Embed Size (px)
Citation preview
THROMBO-PROPHYLAXISIN
OBSTETRICS
SUJOY DASGUPTAMBBS (Gold Medalist, Hons),
MS (OBGY- Gold Medalist), DNB (OBGY)
Senior Resident, Deptt of Gynaecological Oncology, Chittaranjan National cancer Institute (CNCI), Kolkata

Venous Thromboembolism (VTE)• Incidence- 2.3 per 1000 pregnancy
• Risk increases 4-6 fold in pregnancy
• Risk increases further in puerperium (especially the 1st week)
• Overall case fatality rate- 3.5%
• The mortality rate of PE is 11% within an hour of presentation and a further 30% among survivors if not recognized.
• Often no time for diagnosis and treatment
• Globally- 3% of maternal deaths (WHO, 2014)
Prevention- THROMBO-PROPHYLAXIS
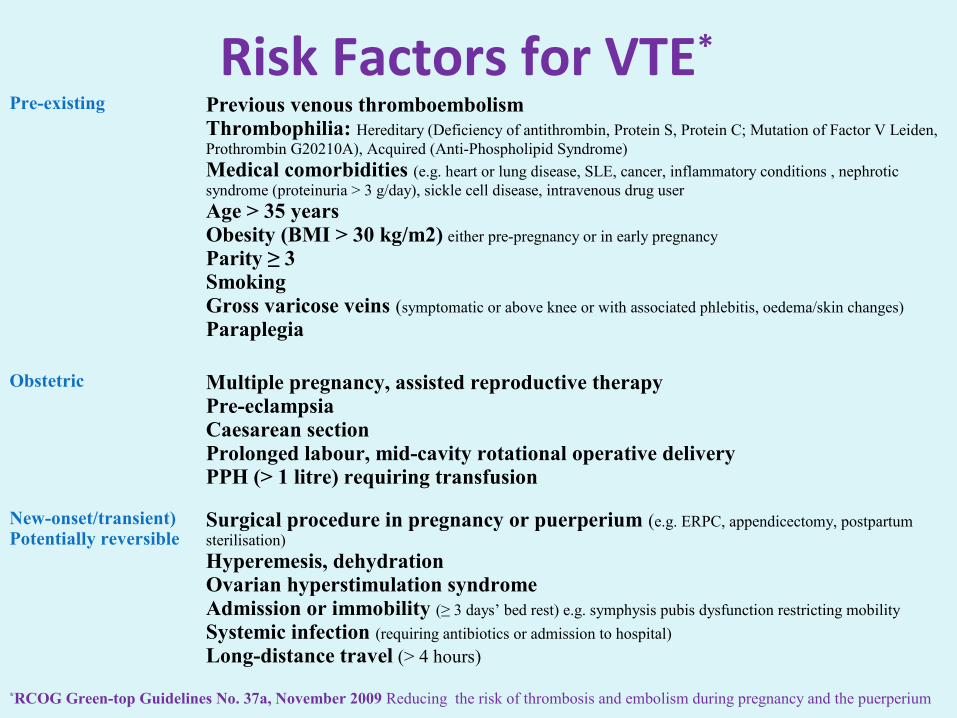
Risk Factors for VTE*
Pre-existing Previous venous thromboembolismThrombophilia: Hereditary (Deficiency of antithrombin, Protein S, Protein C; Mutation of Factor V Leiden, Prothrombin G20210A), Acquired (Anti-Phospholipid Syndrome)
Medical comorbidities (e.g. heart or lung disease, SLE, cancer, inflammatory conditions , nephrotic syndrome (proteinuria > 3 g/day), sickle cell disease, intravenous drug user
Age > 35 yearsObesity (BMI > 30 kg/m2) either pre-pregnancy or in early pregnancy
Parity ≥ 3SmokingGross varicose veins (symptomatic or above knee or with associated phlebitis, oedema/skin changes)
Paraplegia
