Embed Size (px)
Citation preview

Specialty Drug Benefit Design and Patient Out-of-Pocket Costs in the ACA Marketplaces
Erin Taylor, Dan Han, Andrew Mulcahy, and Christine Eibner
June 2015
A10793-ET-2
Expensive “specialty” drugs are becoming more prevalent
• Generally biologic products for chronic conditions, prescribed by specialists
• Usually very effective treatments
• Often very expensive, due to:– Few substitutes
– Costly to produce
• Annual treatment costs can exceed $40,000– 30-day supply of adalimumab = $2,905
(Part D average)
– Sovaldi course of treatment = $72,000
• Pose financial burden for both patients and payers (government and insurers)

A10793-ET-3
To address costs, insurers are altering the traditional cost sharing structure
Generic
Copay*=$12
Copay*=$45
Copay*=$75
Traditional 3-tier formulary with modest, fixed copays
Insurers negotiate discounts with manufacturers for preferred placement lower premiums
* Average copayments for Silver plans in Marketplace
Non-preferred brand
Preferred brand

A10793-ET-4
To address costs, insurers are altering the traditional cost sharing structure
Generic Preferred brand Non-preferred brand
Copay*=$12
Copay*=$45
Copay*=$75
Increasing use of higher cost sharing tiers
Complex cost sharing arrangemen
ts
Specialty
* Average copayments for Silver plans in Marketplace

A10793-ET-5
Specialty tiers raise questions about tiered formularies
• Specialty drug users have always faced high costs
• Affordable Care Act (ACA) increased access to insurance– Did it go far enough for
specialty drugs?
• Costs may deter utilization (moral hazard)– Out-of-pocket maximum limits
may temper effects of high cost sharing
• Costs may also deter enrollment (adverse selection)

A10793-ET-6
Focus of this Study
• Comparing coverage of specialty drugs in 37 Marketplaces
• Simulate patient out-of-pocket costs for specialty drugs– Focus on drugs used to treat rheumatoid arthritis, HIV, organ
transplants, and multiple sclerosis– Compare costs in ACA Marketplace plans to costs incurred by Medicare
Part D patients taking same drugs
• Data sources– Publicly available benefit design data, MEPS prescription drug utilization– Assumptions related to medical benefits utilization
• Part D is a reasonable comparator because:– Both offered by private insurers that are subject to regulation– Coverage under Part D is also subject to catastrophic spending limits
A10793-ET-7
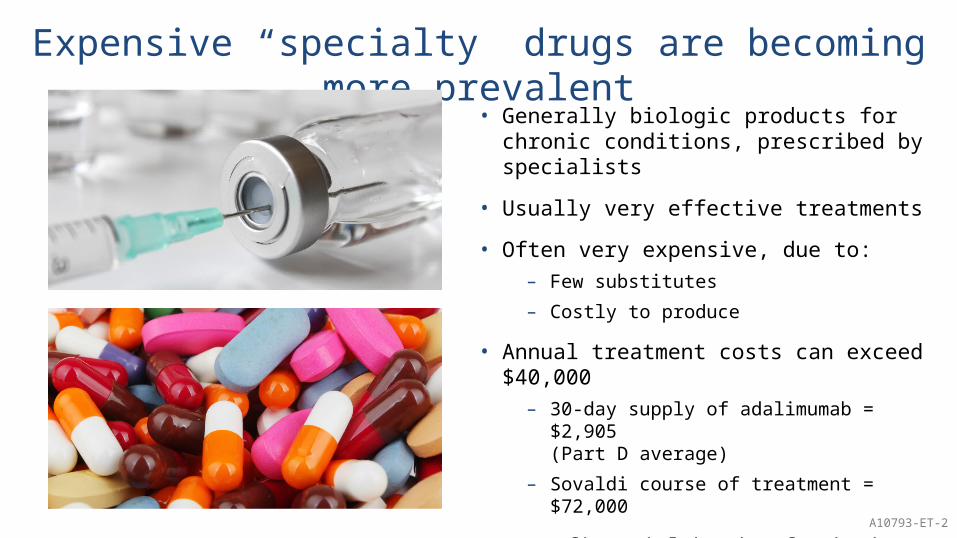
Marketplace plan design is extremely complicated
Bronze60%
Silver70%
Gold80%
Platinum90%
Different metal tiers cover different levels of average medical spending
Insurers make tradeoffs to achieve these coverage levels
Higher premiums Lower deductibles
Lower cost sharing
Higher deductibles Lower cost sharing
Higher cost sharingfor some benefits
Lower cost sharingfor other benefits
A10793-ET-8
While plans cover a certain percent of average medical spending . . .
Specialty drug users likely spend more than the
average
This can make selecting a plan more
complicated
BenefitsCosts
Out-of-pocketSpecialty drugs

