Embed Size (px)
Citation preview
Endoscopic Therapy for Barrett’s EsophagusTechnique is Everything
Sri Komanduri MD MS
Director of Interventional Endoscopy
Associate Professor of Medicine
Section of Gastroenterology
Feinberg School of Medicine
Northwestern University
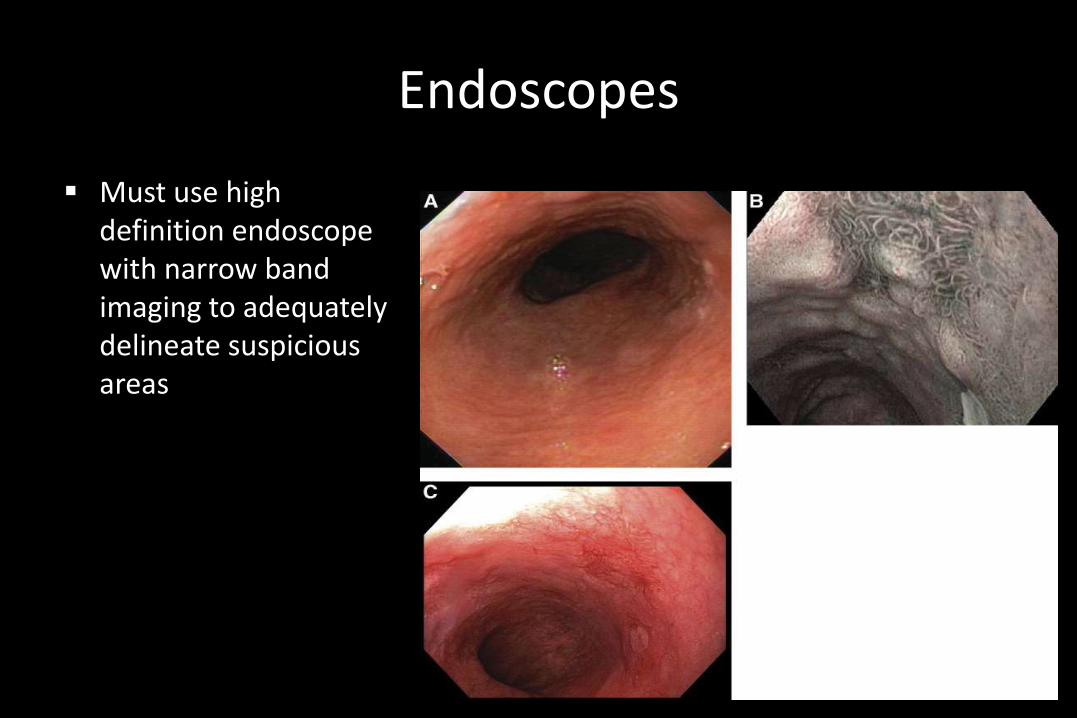
Endoscopes
Must use high definition endoscope with narrow band imaging to adequately delineate suspicious areas
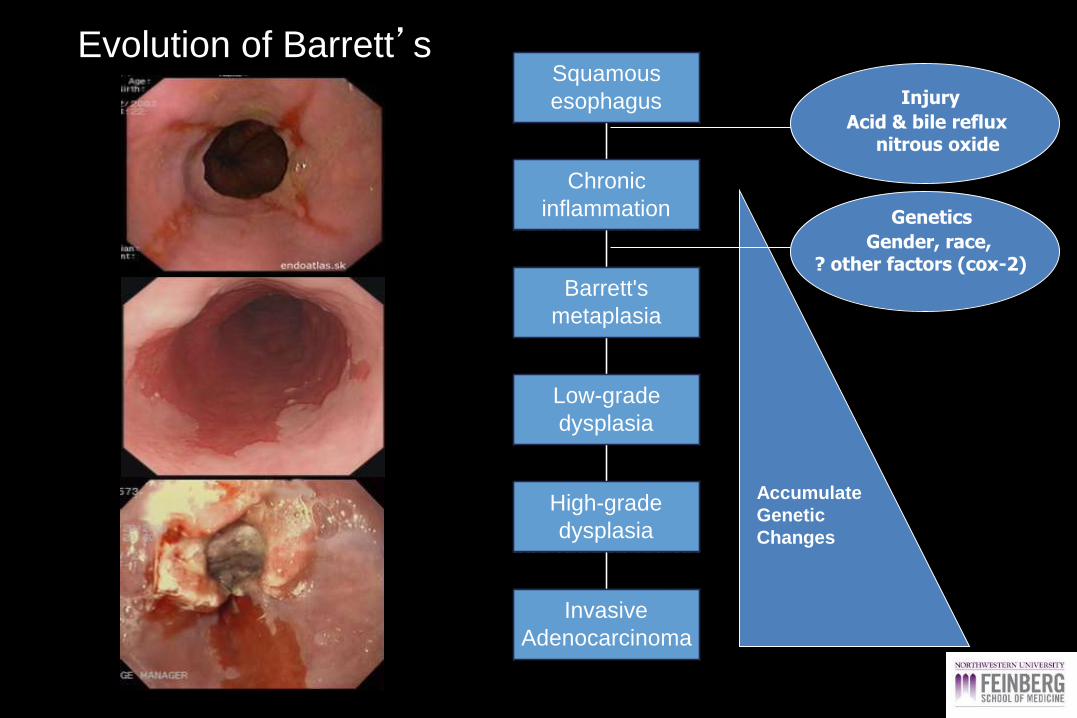
Invasive
Adenocarcinoma
High-grade
dysplasia
Low-grade
dysplasia
Barrett's
metaplasia
Chronic
inflammation
Squamous
esophagus
Accumulate
Genetic
Changes
Injury
Acid & bile refluxnitrous oxide
Genetics
Gender, race,? other factors (cox-2)
Evolution of Barrett’s

HALO Ablation Catheters
HALO360+
HALO90HALO60HALOULTRA
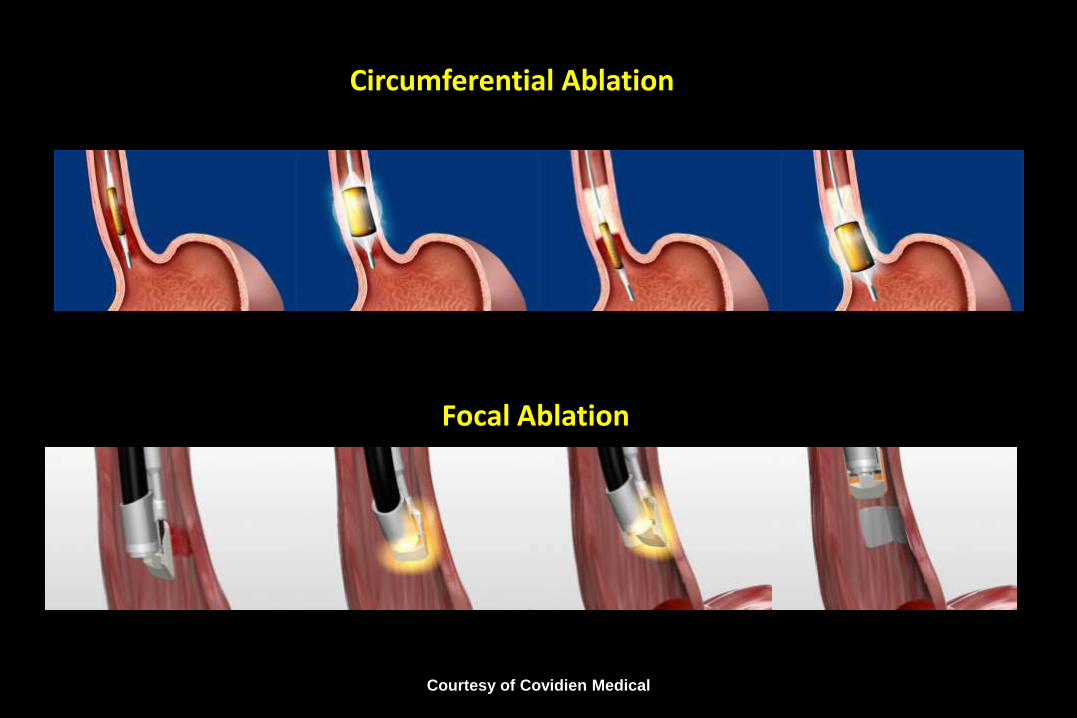
Circumferential Ablation
Focal Ablation
Courtesy of Covidien Medical
