Embed Size (px)
Citation preview


The ocular presentation of systemic diseases
Data collected by : Ruwida Mohammed Saeed

The eyes are actually a part of the human body sharing functions with it , and affected by factors leading to its deterioration …
It can be your mirror if you knew how to use

Here are some of the main complaints that are commonly faced

Eye presentation
Amaurosis Fugax
Uveitis
Cataracts
Abnormal EyeMovements
Pupillary Abnormalities
Retinal vessel disease
Corneal effects
Eyelids

Amaurosis Fugax = is a painless transient monocular
visual loss

Amaurosis Fugax
Embolic
Vasospastic/
Haemodynamic
Neurologic
Ocular
Idiopathic

Amaurosis Fugax
Embolic
Vasospastic/
Hemodynamic
Neurologic
Ocular
Idiopathic
Optic neuritis (MS)Migraine

Optic neuritis • Rapidly developing impairment of vision in 1
eye or, less commonly, both eyes
• Dyschromatopsia ,may be more prominent than the decreased vision
• Retro-orbital or ocular pain exacerbated by eye movement
• Uhthoff phenomenon, in which vision loss is exacerbated by heat or exercise
• Pulfrich phenomenon, in which objects moving in a straight line appear to have a curved trajectory: Presumably caused by asymmetrical conduction between the optic nerves

Multiple sclerosis is the most common manifestation (usually unilateral, but may be bilateral) and the presenting feature in about 25% of MS patients
About 60% of patients in the 20-40 years age group who present with ON will subsequently develop evidence of systemic demyelinisation !

Amaurosis Fugax
Embolic
Vasospastic/
Haemodynamic
Neurologic
Ocular
Idiopathic
Embolic
TIAcardiac/carotid/

Amaurosis Fugax
Embolic
Vasospastic/
Hemodynamic
Neurologic
Ocular
Idiopathic
Temporal Arteritis

Temporal arteritis • is a systemic inflammatory vasculitis of
unknown etiology that affects medium- and large-sized arteries.
The clinical criteria is :1. New headache (localized temporal)
2. Abnormalities of the temporal arteries (tenderness or decreased temporal artery pulse)
3. (ESR) of 50 mm/h
4. Positive results of a temporal artery biopsy
5. visual impairment may occur in as many as 60% of patients

• The most common cause of vision loss is anterior ischemic optic neuropathy (AION). This results from ischemia of the optic nerve head
• optic neuropathy, central retinal artery occlusion, branch retinal artery occlusion
• diplopia, ptosis, nystagmus, internuclear ophthalmoplegia (INO), and pupillary abnormalities. Branch retinal vein occlusion in a patient
with giant cell arteritis

Eyelids presentation
Dermatochalsis Proptosis Ptosis

Proptosis • Infectious
• Orbital cellulitis . Mucormycosis , Concurrent sinus disease
• Inflammatory• Thyroidopathy
• Vasculitis• Wegener granulomatosis
• Churg-Strauss syndrome
• Neoplastic• Lymphoma
• Leukemia
• Meningioma
• Glioma
• Ossifying fibroma
• Metastatic (breast in women, lung and prostate in men, gastrointestinal, kidney

Dermatochalsis • Chronic dermatitis , as of the chronic
inflammation leads to recurrent edema and redundancy of the eyelid skin.
• Thyroid eye disease frequently associated with dermatochalsis and steatoblepharon ,infiltration of the orbital fat and extraocular muscles with immunoglobulin complexes.
• Chronic renal insufficiency can be associated with periorbital edema. When chronic edema can result in stretching of the eyelid skin and redundancy of the eyelid

1. Soft tissue involvement• Periorbital and lid swelling• Conjunctival hyperaemia• Chemosis• Superior limbic keratoconjunctivitis
2. Eyelid retraction3. Proptosis4. Optic neuropathy5. Restrictive myopathy
THYROID EYE DISEASE

Soft tissue involvementPeriorbital and lid swelling
Chemosis
Conjunctival hyperaemia
Superior limbic keratoconjunctivitis

Signs of eyelid retraction Occurs in about 50%
Bilateral lid retraction Bilateral proptosis Lid lag in downgaze

Proptosis
• Occurs in about 50% • Uninfluenced by treatment of hyperthyroidism
Axial and permanent in about 70% May be associated with choroidal folds

• Occurs in about 40% • Due to fibrotic contracture
Restrictive myopathy
Elevation defect - most common Abduction defect - less common
Depression defect - uncommon Adduction defect - rare

Ptosis • Any condition causing the upper eyelid to swell may cause ptosis
• Reduced Sympathetic Activity (Horner’s syndrome )
• Partial Ptosis , Miosis , anhydrosis
Brainstem stroke or tumor , 33% of patients with brainstem lesions demonstrated Horner syndrome
Tumors (eg, Pancoast) or infection of the lung apex
Dissecting carotid aneurysm
Demyelinating disease (eg, multiple sclerosis)
Central venous catheterization , Chest tubes
Lymphadenopathy (eg, Hodgkin disease, leukemia, tuberculosis, or mediastinal tumors)
Lesions of the middle ear (eg, acute otitis media

