminates
prospects of cure• 5yr survival without lymph node metastasis is
70%