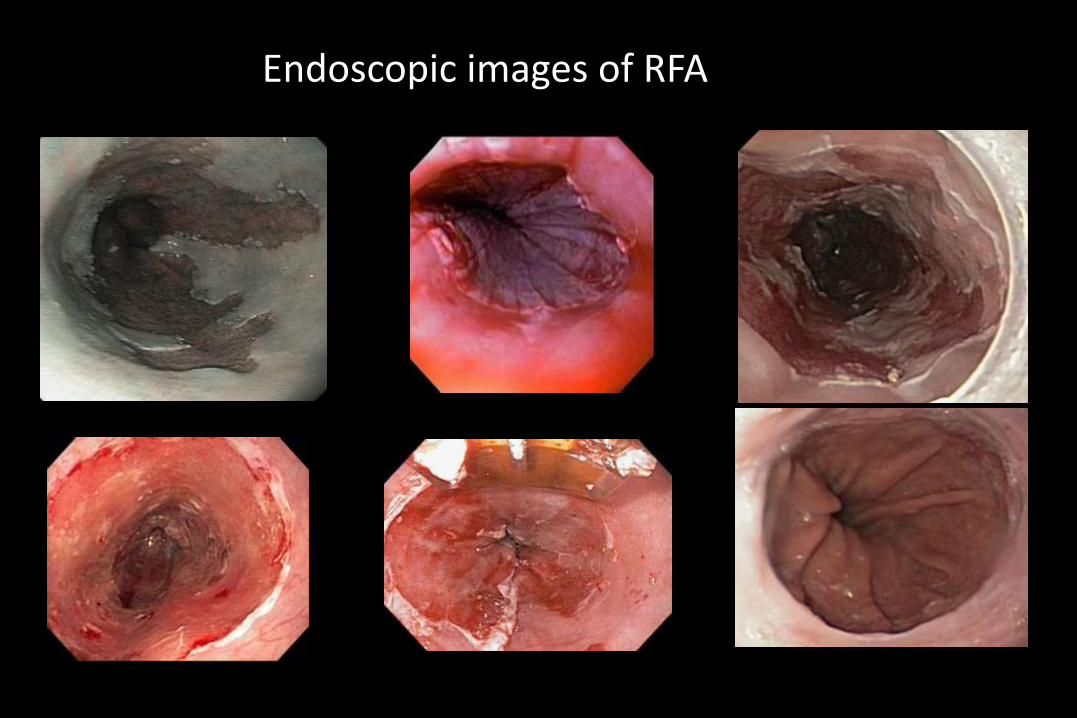
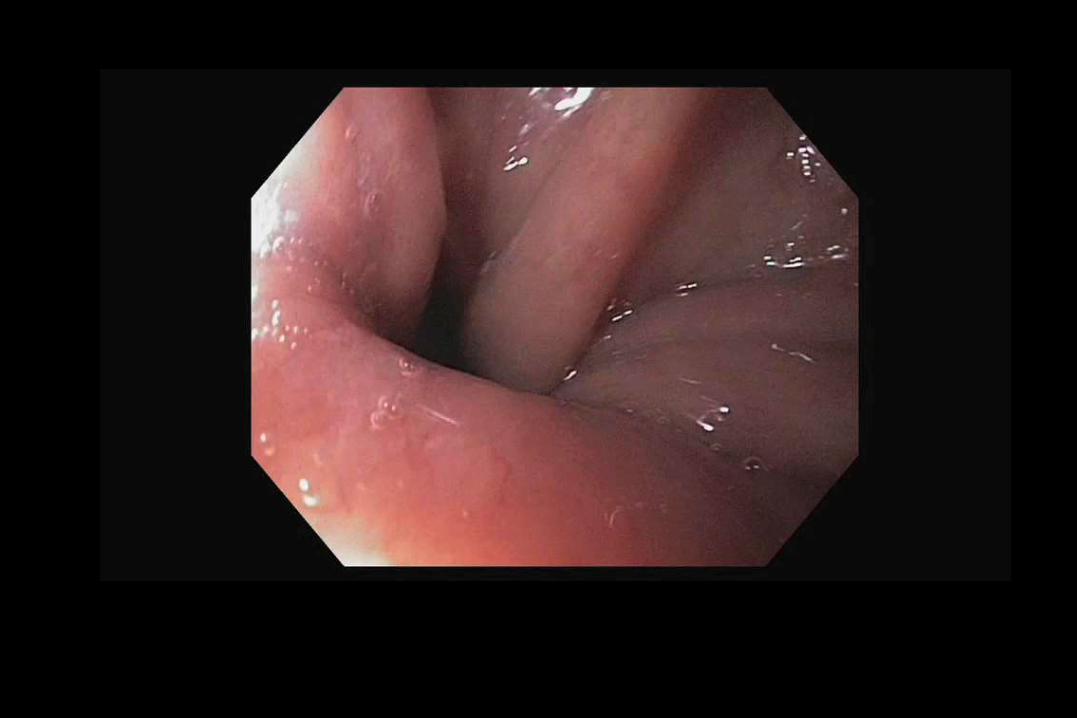
Endoscopic images of RFA

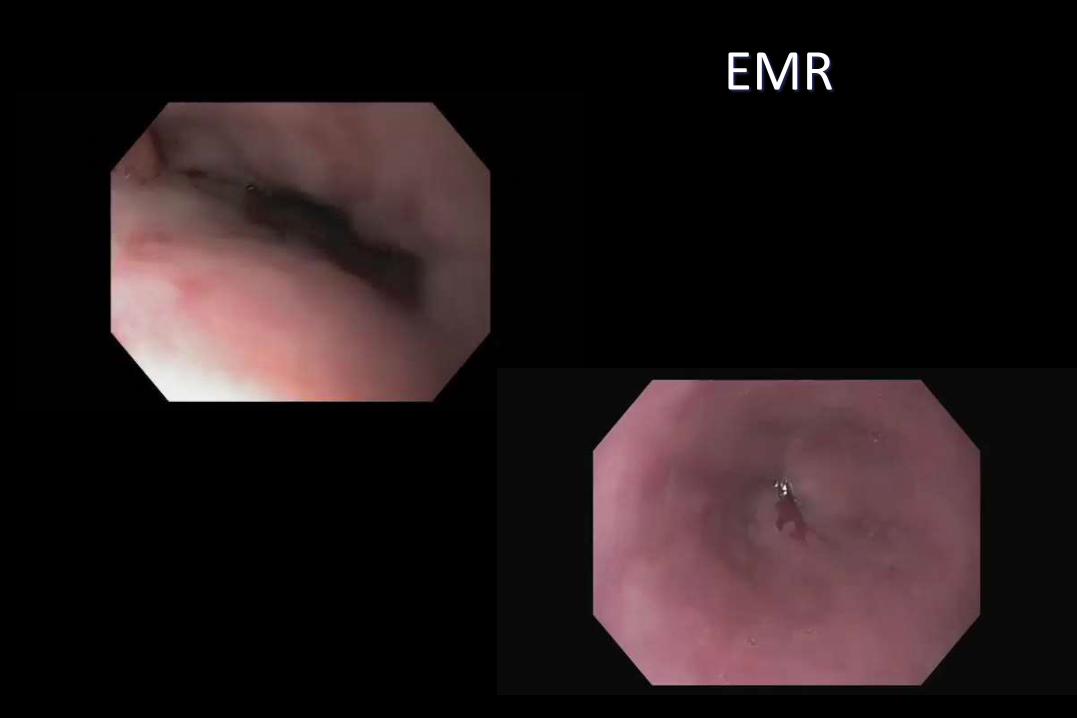
EMR
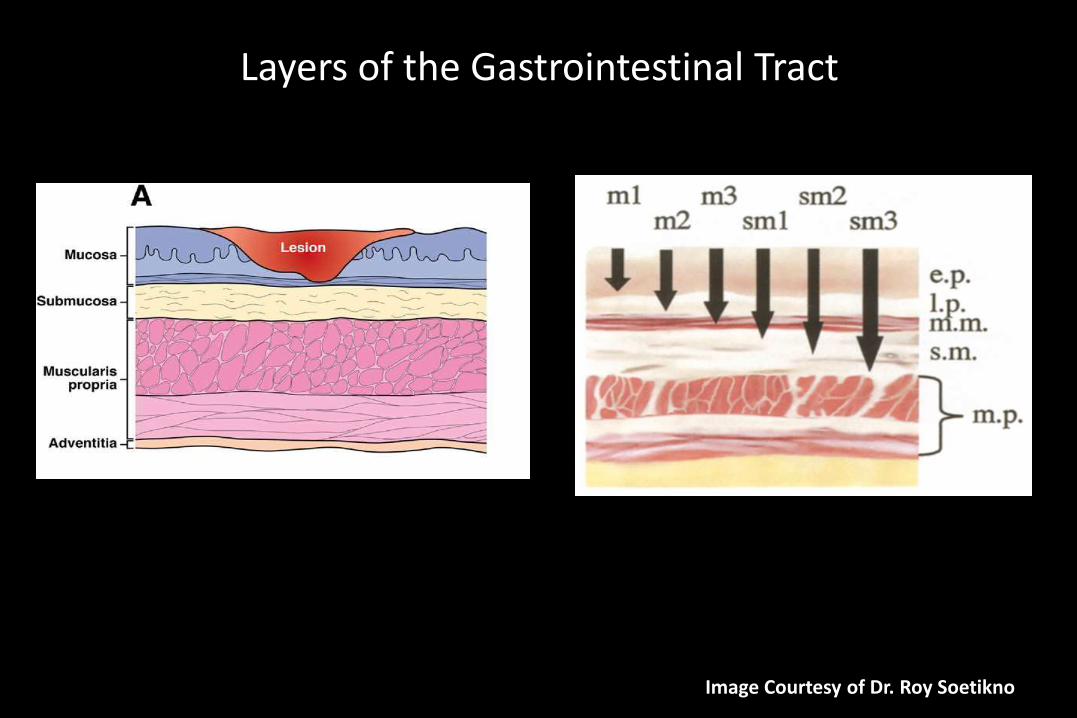
Layers of the Gastrointestinal Tract
Image Courtesy of Dr. Roy Soetikno
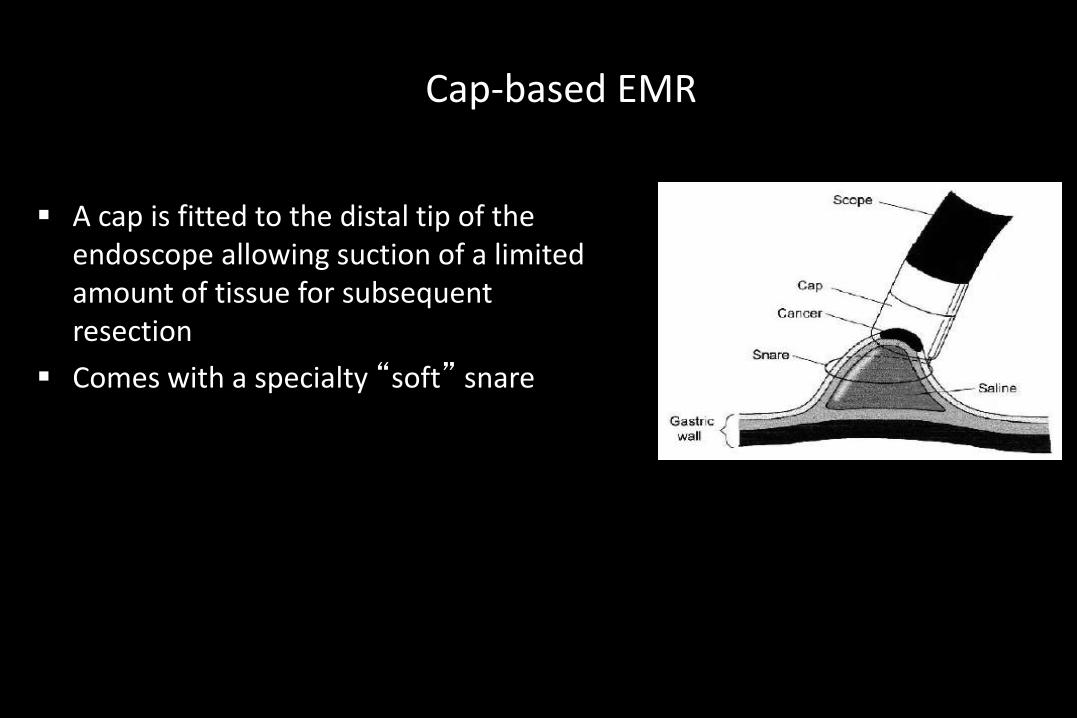
Cap-based EMR
A cap is fitted to the distal tip of the endoscope allowing suction of a limited amount of tissue for subsequent resection
Comes with a specialty “soft” snare
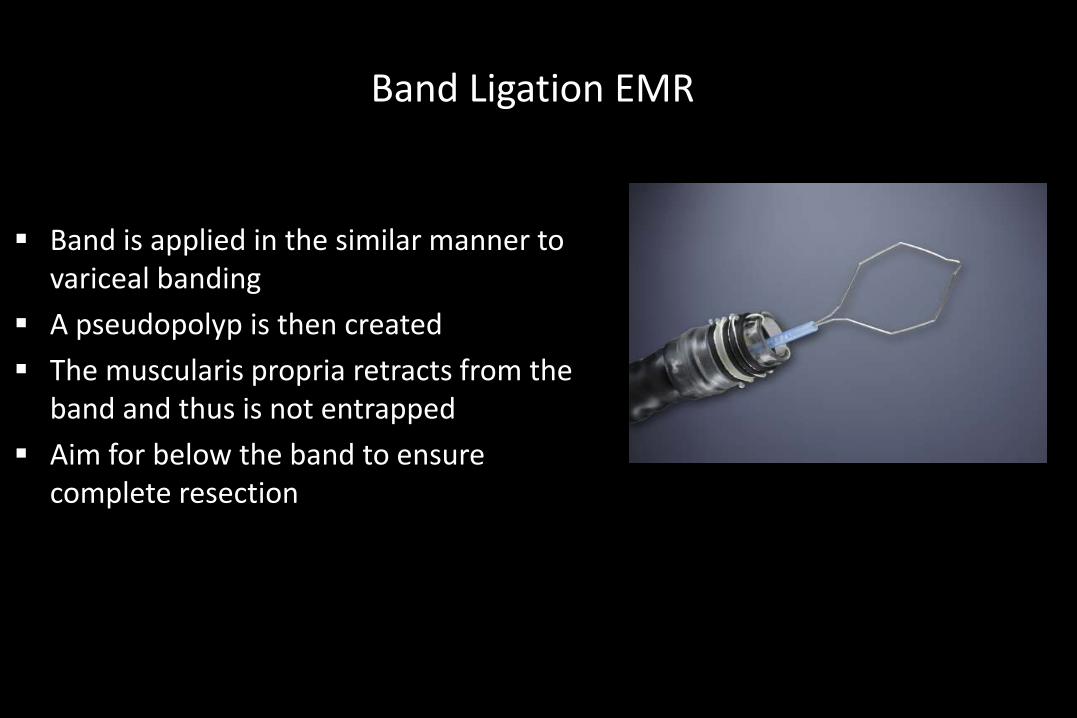
Band Ligation EMR
Band is applied in the similar manner to variceal banding
A pseudopolyp is then created
The muscularis propria retracts from the band and thus is not entrapped
Aim for below the band to ensure complete resection
Band versus Cap
Have been compared in two prospective studies
– Size of lesions obtained with band is smaller, but depth is not