• Muscular , nerve , neuromuscular junction : myotonic dystrophy , polymyositis, dermatomyositis , myasthenia, Lambert–Eaton syndrome
• Oculomotor nerve palsy giant cell arteritis, Infection, cavernous
sinus thrombosis ,
diabetes mellitus
Miller Fisher syndrome, associated with antibodies to ganglioside GQ1b In Miller Fisher syndrome, extraocular muscle involvement is the rule but there are reports of isolated ptosis.


Pupillary Abnormalities
• Horner's syndrome
• Third nerve palsy
• Holmes-Adie syndrome
• Argyl Robertson
• Pontine stroke

Third nerve palsy
• Infectious meningitis - Bacterial, fungal/parasitic, viral
• Carcinomatous/lymphomatous/leukemic infiltration, granulomatous inflammation (sarcoidosis, lymphomatoid granulomatosis, Wegener granulomatosis)
• Pituitary adenoma, meningioma, craniopharyngioma, metastatic carcinoma


• is a neurological disorder characterized by dilated pupil that reacts slowly to light but shows a more definite response to accommodation
• the classic signs of Argyll Robertson pupil, are rigidity to light and contraction to accommodation
• it has been seen with herpes zoster, sarcoid, von Beonomo's encephalitis, diabetes, Lyme disease, Wernicke's encephalopathy.
• Tertiary syphilis
Holmes-Adie syndrome
Argyl robertson pupil


The corneal changes and the systemic disease • Ulceration• Collagen vascular disease:
rheumatoid arthritis, lupus erythematosus, polyarteritis, Sjögren's disease, Wegener's granulomatosis
• Sjögren's disease (keratitis sicca, marginal melting)
• Alterations in contour / keratoconus• Atopic diseases
• Down's syndrome
• Marfan's syndrome
• DEPOSITS• Gout , myeloma
• Wilson's disease (dark copper pigment in Descemet's membrane)


The lens changes are presented as cataracts


CATARACT
MetabolicOther Systemic
Diseases Drug Induced
DM
G6PDMuscular
Dystrophy
NF 2
DermatitisSteroids

Two types of cataracts result from diabetes
Earlier onset age-related • diabetic cataract ,more common
type is which occurs in type I or II diabetics.
• It is very similar to other age-related cataracts, and may present as a cortical, posterior subcapsular
snowflake cataract• Rare, bilateral, occurs rapidly,
and related to very high, uncontrolled DM in young type II diabetics


Uveitis
Systemic Dis&
Syndromes
Infections Infestations
TB
Candida
Herpes Zoster

UveitisSystemic Dis
& Syndromes
Sarcoid
BehcetsReiter's
Ankylosing Spondylitis
Crohn'sDis UC JCA

Uveitis
Systemic Dis& Syndromes
Sarcoid
BehcetsReiter's
Ankylosing Spondylitis
Crohn'sDis
Ulcerative colitis
JCA

Ulcerative colitis is characterized severe diarrhea and cramps , Fever ,Leukocytosis , Abdominal distention
UC is associated with various extracolonic manifestations, as follows:
• Uveitis
• Pyoderma gangrenosum
• Pleuritis
• Erythema nodosum
• Ankylosing spondylitis
• Spondyloarthropathies

UveitisSystemic Dis
& Syndromes
Sarcoid
BehcetsReiter's
Ankylosing Spondylitis
Crohn'sDis UC JCA


Systemic Dis& Syndromes
Sarcoid
BehcetsReiter's
Ankylosing Spondylitis
Crohn'sDisease
UCRheumatoid
arthritis

Uveitis
Systemic Dis& Syndromes
Sarcoid
Behcets
Reiter's
Ankylosing Spondylitis
Crohn'sDis UC JCA
Sacroilitis
33% of pts of AS present with acute anterior uveitis …

Systemic Dis& Syndromes
Sarcoid
Behcets
Reiter's
Ankylosing Spondylitis
Crohn'sDis UC JCA
UrethritisArthritis

Systemic Dis& Syndromes
Sarcoid
BehcetsReiter's
Ankylosing Spondylitis
Crohn'sDis UC JCA

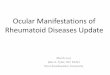
Ocular involvement in Behçet disease
• Ocular involvement is seen in about 70% of patients
• In most cases, the ocular symptoms follow the oral and genital ulcers by 3-4 years, although ocular disease is the initial manifestation in about 20% of cases.
• The classic finding of Behçet disease, iridocyclitis with hypopyon, is present in about one third of cases.
• Gonioscopy may reveal an occult hypopyon characterised by hypopyon that it may change position with head movement, and it may form and disappear rapidly without sequelae.
• Recurrent attacks may result in posterior synechiae, peripheral anterior synechiae, iris atrophy, and secondary glaucoma.
A 19-year-old boy presenting with vitreous haze, and retinal infiltrates due to Behçet’s disease.