A10793-ET-9
Specialty drug coverage design is part of a complex puzzle
Then co-payment
Deductible
Deduct-ible
Then nocharge
Deduc-tible
Thencoinsu-rance
Only copayor
coinsurance
Nodeductibl
e
A10793-ET-10
Plans can also combine a drug deductible with a medical deductible
Drugdeductible
Medicaldeductible

A10793-ET-11
Higher proportion of Gold and Platinum plans offer $0 drug deductible
Bronze Silver Gold Platinum0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
4.3%
28.7%
44.6%
78.2%
Metal Tier

A10793-ET-12
On average, more generous plans offer lower deductibles and out-of-pocket
maximums
Bronze Silver Gold Platinum$0
$1,000$2,000$3,000$4,000$5,000$6,000$7,000
Average Deductible
Drug-Only DeductibleIncluded in Medical
Metal Tier Bronze Silver Gold Platinum$0
$1,000$2,000$3,000$4,000$5,000$6,000$7,000
Average Out-of-Pocket Max-imum
Drug-Only OOP Max Included in Medical
Metal Tier

A10793-ET-13
Bronze Silver Gold Platinum0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%60.3%
49.5%44.3%
15.4%
Deductible, then CoinsuranceDeductible, then No ChargeCopayment OnlyCoinsurance Only
Plans offering more generous benefits less likely to charge deductible plus coinsurance for
specialty drugsPercentage of plans offeringthe cost sharing structure
Metal Tier

A10793-ET-14
While ACA established broad Marketplace plan requirements, states may set specialty drug
coverage requirementsSome states have enacted legislation limiting the cost sharing for specialty drugs, for example:
New York: cost sharing no greater than non-preferred brand tierDelaware: cost sharing no greater than $150 per month or $3500 per yearLegislation may be more common in states operating their own Marketplaces (for which we do not have data)
Some states trying to impose one of two types of requirements:• Limits on per-month cost sharing• Annual caps on spending (out-of-
pocket maximums)
Source: Brooker, 2013

A10793-ET-15
Some states have enacted legislation limiting the cost sharing for specialty drugs, for example:
New York: cost sharing no greater than non-preferred brand tierDelaware: cost sharing no greater than $150 per month or $3500 per yearLegislation may be more common in states operating their own Marketplaces (for which we do not have data)
ME
Maine: Specialty drug cost sharing no greater than $3500
per year
While ACA established broad Marketplace plan requirements, states may set specialty drug
coverage requirements
Source: Brooker, 2013

A10793-ET-16
Some states have enacted legislation limiting the cost sharing for specialty drugs, for example:
New York: cost sharing no greater than non-preferred brand tierDelaware: cost sharing no greater than $150 per month or $3500 per yearLegislation may be more common in states operating their own Marketplaces (for which we do not have data)
New York: Specialty drug cost sharing no greater than non-
preferred brand tier
While ACA established broad Marketplace plan requirements, states may set specialty drug
coverage requirements
Source: Brooker, 2013
NY

A10793-ET-17
Variation across states is more likely due to the way ACA is structured than to state-specific
characteristicsSome states have enacted legislation limiting the cost sharing for specialty drugs, for example:
New York: cost sharing no greater than non-preferred brand tierDelaware: cost sharing no greater than $150 per month or $3500 per yearLegislation may be more common in states operating their own Marketplaces (for which we do not have data)
Our analysis indicates that:• In 28 of 37 states, most common specialty drug
design is deductible, then coinsurance
• 5 of 37 states: only coinsurance (2) or copayments (3), no deductible
• Other states offer a mix of coverage types