– Increased complications with cap technique (3/39 with perforation in cap group, none in band group)
Early Esophageal Adenocarcinoma
Risk of lymph node metastases:
• Tis (intraepithelial,HGD) 0
• T1a (intramucosal) 1-2%
• T1b (submucosal) 25%
Hulscher, et al. N Engl J Med 2002;347:1662-1669Dunbar, Spechler. Am J Gastroenterol 2012;107:850-62
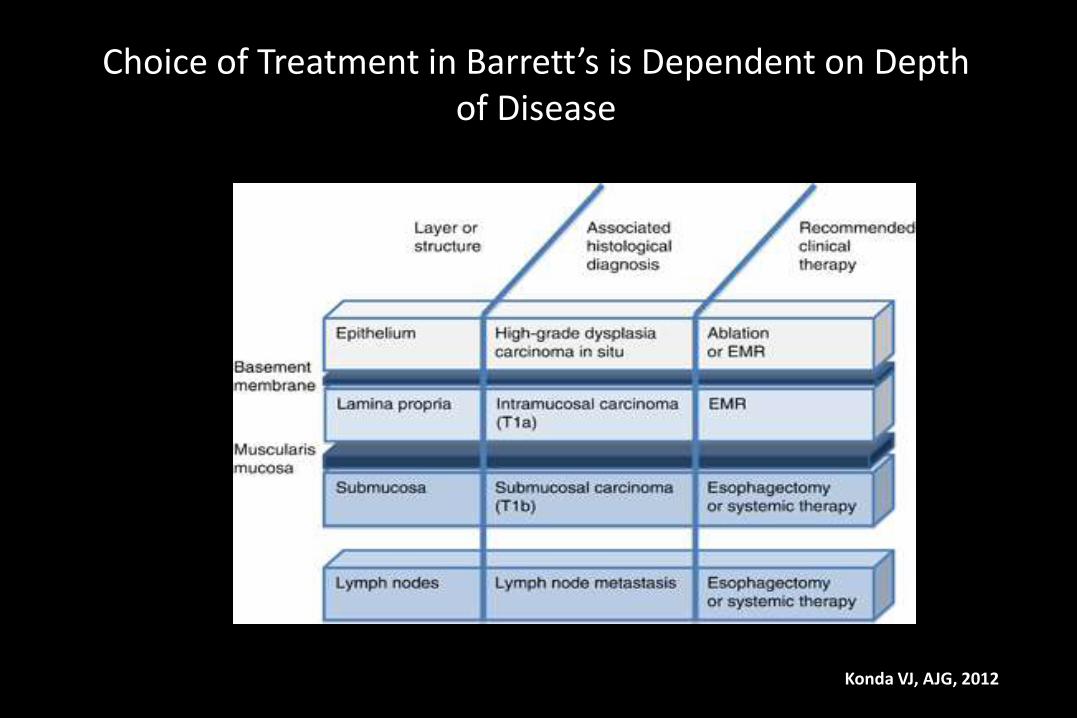
Choice of Treatment in Barrett’s is Dependent on Depth of Disease
Konda VJ, AJG, 2012
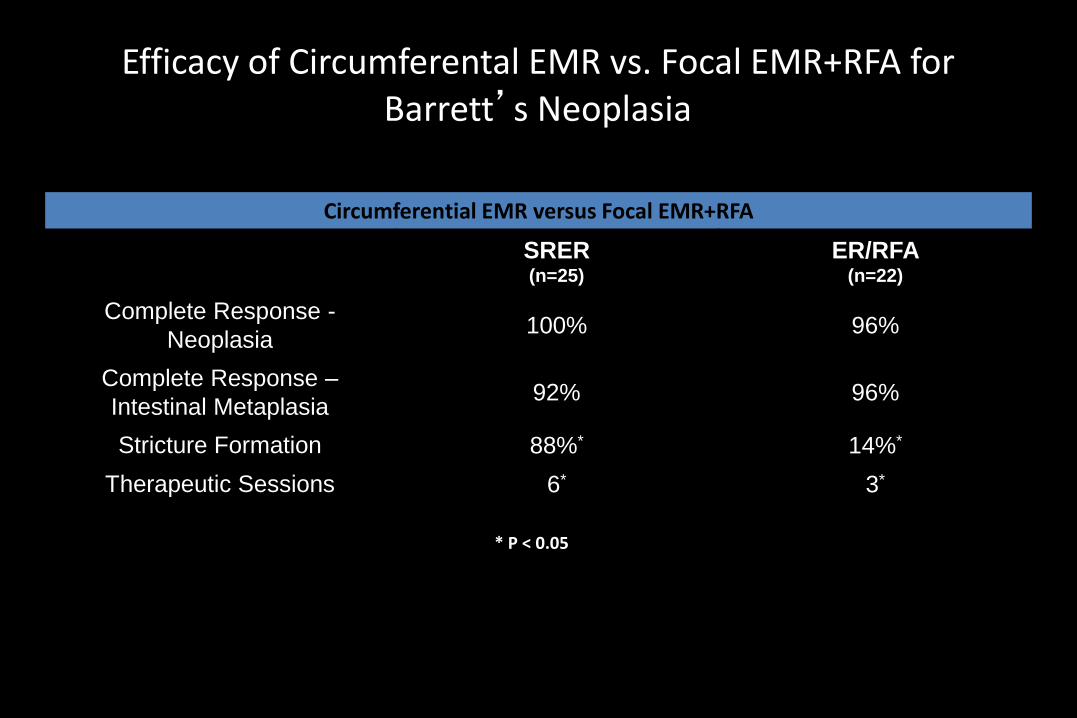
Efficacy of Circumferental EMR vs. Focal EMR+RFA for Barrett’s Neoplasia
Circumferential EMR versus Focal EMR+RFA
SRER(n=25)
ER/RFA(n=22)
Complete Response -
Neoplasia100% 96%
Complete Response –
Intestinal Metaplasia92% 96%
Stricture Formation 88%* 14%*
Therapeutic Sessions 6* 3*
* P < 0.05
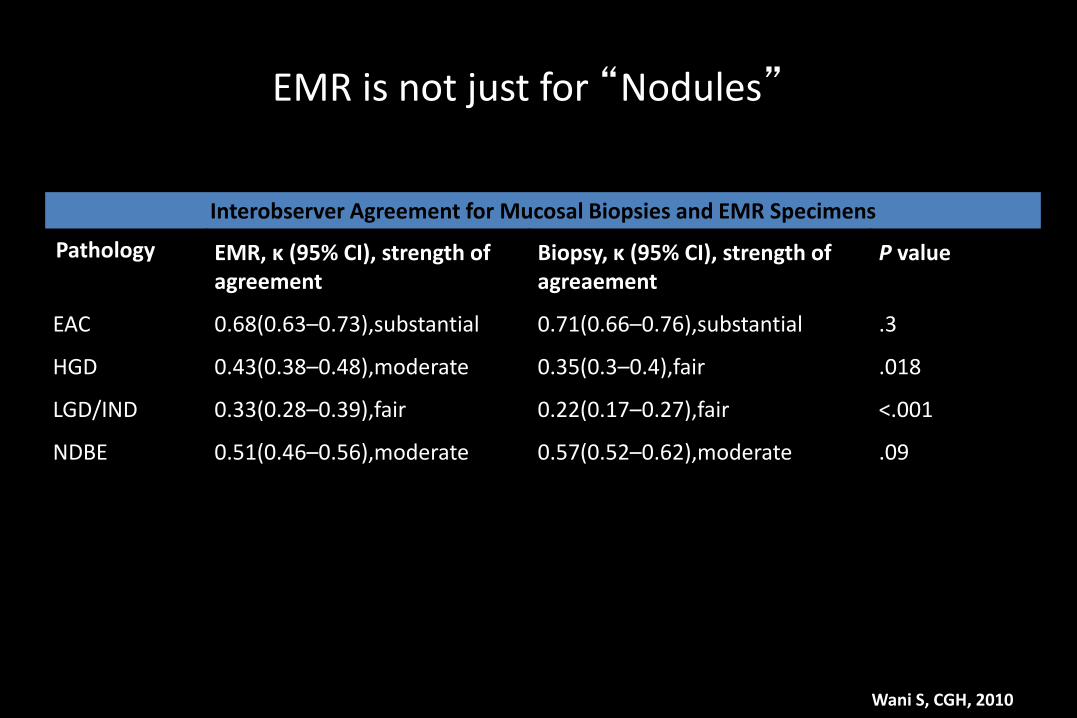
EMR is not just for “Nodules”
Interobserver Agreement for Mucosal Biopsies and EMR Specimens