• The classic fundus finding is retinal vasculitis
• retinal hemorrhages, yellow-white exudates deep in the retina, white focal retinal infiltrates, retinal edema, and optic disc edema with hyperemia.
• Retinal neovascularization, secondary to either retinal vein occlusion or chronic inflammation, may result in retinal or vitreous hemorrhage.
• Neovascular glaucoma
• Vitreous cellular infiltration almost always is present during the acute phase.
• Repeated episodes of posterior segment inflammation cause sheathing of retinal vessels, chorioretinal scars, and retinal and optic nerve atrophy.

Uveitis
Systemic Dis& Syndromes
Sarcoid
BehcetsReiter's
Ankylosing Spondylitis
Crohn'sDis UC JCA
Unknown Aetiology granuloma

SARCOIDOSISSystemic Involvement• Lung lesions – 95%
• Thoracic lymph nodes – 50%
• Skin lesions – 30%
• Eyes – 30%

SARCOIDOSISOcular Involvement• Conjunctival granuloma
• Lacrimal gland involvement/dry eye
• Acute or chronic uveitis
• KPs described as ‘mutton fat’ because they are large and greasy
• Chorioretinal granulonmas
• Vasculitis including occlusive causing:-
• Neovascularisation
• Infiltrate in vitreous (vitritis)
• Optic nerve head granuloma


The retina is affected by many diseases , but thecommonest are diabetes , hypertension ,

Capillary damage
Pericyte necrosis(capillaries and veins)
Endothelial damage
Capillary non-perfusion
Retinal ischaemia
Vasoactive factors
HyperperfusionAbnormal autoregulation
Hypertension
New vesselsGrowth factors
Hyperglycemia


Diabetic retinopathy • Diabetic retinopathy is the leading cause of new blindness in persons
aged 25-74 years in the United States . And classified as : Background diabetic retinopathyNonproliferative diabetic retinopathyproliferative diabetic retinopathyMaculopathy


BackgroundRetinopathy
Dot Haemorrhages
Hard Exudates
NORMAL eyesight
-present in almost all who have had type 1 diabetes for 20 years -present in nearly 80 percent of those with type 2 disease for 20 years
Micro-aneurysms


Pre-prolifRetionopathy
Cotton WoolSpots
Venous Irregularity
NORMAL EYESIGHT


Pre-prolifRetionopathy
REFER!
50% of patients progress to proliferative retinopathy within 1-2 years

ProliferativeRetinopathy
Neo-vascularisation
NVD
NVE
NORMALEYESIGHT,but threatened....


Maculopathy
Early and Diffuse
Severe andIschaemic
EYESIGHTAFFECTED


ANTERIOR SEGMENT COMPLICATIONS OF DIABETES
Recurrent, non-healing corneal epithelial defects
Neovascular glaucoma
Diabetes lowers the resistance of the patient to pyogenic infections and predisposes to recurrent styes

Transient Refractive Changes and diabetes
Accommodation Disorders.
Weakness of accommodation may result when the ciliary muscle becomes weakened by peripheral neuritis involving its nerve supply.
Subjective Visual Disturbances.
Amaurosis may occur in severe cases of diabetes. Disturbances of the visual cortex may lead to misty vision and to lashes of light which patients may experience after an overdose of insulin. .

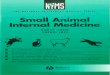
Hypertension
Grade I
Grade II
Grade III
Grade IV
Papill-oedema
HaemorrhagesCottonWoolSpots
A-V Nipping
SilverWiring

Abnormal eye movement Nystagmus
• Seesaw nystagmus• Rostral midbrain lesions - Parasellar
lesions (eg, pituitary tumors)

Downbeat nystagmus Lesions of the vestibulocerebellum and underlying medulla, including the following:
• Demyelination (eg, multiple sclerosis)
• Microvascular disease with vertebrobasilar insufficiency
• Brain stem encephalitis
• Tumors at the foramen magnum (eg, meningioma, cerebellar hemangioma)
• Nutritional (eg, Wernicke encephalopathy, parenteral feeding, magnesium deficiency)

Restricted eye movement 1. Cranial Nerve Disease (palsy/paresis, congenital/developmental anomaly,tumor,
vascular, inflammatory, trauma, immune, etc.)
2. Neuromuscular Junction (Myasthenia, etc)
3. Muscular Disease (congenital/developmental anomaly, tumor, vascular, inflammatory, trauma, immune, etc.)
4. Orbital Disease (pulley, congenital/developmental, tumor, vascular,inflammatory, trauma, immune, etc.)

Thank you