Embed Size (px)
DESCRIPTION
Geared towards advanced pain nurses for the hospital-based and evidence-based management of pain. Overview of physiology, pathophysiology, assessment and management.
Citation preview

THE INS AND OUTS OF PAIN
Kyle P. Edmonds, MDFellow, Scripps Health & The Institute for Palliative Medicine at San Diego
Hospice
Adapted from the Palliative Care International Curriculum Series
Editor, Frank R. Ferris, MD

OBJECTIVES
• Review the definitions, pathophysiology & classifications of pain.
• Perform a standardized assessment of pain and state why it is important for team communication.
• State how Cmax and half-life relate to opioid dosing.
• Describe the hallmark of addiction and the low likelihood of occurrence in pain management.

International Association for the Study of Pain ( IASP ):
“An unpleasant sensory and emotional experience
associated withactual or potential tissue damage.”
PAIN

Margo McCaffery:
“Pain is whatever the person says it is…”
PAIN

TOTAL PAINCICELY SAUNDERS 1964
Patient
with Pain
Physical
Emotional
Existential
Social

MECHANISM OF PAIN- DESCARTES


NOCICEPTOR
• Nerve cell
• Activation• Thermal • Chemical• Mechanical
• Transmits signal

NOCICEPTION
• Activation of receptors
• Transmitting
• Processing
• Leads to pain perception

BASIC STEPS: PAIN PROCESSING
• Transduction
• Transmission
• Perception
• Modulation

Mechanical Thermal
Chemical
Judith A. Paice, AAHPM, 2008
Aδ or C fibers
PAIN TRANSDUCTION

TRANSMISSION
• Stimulus to cord
• Cord to brain stem
• Brain stem to higher cortex

Thalamus
Somatosensory Cortex
Associative Cortex
Judith A. Paice, AAHPM, 2008
TRANSMISSION

PERCEPTION
• Experience• Conscious
• Multidimensional
• Interaction of transmission/transduction

MODULATION
• Changing
• Inhibiting
• Spinal cord level

PAIN PROCESSING
• Transduction
• Transmission
• Modulation
• Perception

CLASSIFICATION OF PAIN
• Physiologic• Nociceptive
• Neuropathic
• Mixed
• Temporal• Acute
• Chronic

NOCICEPTIVE PAIN
• Somatic
• Visceral
• “Sharp” “Aching” “Throbbing”

NEUROPATHIC PAIN
• Damaged or dysfunctional nerves
• Central
• Peripheral
• “Burning” “Tingling” “Numbness” “Electric”

MIXED PAIN
• Experiencing • nociceptive
and
• neuropathic

CLASSIFICATION OF PAIN
• Physiologic• Nociceptive
• Neuropathic
• Mixed
• Temporal• Acute
• Chronic

TEMPORAL CLASSIFICATION: ACUTE
• Sudden or recent onset
• Identifiable cause
• Short duration
• Sympathetic response

TEMPORAL CLASSIFICATION: CHRONIC
• Persistent
• May have no obvious cause
• Prolonged functional impairment
• No sympathetic response

INTERVAL SUMMARY
Understanding the pathophysiologyleads to improved assessment and
targeted management that will improve outcomes

PAIN ASSESSMENT
1. Location2. Description (type)3. Change over time4. Severity (0 – 10)5. Effect of
treatments• Benefit (+)• Unwanted effects (-)

1. LOCATION
• Where is it ? • Does it move ?

2. DESCRIPTION
• What does the pain feel like ?
• Does it ever feel burning or shooting ?
• How does the pain impact your life ?

• Constant
• Breakthrough
• Intermittentacute
3. CHANGE OVER TIME

4. PAIN SEVERITY = 5TH VITAL SIGN
29


5. EFFECT OF TREATMENTS
• Therapies tried• What worked ?• What didn’t work ? • Any affects you
didn’t like ?

EXAMINATION
• General exam• Changes in behavior• Focused exam• Psychological exam

INTERDISCIPLINARY TEAM
• Physician•Assess•Diagnose•Prescribe•Monitor•Communicate
• Nurse•Assess•Deliver•Monitor•Teach•Communicate
• Pharmacist•Assess•Provide•Monitor•Teach•Communicate

INTERVAL SUMMARY
Assessment of pain requires a thoughtful history and physical. Standardizing the
process helps prevent miscommunication.