Obstetric Multiple pregnancy, assisted reproductive therapyPre-eclampsiaCaesarean sectionProlonged labour, mid-cavity rotational operative deliveryPPH (> 1 litre) requiring transfusion
New-onset/transient)Potentially reversible
Surgical procedure in pregnancy or puerperium (e.g. ERPC, appendicectomy, postpartum sterilisation)
Hyperemesis, dehydrationOvarian hyperstimulation syndromeAdmission or immobility (≥ 3 days’ bed rest) e.g. symphysis pubis dysfunction restricting mobility
Systemic infection (requiring antibiotics or admission to hospital)
Long-distance travel (> 4 hours)
*RCOG Green-top Guidelines No. 37a, November 2009 Reducing the risk of thrombosis and embolism during pregnancy and the puerperium
When to Assess
• Preconceptional Care
• First Antenatal visit
• Intrapartum period
• Immediate postpartum
• If admitted to hospital for any reason
• If develops intercurrent problems (e.g., infection)
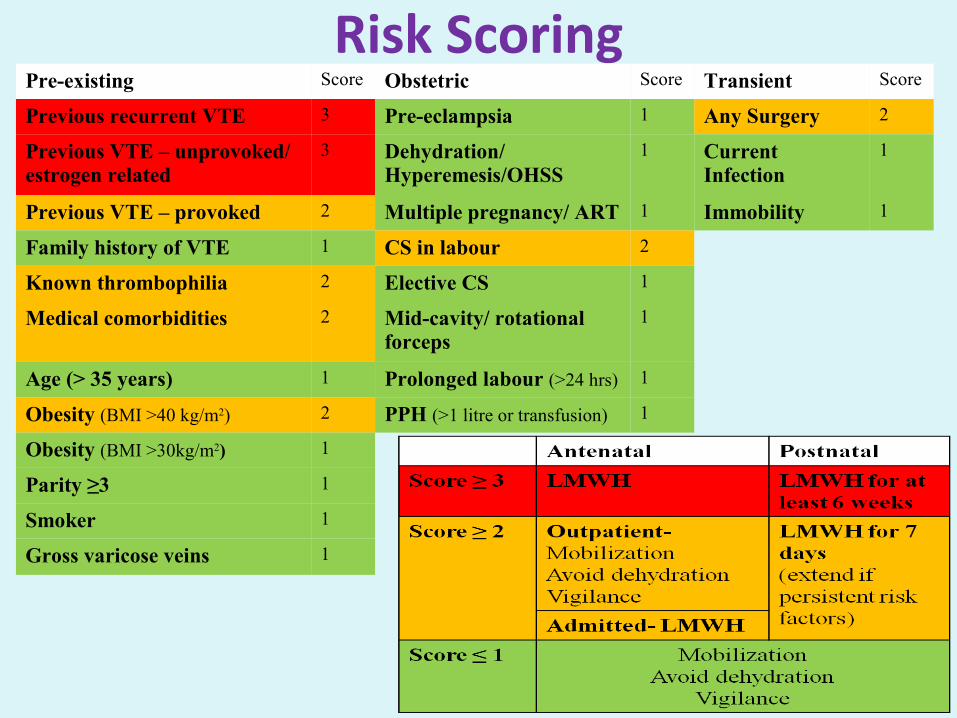
Risk ScoringPre-existing Score Obstetric Score Transient Score
Previous recurrent VTE 3 Pre-eclampsia 1 Any Surgery 2
Previous VTE – unprovoked/ estrogen related
3 Dehydration/ Hyperemesis/OHSS
1 Current Infection
1
Previous VTE – provoked 2 Multiple pregnancy/ ART 1 Immobility 1
Family history of VTE 1 CS in labour 2
Known thrombophilia 2 Elective CS 1
Medical comorbidities 2 Mid-cavity/ rotational forceps
1