Pathology EMR, κ (95% CI), strength of agreement
Biopsy, κ (95% CI), strength of agreaement
P value
EAC 0.68(0.63–0.73),substantial 0.71(0.66–0.76),substantial .3
HGD 0.43(0.38–0.48),moderate 0.35(0.3–0.4),fair .018
LGD/IND 0.33(0.28–0.39),fair 0.22(0.17–0.27),fair <.001
NDBE 0.51(0.46–0.56),moderate 0.57(0.52–0.62),moderate .09
Wani S, CGH, 2010
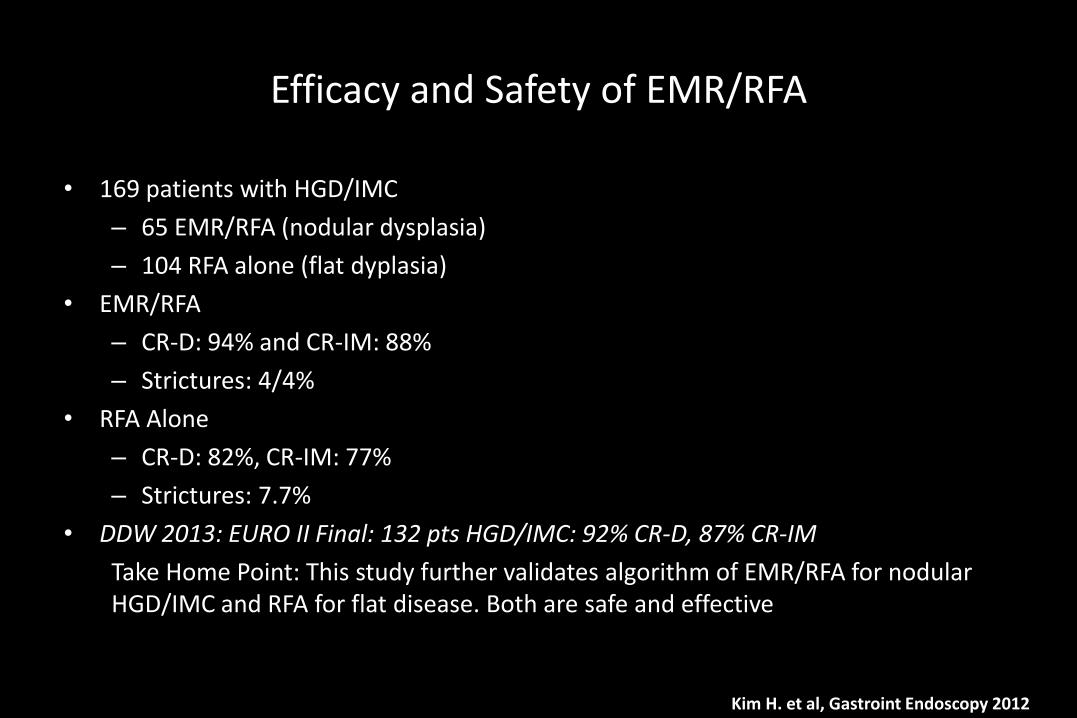
Efficacy and Safety of EMR/RFA
• 169 patients with HGD/IMC
– 65 EMR/RFA (nodular dysplasia)
– 104 RFA alone (flat dyplasia)
• EMR/RFA
– CR-D: 94% and CR-IM: 88%
– Strictures: 4/4%
• RFA Alone
– CR-D: 82%, CR-IM: 77%
– Strictures: 7.7%
• DDW 2013: EURO II Final: 132 pts HGD/IMC: 92% CR-D, 87% CR-IM
Take Home Point: This study further validates algorithm of EMR/RFA for nodular HGD/IMC and RFA for flat disease. Both are safe and effective
Kim H. et al, Gastroint Endoscopy 2012