PAIN MANAGEMENT: DEFINITIONS
• Opioid: anything that binds the opioid receptor
• Opiate: derived from the opium poppy (Papaver somniferum)
• Narcotic: archaic term, associated with illicit use
35

PAIN MANAGEMENT PRINCIPLES
• Don’t delay control
• Unmanaged pain nervous system changes
• Treat underlying cause

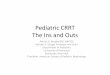
WHO LADDER
1, Pain 1 – 3
2, Pain 4 – 6
3, Pain 7 – 10
Morphine
Hydromorphone
Fentanyl
Oxycodone
Methadone
Levorphanol
± Adjuvants
Codeine
Tramadol
A / Codeine
A / Hydrocodone
A / Oxycodone
A / Dihydrocodeine
± Adjuvants
ASA
Paracetamol / Acetaminophen
NSAID’s
± Adjuvants WHO. Geneva, 1996.

Pla
sma
Co
nce
ntr
atio
n
0 Time
AbsorptionExcretion
First Order KineticsWhen biological effect
follows plasma concentration

Pla
sma
Co
nce
ntr
atio
n
0
Maximum Concentration ( Cmax )
20
10
= maximum concentration during the dosage interval
Cmax
Time ( hours )4

Pla
sma
Co
nce
ntr
atio
n
0 Time ( hours )
Time to MaximumConcentration ( t Cmax )
20
10
1 4
= time it takes to get to maximum concentration
Cmax MorphinePO / PR
Cmax = 1 hour

Pla
sma
Con
cen
trat
ion
0 Half-life (t1/2) Time
IV
PO / PR
SC / IM
Cmax
Time to MaximumConcentration ( t Cmax )

Pla
sma
Co
nce
ntr
atio
n
0
Half-Life ( t ½ )
Morphineall routes
t ½ = 4 hours
20
10
= time it takes for the body to excrete half the dose
Time ( hours )4

CLEARANCE CONCERNSMORPHINE
Liver
•Morphine M3G . . .
M6G . . .
Analgesia CNS
+ +++
++++
Collins SL, et al. J Pain Symptom Manage. 1998.Mercadante S, Arcuri E. J Pain. 2004.
Urine90 – 95 %

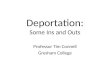
PRINCIPLEFOR CONTINUOUS PAIN
For constant pain
• To achieve steady-state, dose routinely every
half-life ( t ½ )

CONTINUOUS PAIN PRINCIPLE

Pla
sma
Co
nce
ntr
atio
n
0
Dosing every half-life ( t ½ )Oral morphine = 4 hours
164 8 12Time ( hours )20 24
50%75%
87.5%93.75%
97%100%

Pla
sma
Co
nce
ntr
atio
n
0 Time
Steady state after 5 half-livesMorphine ≈ 20 hours
Peak
TroughConcentration
needed to control pain
Concentration where side-effects
start to occur

PRINCIPLEFOR BREAKTHROUGH PAIN
• Dose once every Time to Cmax
• PO 1 h
• Dose =10% of total 24 hr routine dose

Pla
sma
Con
cen
trat
ion
0 Time
Cmax
Breakthrough Pain
PO / PR≈ 1 hr

OPIOID ADVERSE EFFECTS
Uncommon
• Bad dreams / hallucinations
• Delirium
• Myoclonus / seizure
• Pruritis / urticarial
• Respiratory depression
• Urinary retention
Common
• Constipation
• Dry mouth
• Nausea
• Sedation
• Sweats

EQUIANALGESIC DOSES
Oral/Rectal Analgesic IV/SC/IM
150 Codeine --
15 Hydrocodone --
15 Morphine 5
10 Oxycodone --
3 Hydromorphone 1
51

MORPHINE PO OXYCODONE POMorphine 15 mg PO = Oxycodone 10 mg PO
• Patient is on Morphine ER 90mg BID PO
• Oral Morphine Equivalent?
• (90 mg x 2 = )180mg
• This equals how much Oxycodone?
• ( 180 mg x 15 / 10 =) 120mg
• How much Oxycodone ER?
• 60mg PO BID

MORPHINE PO HYDROMORPHONE IV
Morphine 15 mg PO = Morphine 5 mg IV = Hydromorphone 1 mg IV
• Patient is on Morphine IR 20mg q2hrs PO PRN
• Now can’t take PO, how much HM?
• ( 20mg / 3 then 6.67 mg / 5 =) 1.3mg IV

MORPHINE PO HYDROMORPHONE IV
Morphine 15 mg PO = Morphine 5 mg IV = Hydromorphone 1 mg IV
• Patient is on Morphine ER 90mg BID (OME 180mg)
• How much IV Hydromorphone in a day?
• ( 180mg / 3 then 60 mg / 5 =) 12mg IV / 24hrs

MORPHINE PO HYDROMORPHONE IV
Morphine 15 mg PO = Morphine 5 mg IV = Hydromorphone 1 mg IV
• Patient is getting 8mg IV Morphine hourly PRN without relief
• What is this equal to in Hydromorphone IV?
• ( 8 mg / 5 =) 1.6 mg

INTERVAL SUMMARY
Understanding the way these medications enter and leave the body can help you safely and effective treat pain. Always
have someone independently check your work when changing medications.