Age (> 35 years) 1 Prolonged labour (>24 hrs) 1
Obesity (BMI >40 kg/m2) 2 PPH (>1 litre or transfusion) 1
Obesity (BMI >30kg/m2) 1
Parity ≥3 1
Smoker 1
Gross varicose veins 1
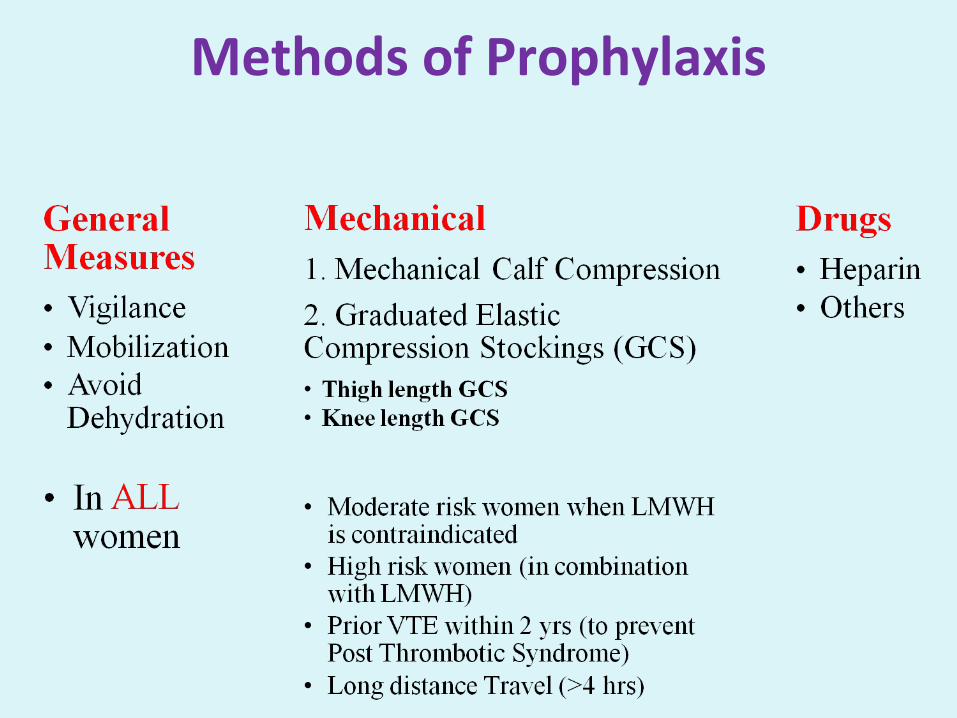
Methods of Prophylaxis
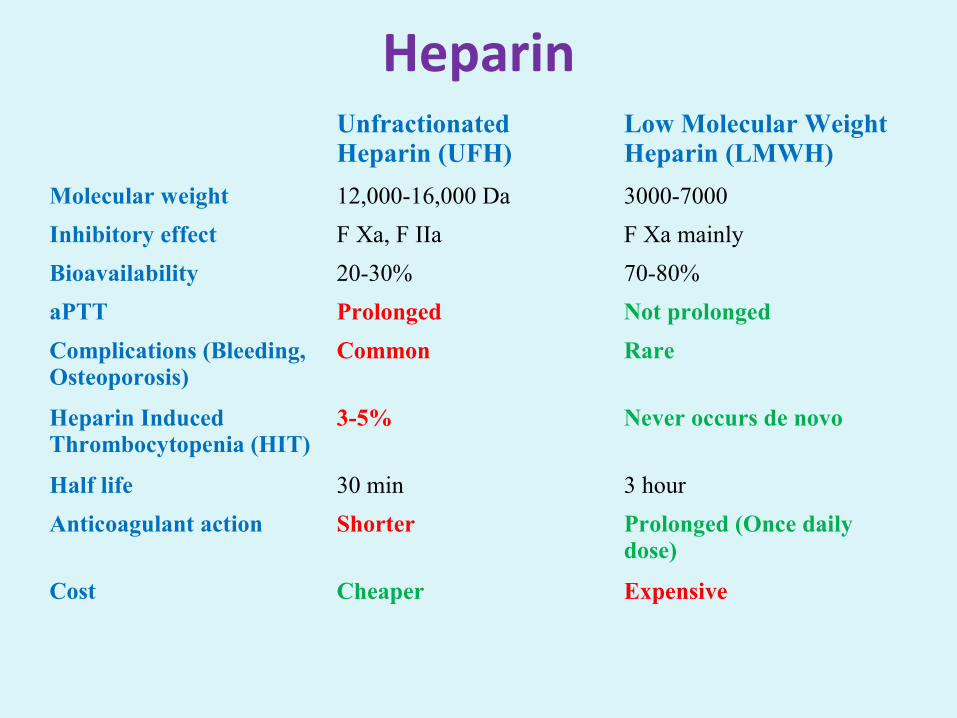
HeparinUnfractionated Heparin (UFH)
Low Molecular Weight Heparin (LMWH)
Molecular weight 12,000-16,000 Da 3000-7000
Inhibitory effect F Xa, F IIa F Xa mainly
Bioavailability 20-30% 70-80%
aPTT Prolonged Not prolonged
Complications (Bleeding, Osteoporosis)
Common Rare
Heparin Induced Thrombocytopenia (HIT)
3-5% Never occurs de novo
Half life 30 min 3 hour
Anticoagulant action Shorter Prolonged (Once daily dose)
Cost Cheaper Expensive
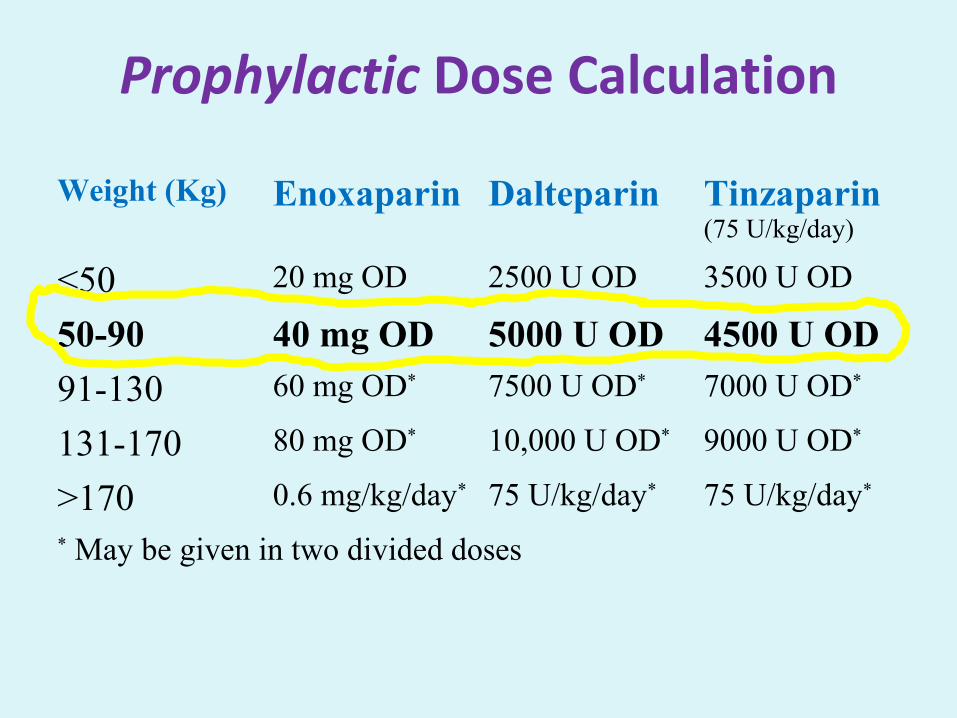
Prophylactic Dose Calculation
Weight (Kg) Enoxaparin Dalteparin Tinzaparin(75 U/kg/day)
<50 20 mg OD 2500 U OD 3500 U OD
50-90 40 mg OD 5000 U OD 4500 U OD
91-130 60 mg OD* 7500 U OD* 7000 U OD*
131-170 80 mg OD* 10,000 U OD* 9000 U OD*
>170 0.6 mg/kg/day* 75 U/kg/day* 75 U/kg/day*
* May be given in two divided doses
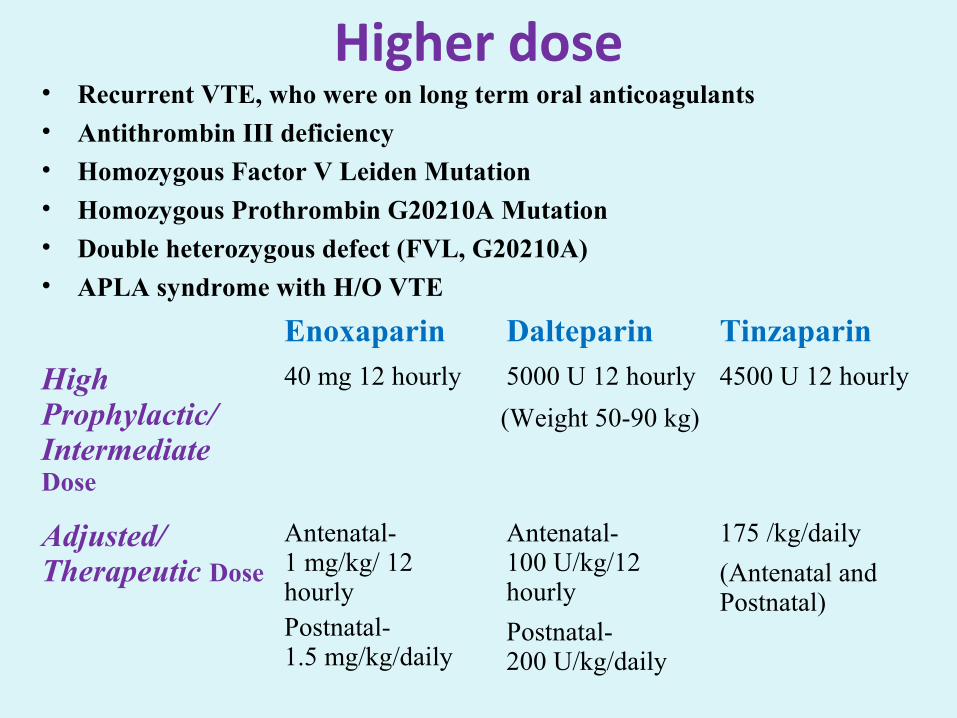
Higher dose• Recurrent VTE, who were on long term oral anticoagulants
• Antithrombin III deficiency
• Homozygous Factor V Leiden Mutation
• Homozygous Prothrombin G20210A Mutation
• Double heterozygous defect (FVL, G20210A)
• APLA syndrome with H/O VTE