Histologic Caveats for EMR
Deep resection margin
Submucosal Invasion
Lymphovascular invasion
Tumor differentiation
Lateral Margin
Most of these can be determined en bloc or piecemeal
**More local recurrence post piecemeal (rare)
138 patients EMR for dysplastic BE
31 % change in diagnosis
– 10% Upstage to EAC, 20% downstage
EMR is an essential staging and therapeutic modality for EET dysplastic BE or early esophageal cancer
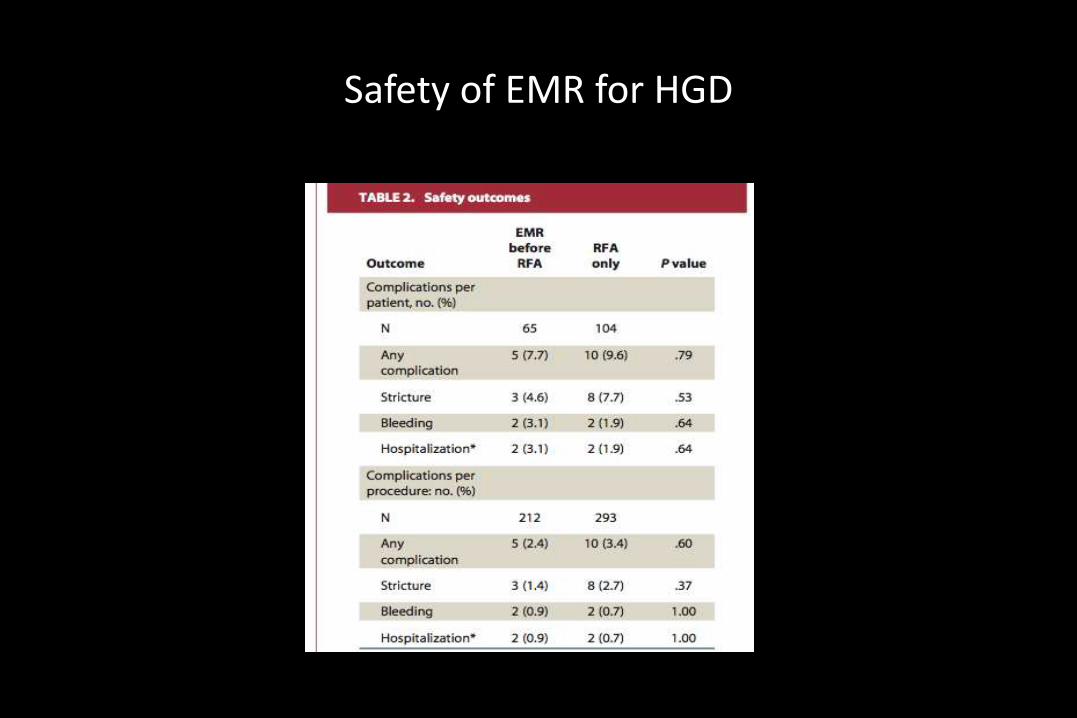
Safety of EMR for HGD
Tomizawa Y et al Am J Gastro 2013
RFAPatient Pearls
• Proper Consent and Discussion Prior is Priceless
• Prepare the patients mentally for pain
• There should be a clear understanding that this a
treatment for Barrett’s NOT GERD
• Involve your surgeons or multifocal HGD/IMC
• Spend some time on post-RFA diet
• A picture is always worth a 1000 words…
• Give them your cell phone number
RFAClinical Pearls
• Proper Patient Selection/Team Selection
• See All Patients in Clinic first
• MAC is ideal
• Give ample time in patients post EMR
• Stringent protocol for anticoagulation/antiplatelet tx
• Acid suppression is essential (ph/impedance)
• Avoid early endoscopy
• Meet with patients after CR-IM to establish long term GERD plan
RFATechnical Pearls
• Listen to your rep!
• Follow the IFU’s to a tee (Despite intuition)
• Take time sizing
• The smallest measurement is the best one! (Mostly)
• The ULTRA focal ablation device may provide better therapy for some
patients 1st treatment
• Respect the Hiatal Hernia. Make sure the patient understands the fight is not
over after CR, it actually has just begun…
RFATechnical Pearls
• There is a feeling that focal ablation is “easier”. Proper focal therapy
is much more difficult than the 360
• Be meticulous at every step. No cutting corners!