SARAH, 43 YO
• Metastatic colorectal CA
• Sacral plexus destruction
• Multiple opioid trials• Pain 6 / 10
• Drowsiness
• Confusion

58
“TOTAL PAIN”

ADJUVANT THERAPIES
• Pharmacological• Interventional Anesthesia
• Non-pharmacological• Acupuncture
• Biofeedback
• TENS
• Counseling
• Integrative therapies

ADJUVANT EVIDENCE
• Therapies extrapolated from non-cancer pain
• Few RCTs
• Very few comparative trials

GUIDING THERAPY
• Diagnosis
• Assessment
• Efficacy
• Safety / tolerability
• Ease of use
• Cost

OPIOIDS
• Nociceptive pain > neuropathic pain
• First-line for mod to severe neuropathic pain
• Titrate to effect or side-effect

METHADONE
• Long half-life
• NOT first order kinetics
• Experienced palliative care / pain experts
• Coanalgesic: 2.5 – 5+ mg
• Cost PO << parenteral

GABAPENTINOIDS
• Sodium channel antagonist
• Positive RCT’s
• NNT less favorable than TCAs
• First-line 2º safety

• Trial gabapentin
•Start 100-300 mg qhs
•Daily, increase 100 mg q8h
•Effective 900 - 1800 mg / 24 hr
•Max 3600 - 5400 mg / 24 hr
• If ineffective, pregabalin
•Start 25-75 mg q12h
•Increase 25 mg q12h
•Effective 100-150 mg / 24 hr
•Max 300 - 600 mg / 24 hr
GABAPENTINOIDS…

ANTIDEPRESSANTS
• 3º amine TCAs (amitriptyline)
• 2º amine TCAs (desipramine, nortriptyline)
• Mixed SNRIs (duloxetine, venlafaxine)
• SSRIs (citalopram, paroxetine)

OTHER ANTICONVULSANTS
• excitation
• Limited data, trial-and-error
• Newer drugs have better safety profiles

CORTICOSTEROIDS
• Limited data, widely used in • Bone pain
• Neuropathic pain
• Lymphedema
• Other conditions
• Dexamethasone• Start high dose 8+ mg daily
• Taper to lowest effective dose

OTHER OPTIONS
• Lidocaine (IV or SC)
• Sodium channel blockade
• Good evidence
• Ketamine (PO, IV, SC)
• NMDA blocker
• Dose-limiting psychological effects

SARAH, 43 YO, CA COLON
• Touch
• Simplify meds ( ! )
• Address total suffering
• Feb 14…Pain 6 / 10

INTERVAL SUMMARY
Sometimes the best long-acting medicine for a patient may not be an opioid. Poor
opiate-responsiveness is a sign that multimodal therapies may be necessary
to achieve pain relief.

CLARIFYINGADDICTION

TOLERANCE
• Reduced effectiveness over time
• Not clinically significant with chronic dosing
• Suspect disease progression

PHYSICAL DEPENDENCE
• Process of neuro-adaptation
• Abrupt cessation withdrawal
• Titrate down if stopping
• Avoid antagonists

DRUG DIVERSION
• Regulation
• Record keeping
• Accountability

PSEUDO-ADDICTION
• Most common cause of apparent drug ‘ failure ’ is under-dosing
• Behavior LOOKS like drug seeking

ADDICTION: CHARACTERISTICS
• Psychological dependence
• Compulsive use
• Loss of control over drugs
• Loss of interest in pleasurable activities

ADDICTION: HALLMARK
• Continued use of drugs in spite of harm
• Rare outcome of pain management

SUBSTANCE USERS
• Can have pain too
• Treat with compassion
• Consultation with pain or addiction specialists

INTERVAL SUMMARY
True addiction is rare in the management of pain and pain can occur in those with a
history of substance use.

SUMMARY
81
• Pain may be nociceptive, neuropathic or both and the history tells you which.
• A standardized approach to the assessment of pain helps prevent miscommunication.
• For constant pain, dose on the half-life (q4hrs). For breakthrough pain, dose on the Cmax (route-dependent).
• True addiction is uncommon in pain management.

THE INS AND OUTS OF PAIN
Kyle P. Edmonds, MDFaculty, UCSD Division of Palliative Medicine
928.853.1483
Kylepedmonds.com