Enoxaparin Dalteparin Tinzaparin
High Prophylactic/ Intermediate Dose
40 mg 12 hourly 5000 U 12 hourly 4500 U 12 hourly
(Weight 50-90 kg)
Adjusted/ Therapeutic Dose
Antenatal-1 mg/kg/ 12 hourlyPostnatal- 1.5 mg/kg/daily
Antenatal-100 U/kg/12 hourly
Postnatal-200 U/kg/daily
175 /kg/daily
(Antenatal and Postnatal)
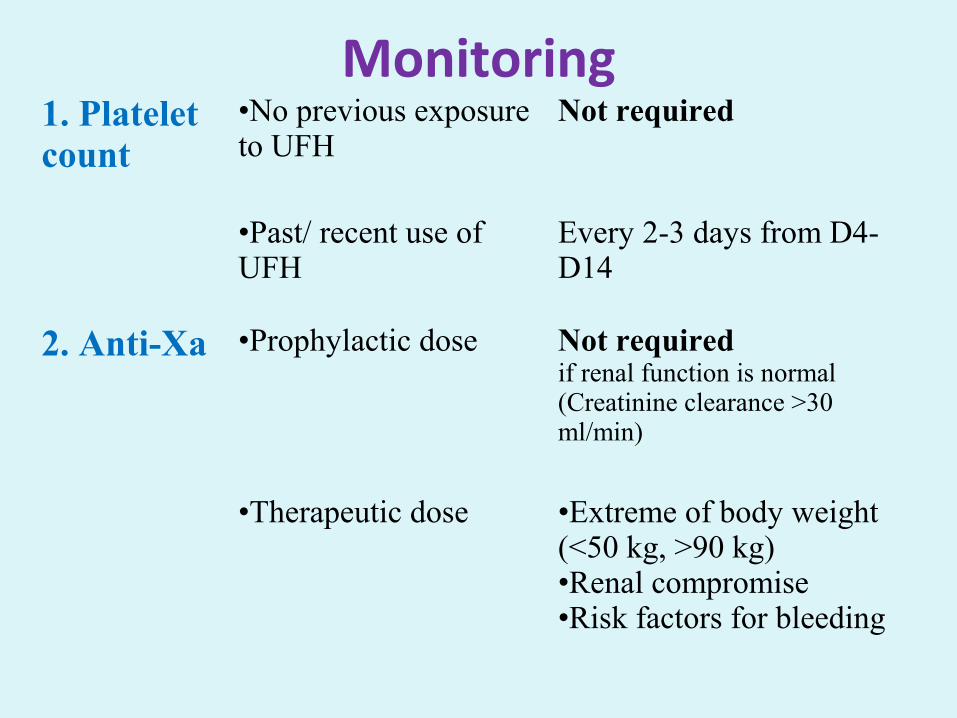
Monitoring1. Platelet count
•No previous exposure to UFH
Not required
•Past/ recent use of UFH
Every 2-3 days from D4- D14
2. Anti-Xa •Prophylactic dose Not required if renal function is normal (Creatinine clearance >30 ml/min)
•Therapeutic dose •Extreme of body weight (<50 kg, >90 kg)•Renal compromise•Risk factors for bleeding
Delivery and anaesthesia
• To stop further injection if she feels labour pain/ vaginal bleeding
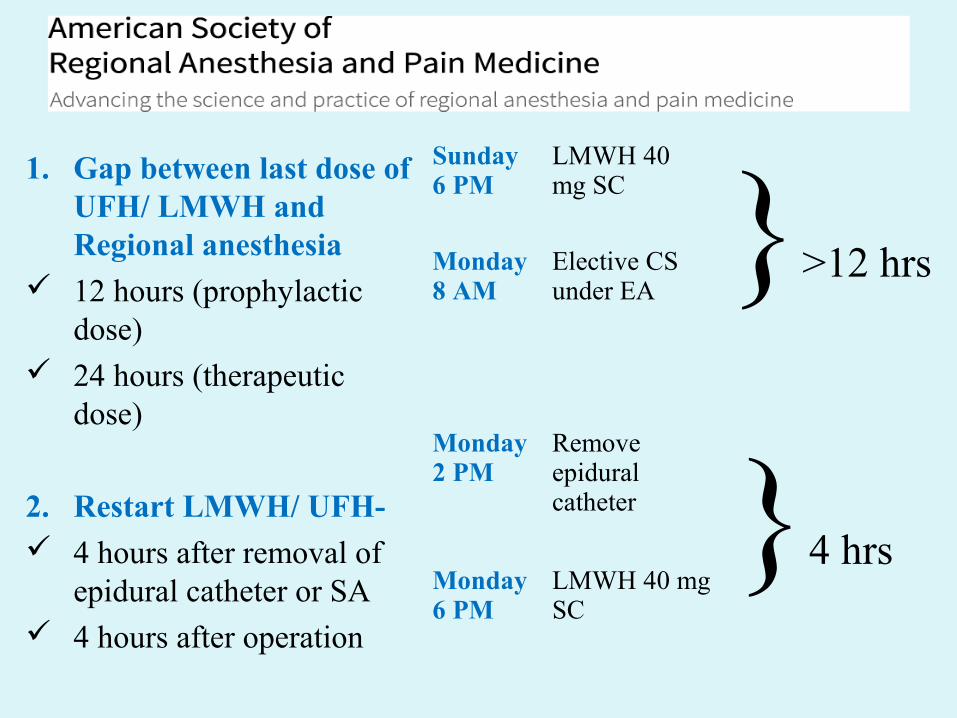
1. Gap between last dose of UFH/ LMWH and Regional anesthesia
12 hours (prophylactic dose)
24 hours (therapeutic dose)
2. Restart LMWH/ UFH- 4 hours after removal of
epidural catheter or SA 4 hours after operation
Sunday 6 PM
LMWH 40 mg SC }>12 hrs Monday
8 AMElective CS under EA
Monday 2 PM
Remove epidural catheter }4 hrs
Monday 6 PM
LMWH 40 mg SC
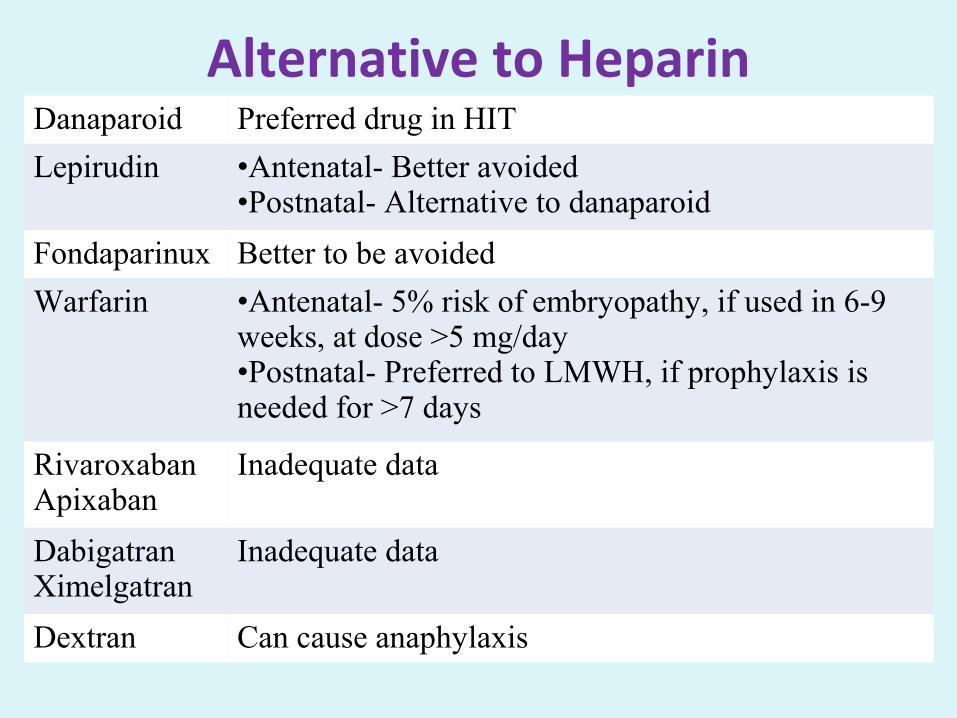
Alternative to HeparinDanaparoid Preferred drug in HIT
Lepirudin •Antenatal- Better avoided•Postnatal- Alternative to danaparoid
Fondaparinux Better to be avoided