– Confirmation of pathology
– Measurements
– Utilization of mucomyst and NBI
– Cleaning of “all” the coagulum
– Sizing the entire 12+ centimeters
– Good final look and photo documentation
– The Big Brother Theory: Ask for Help
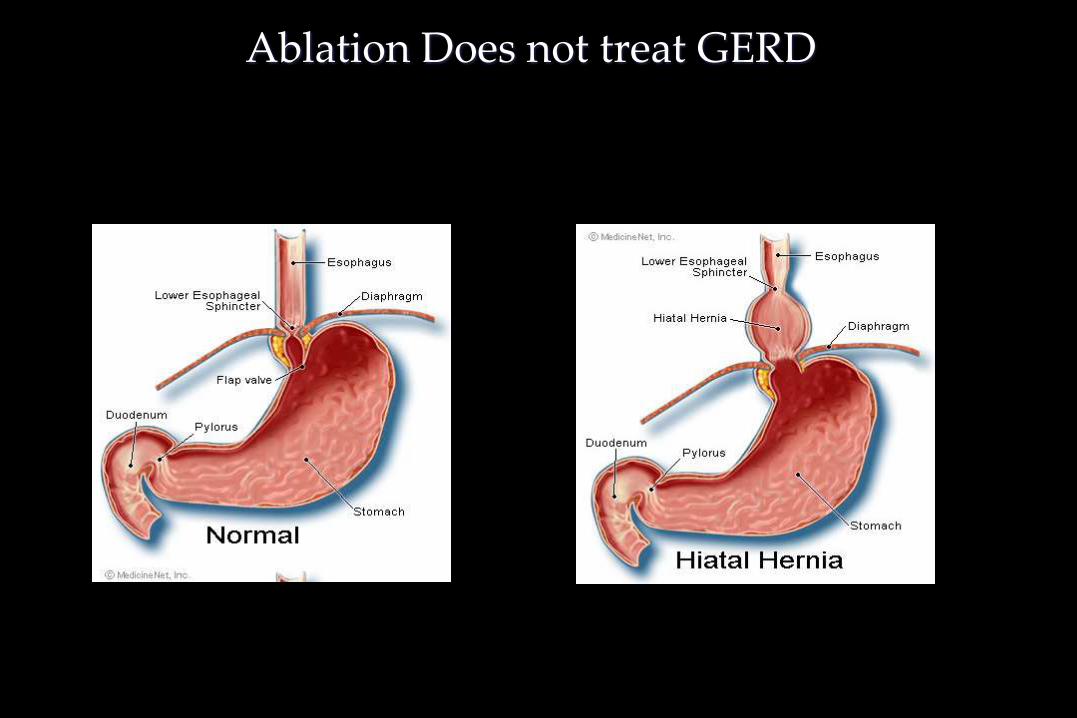
Ablation Does not treat GERD
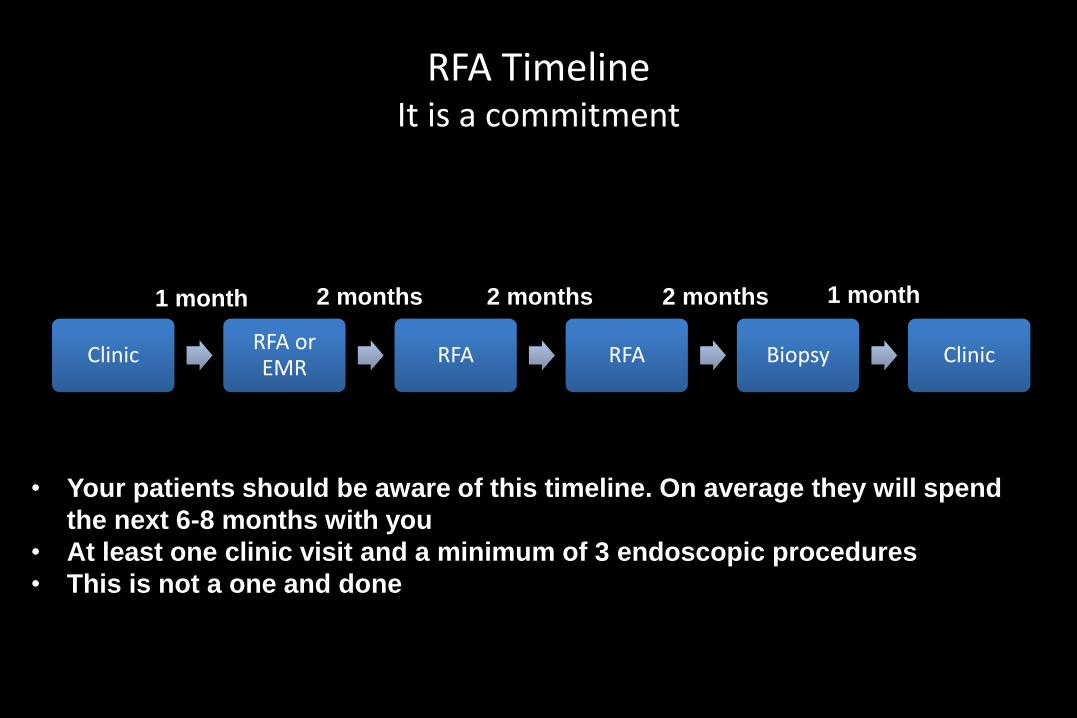
RFA TimelineIt is a commitment
ClinicRFA or EMR
RFA RFA Biopsy Clinic
2 months 2 months 2 months 1 month
• Your patients should be aware of this timeline. On average they will spend
the next 6-8 months with you
• At least one clinic visit and a minimum of 3 endoscopic procedures
• This is not a one and done
1 month

RFA for GAVE
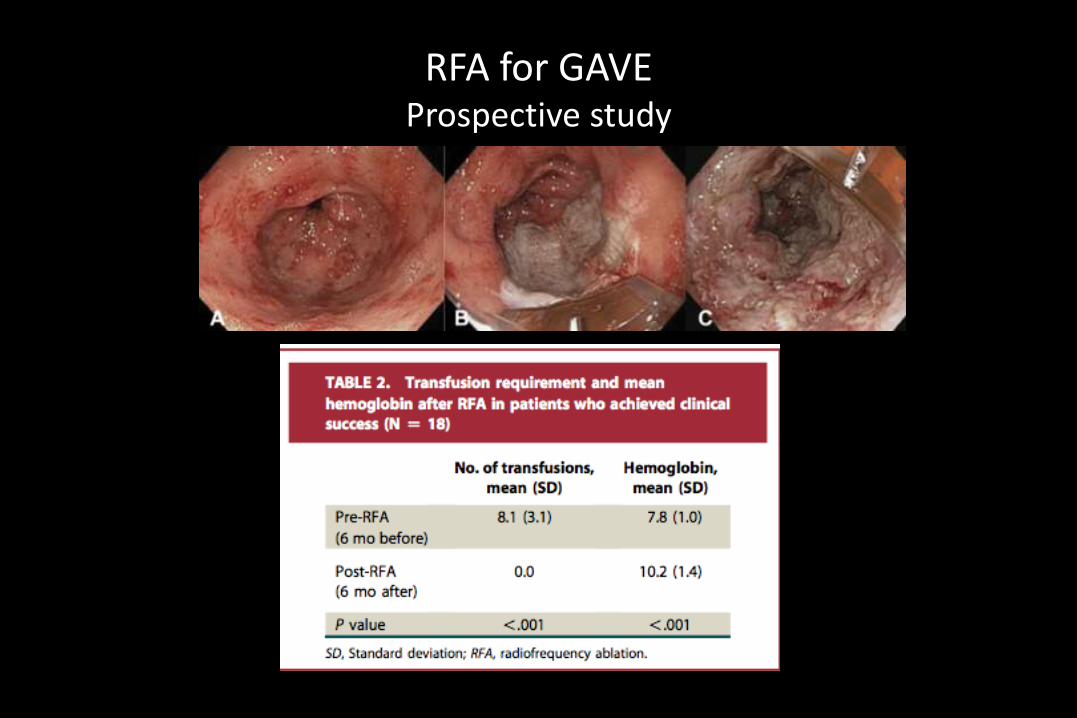
RFA for GAVEProspective study
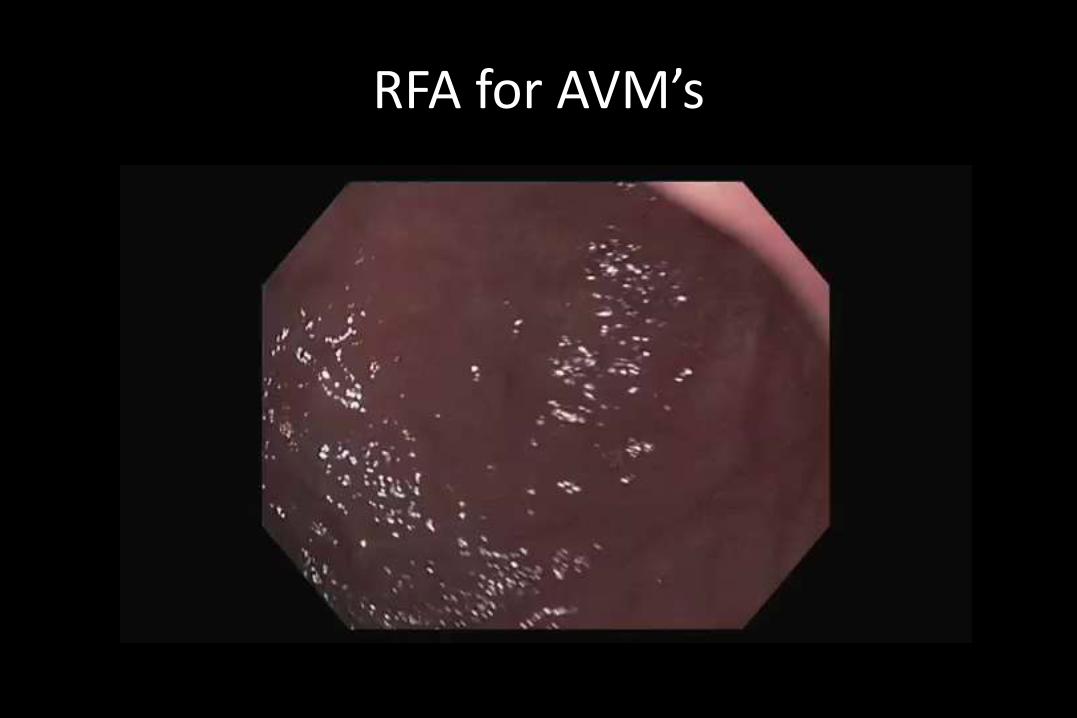
RFA for AVM’s
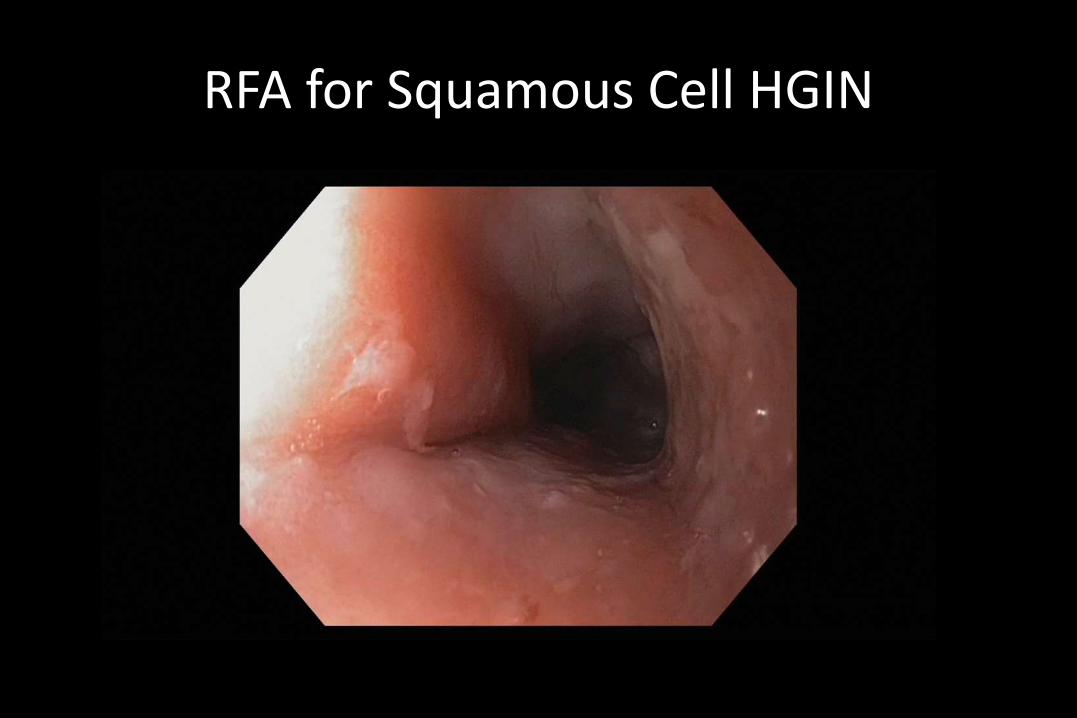
RFA for Squamous Cell HGIN
Endoscopic Therapy of Barrett’s Esophagus:Take Home Points
Should I be treating?
Time commitment
Training and education
Proper patient selection
HGD (EMR skill and EUS availability)
Access to Multidisciplinary team
Then Yes!
The future: Let’s move on from who to ablate and see the forrest from the
trees:
Biomarkers
Screening: Transnasal endoscopy, Cytosponge,…
Endoscopic Therapy of Barrett’s Esophagus:Take Home Points
Are we ready to treat everyone? No!
Are we ready to treat selectively? Yes!
– Almost all with HGD (EMR/RFA)
– Most with confirmed LGD (RFA)
– Some with NDBE with clinical factors indicating increased risk
Buried glands and Recurrence:
Imperative to have proper EMR technique (wide and often!)
Physiologic testing for incomplete responders to RFA





