A10793-ET-18
We found some variation in benefit design across states
Some states have enacted legislation limiting the cost sharing for specialty drugs, for example:
New York: cost sharing no greater than non-preferred brand tierDelaware: cost sharing no greater than $150 per month or $3500 per yearLegislation may be more common in states operating their own Marketplaces (for which we do not have data)
Average cost sharing varies for Silver tier plans:
• Deductible, then coinsurance: 10% to 50%
• Deductible, then copayments: $45 to $276
• Only coinsurance: 25% to 50%
• Only copayments: $75 to $300

A10793-ET-19
On average, more generous plans have lower OOP costs
Medicare OOP cost comparisons vary by drug
Medicare Bronze Silver Gold Platinum$0
$1,000
$2,000
$3,000
$4,000
$5,000
$6,000
$7,000
$8,000$8,000
$7,000
$6,000
$5,000
$4,000
$3,000
$2,000
$1,000
$0
90th percentile
10th percentile
Mean
Adalimumab (rheumatoid arthritis)

A10793-ET-20
On average, more generous plans have lower OOP costs
Medicare OOP cost comparisons vary by drug
Medicare Bronze Silver Gold Platinum$0
$1,000
$2,000
$3,000
$4,000
$5,000
$6,000
$7,000
$8,000$8,000
$7,000
$6,000
$5,000
$4,000
$3,000
$2,000
$1,000
$0
90th percentile
10th percentile
Mean
Interferon beta-1a (multiple sclerosis)

A10793-ET-21
Silver plan enrollees face variation in expected out-of-pocket costs both within and
across statesO
K FL TX MT
AL
MS
SD TN IL AR
NM LA UT
GA KS NJ
SC
OH PA DE
NH WI
IN OR
MO
AZ
ME
VA
AK
WV
NE
NC
WY
ND MI
IA NV
$0
$1,000
$2,000
$3,000
$4,000
$5,000
$6,000
$7,000 $7,000
$6,000
$5,000
$4,000
$3,000
$2,000
$1,000
$0
90th percentile
10th percentile
Interferon beta-1a (multiple sclerosis)

A10793-ET-22
Silver plan enrollees face variation in expected out-of-pocket costs both within and
across statesO
K FL TX MT
AL
LA MS
WV
SD TN GA
NM SC
OH IL NJ
UT
DE
PA WI
MO IN NH
NV
AR
WY
OR KS MI
AZ
ME
NC
AK
VA
NE
ND IA
$0
$1,000
$2,000
$3,000
$4,000
$5,000
$6,000
$7,000$7,000
$6,000
$5,000
$4,000
$3,000
$2,000
$1,000
$0
90th percentile
10th percentile
Mycophenolic acid (organ transplant)

A10793-ET-23
Policy lessons
• Limits on specialty drug cost sharing– To maintain coverage level, must trade off other benefits
• Benefit harmonization – Results in fewer plan parameters
– Can make it easier for consumers to shop and compare plans
• Require plan standardization– Easy comparisons across plans
– Drawbacks:
• Restricts ability to innovate
• May result in worse coverage for people with certain conditions

A10793-ET-24
Why we need to get this right
• Specialty drugs pose an increasing burden on payer budgets, possibly resulting in limited access
• Use of specialty tiers shifts costs to patients, raises concerns about:– Affordability of essential / high-value medicines
– Adverse selection
• Our research explores cost sharing effects on patients and payers
• More research needed to inform potential solutions, for example:– Effects of other payment mechanisms (value-based purchasing,
bundled payment)
– Impacts of biosimilars









![SHRI MALAR ACADEMY - WordPress.com€¦ · 2014-12-18 · SHRI MALAR ACADEMY, kyh; gy kUjJtkid(Nky khbapy;)> khh;nfl;bq nrhirlb vjphpy> frNrhp NkL> Nryk ig-gh] NuhL> m&h. nry : 94864](https://img.pdfslide.us/doc/110x75/5f4bfb5405d6ee5da85db75a/shri-malar-academy-2014-12-18-shri-malar-academy-kyh-gy-kujjtkidnky-khbapy.jpg)