Warfarin •Antenatal- 5% risk of embryopathy, if used in 6-9 weeks, at dose >5 mg/day•Postnatal- Preferred to LMWH, if prophylaxis is needed for >7 days
RivaroxabanApixaban
Inadequate data
DabigatranXimelgatran
Inadequate data
Dextran Can cause anaphylaxis
Special Cases
Thrombophilia and Thrombosis
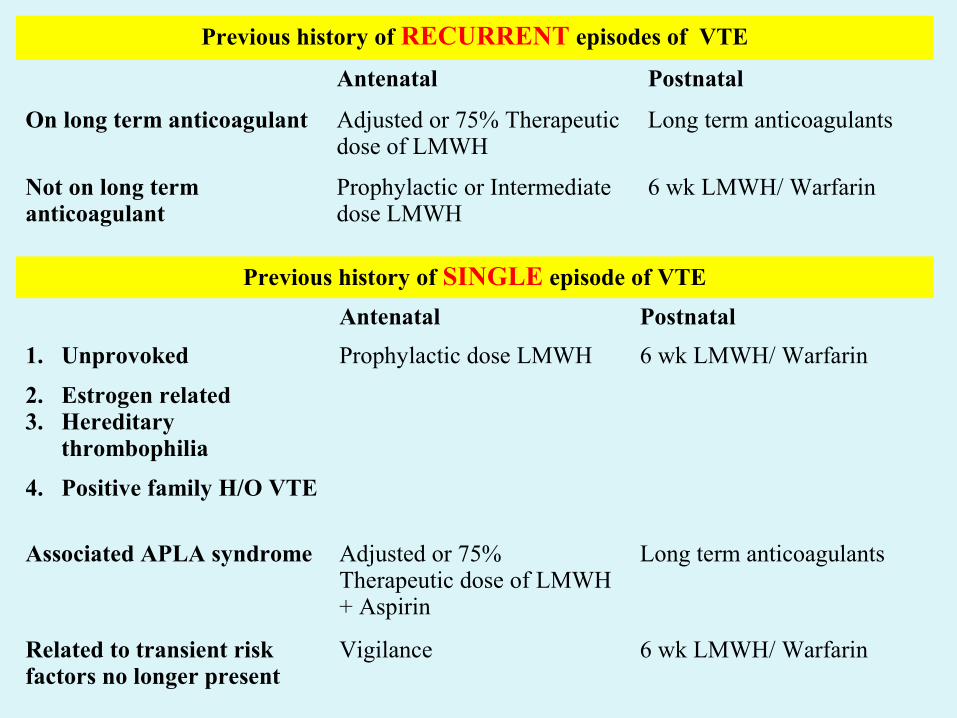
Previous history of RECURRENT episodes of VTE
Antenatal Postnatal
On long term anticoagulant Adjusted or 75% Therapeutic dose of LMWH
Long term anticoagulants
Not on long term anticoagulant
Prophylactic or Intermediate dose LMWH
6 wk LMWH/ Warfarin
Previous history of SINGLE episode of VTE
Antenatal Postnatal
1. Unprovoked
2. Estrogen related3. Hereditary
thrombophilia
4. Positive family H/O VTE
Prophylactic dose LMWH 6 wk LMWH/ Warfarin
Associated APLA syndrome Adjusted or 75% Therapeutic dose of LMWH + Aspirin
Long term anticoagulants
Related to transient risk factors no longer present
Vigilance 6 wk LMWH/ Warfarin
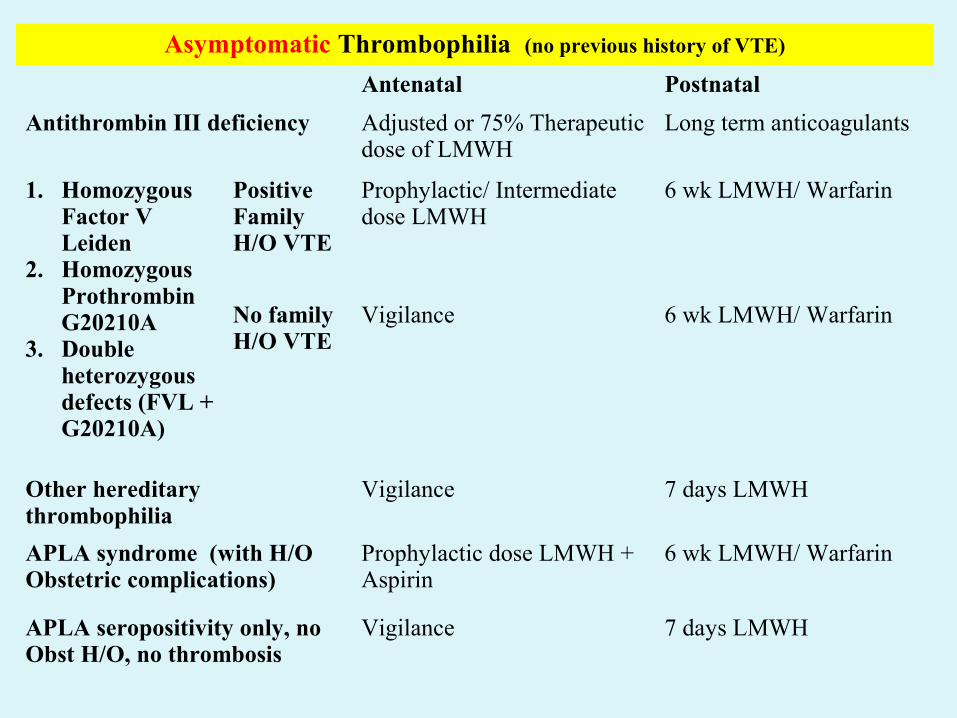
Asymptomatic Thrombophilia (no previous history of VTE)
Antenatal Postnatal
Antithrombin III deficiency Adjusted or 75% Therapeutic dose of LMWH
Long term anticoagulants
1. Homozygous Factor V Leiden
2. Homozygous Prothrombin G20210A
3. Double heterozygous defects (FVL + G20210A)
Positive Family H/O VTE
Prophylactic/ Intermediate dose LMWH
6 wk LMWH/ Warfarin
No family H/O VTE
Vigilance 6 wk LMWH/ Warfarin
Other hereditary thrombophilia
Vigilance 7 days LMWH
APLA syndrome (with H/O Obstetric complications)
Prophylactic dose LMWH + Aspirin
6 wk LMWH/ Warfarin
APLA seropositivity only, no Obst H/O, no thrombosis
Vigilance 7 days LMWH
Artificial Mechanical Heart Valves
• Thrombosis vs fetal risk
• Individualization and informed risk consent

• 1st trimester:1. If on low dose warfarin (<5 mg/day)- Consider
continuation of warfarin (ESC, 2011)
2. High risk of VTE (Older generation in mitral position, past H/O VTE)- Continue Warfarin (ACCP, 2012)
3. In other cases- Consider replacement of warfarin by LMWH or UFH (ACCP, 2012)
• 2nd and 3rd trimester:1. Warfarin and replace by UFH close to term (ESC,
2011)
2. Any one of Warfarin, LMWH or UFH (ACCP, 2012)
• After delivery: Resume anticoagulant 4-6 hour after delivery
(ACCP 2012, ESC 2011)
INDIAN SCENARIO
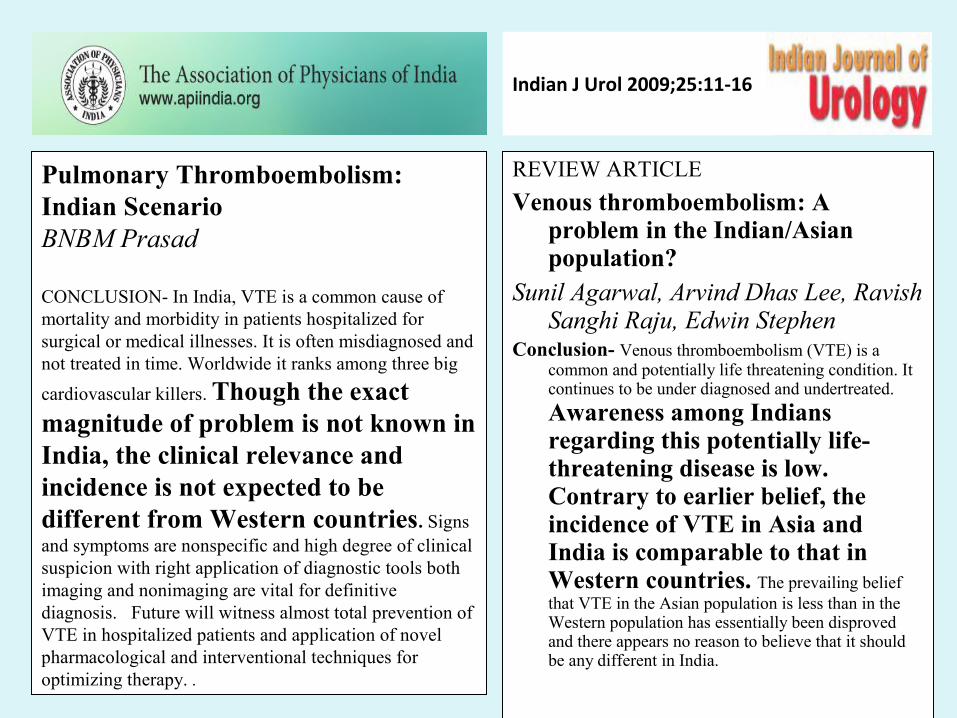
Indian J Urol 2009;25:11-16
REVIEW ARTICLE
Venous thromboembolism: A problem in the Indian/Asian population?
Sunil Agarwal, Arvind Dhas Lee, Ravish Sanghi Raju, Edwin Stephen
Conclusion- Venous thromboembolism (VTE) is a common and potentially life threatening condition. It continues to be under diagnosed and undertreated.
Awareness among Indians regarding this potentially life-threatening disease is low. Contrary to earlier belief, the incidence of VTE in Asia and India is comparable to that in Western countries. The prevailing belief that VTE in the Asian population is less than in the Western population has essentially been disproved and there appears no reason to believe that it should be any different in India.
Pulmonary Thromboembolism: Indian Scenario BNBM Prasad
CONCLUSION- In India, VTE is a common cause of mortality and morbidity in patients hospitalized for surgical or medical illnesses. It is often misdiagnosed and not treated in time. Worldwide it ranks among three big
cardiovascular killers. Though the exact magnitude of problem is not known in India, the clinical relevance and incidence is not expected to be different from Western countries. Signs and symptoms are nonspecific and high degree of clinical suspicion with right application of diagnostic tools both imaging and nonimaging are vital for definitive diagnosis. pFuture will witness almost total prevention of VTE in hospitalized patients and application of novel pharmacological and interventional techniques for optimizing therapy. .
International Journal of Biological & Medical Research
Journal homepage: www.biomedscidirect.com
Original Article
Maternal Mortality at a Tertiary Care Teaching Hospital of Rural India: A Retrospective Study
Vidyadhar B. Bangal, Purushottam A. Giri, Ruchika Garg
Pulmonary embolism is the third most common direct cause of maternal mortality (10.59% deaths) after haemorrhage and eclampsia
Original ArticleDeep venous thrombosis in the
antenatal period in a large cohort of pregnancies from western India
Sonal Vora, Kaniaksha Ghosh, Shrimati Shettv, Vinita Salvi, and Purnima Santoskar
Conclusion- We conclude that the prevalence of DVT in India is more or less similar to other reports published (1 in 1000) and both acquired and heritable thrombophilia show strong association with DVT associated with pregnancy.
Thromb J. 2007; 5: 9J Obstet Gynaecol India.
Dec 2013; 63(6): 373–377
Original ArticleSafety and Efficacy of Low
Molecular Weight Heparin Therapy During Pregnancy: Three Year Experience at a Tertiary Care Center
Nilanchali Singh, Priva Varshnev, Reva Tripathi, Y. M. Mala, and Shakun Tyagi
Conclusion- Low molecular weight heparin can be used in pregnancy for various indications as an alternative to unfractionated heparin or warfarin as it is efficacious and safe.
Conclusion• Pregnancy itself is a
thrombogenic condition• Every woman should be
assessed for risk factors• Decision for
thromboprophylaxis should be individualized
• LMWH is the drug of choice• Threshold for recommending
thromboprophylaxis should be lower because the risk is higher and the duration is shorter

THANK YOU