Embed Size (px)
DESCRIPTION
Dr. Matthew Goetz, assistant professor of oncology and pharmacology at the Mayo Clinic, shared his pharmacogenomic research findings related to risks and occurrence of breast cancer. He explained that in order to truly personalize medicine, you must account for all possible theories and variables. Goetz continued to say that although many believe pharmacology to be boring, it is a key component of the future model of care. Some may say, so this drug doesn’t work–why not just try another drug? It’s much more complicated than that.Dr. Goetz touched on the variety of cases in his study in breast cancer patients, some with strange and perplexing results. When giving the same drug to multiple patients, each yielded a variety of different results. Some patients had successful reduction in tumor size, while others resulted in no change and some even experienced tumor growth as a result of the drug. Personalized health care is the answer to this, for lack of a better term, ’shot-in-the-dark’ type of therapy. If physicians can understand each patient’s biology and genetic makeup individually, they can better apply treatments and medications. This would therefore reduce health care costs and enable patients to receive much more efficient treatments.
Citation preview

3013063-1
Tamoxifen And CYP2D6: Using Pharmacogenetics to discover a new drug
Tamoxifen And CYP2D6: Using Pharmacogenetics to discover a new drug
Matthew P. Goetz, MDAssociate Professor of Oncology
Mayo Clinic
CP1229323-1
Ohio State University Center: Conference on Personalized Health Care

3013063-2
Current Applications of Pharmacogenomics in Breast Cancer
• Current state of adjuvant hormonal therapy
• Pharmacogenetics: CYP2D6 and tamoxifen
• Future directions: endoxifen as a novel hormonal therapy for breast cancer
• Current state of adjuvant hormonal therapy
• Pharmacogenetics: CYP2D6 and tamoxifen
• Future directions: endoxifen as a novel hormonal therapy for breast cancer

3013063-3
Breast Cancer2008 (USA)
• Invasive breast cancer: 178,480new cases
• Ductal carcinoma in situ: 62,030 cases
• 2/3 are estrogen positive — candidates for hormonal therapy
American Cancer Society: Breast Cancer Facts & Figures, 2007-2008

3013063-4
0 5 10 0 5 10
Oxford Overview: 5 Years of Tamoxifen vs NotER Positive vs ER Negative
Oxford Overview: 5 Years of Tamoxifen vs NotER Positive vs ER Negative
5 Years Tamoxifen vsNot Recurrence
ER+/ER UnknownEntry age 50
5 Years Tamoxifen vsNot Recurrence
ER+/ER UnknownEntry age 50
5 Years Tamoxifen vs NotRecurrence
ER – Poor PR – Poor
5 Years Tamoxifen vs NotRecurrence
ER – Poor PR – Poor
Re
cu
rren
ce
Re
cu
rren
ce
YearsYears
50
40
30
20
10
0
Control40.3%
Control40.3%
5-yr TAM23.5%
5-yr TAM23.5%
10-yr gain 15.0% (SE 1.1)Logrank 2P<0.0000110-yr gain 15.0% (SE 1.1)Logrank 2P<0.00001
28.228.2
15.115.1
5-yr TAM29.0%
5-yr TAM29.0%
21.321.3
20.820.8
YearsYears
Loss 1.9% (SE 1.5)Logrank 2P>0.1; NSLoss 1.9% (SE 1.5)Logrank 2P>0.1; NS
Control27.1%
Control27.1%

3013063-5
Cohort 1
Direct Comparison of Tamoxifen and an Aromatase
Inhibitor (9,856 Patients)
Ingle et al. SABC 2008

3013063-6
Cohort 1
5 years of AI vs
tamoxifen
ER+
10
0
20
30
40
50
% SE
% SE
0 5 8Years
15.3%AI
12.6%
9.6%
5-yr gain 2.9% (SE 0.7)8-yr gain 3.9% (SE 1.0)
Logrank 2P<0.00001
Years 0-1 2-4 ≥5
AI 1.69 (163/9647) 2.31 (261/11297) 2.33 (160/6879)
Tamoxifen 2.46 (234/9510) 2.81 (307/10938) 2.78 (180/6478)
Rate ratio, 0.67 SE 0.08 0.81 SE 0.08 0.83 SE 0.10 from (O-E)/V -38.4/96.6 -29.5/137.9 -15.7/83.0
Tamoxifen19.2%
Recurrence
Ingle et al. SABC 2008

3013063-7Jin Y et al: J Natl Cancer Inst 97:30, 2005
Tamoxifen Metabolic Pathway (Humans)
CP1230355-21
400-600 nM
5-10 nM
20-180 nM
200-300 nM
Binding affinity relative to estradiol
1.00 for metabolites 4-OH TAM and endoxifen 0.01 for tamoxifen and N-desmethyl tamoxifen

chromosome 22 CYP2D8 (pseudogene)
CYP2D7 (pseudogene)
CYP2D6
functional alleles*1, *2, *35
nonfunctional (null, *0)
*3, *4, *5, *6, *7, *8, *12,*13, *14, *15, *16, *18, *19, *20, *21, *38 ....
CYP2D gene locus
Molecular Basis of the CYP2D6 Polymorphism
> 100 Genetic Variants duplicated alleles*1x2, *2x2, *35x2
low function alleles*9, *10, *17, *41, *59
q13.1

3013063-9
0
20
40
60
80
100
120
140
160
180
Wt/Wt Wt/*4 *4/*4
CYP2D6 Genotype and Endoxifen
Jin Y et al: J Natl Cancer Inst 97:30, 2005
CYP2D6*4 (most common genetic variant associated with the CYP2D6 poor metabolizer state)
P<0.001, r2=0.24
Plasmaendoxifen
(nM)

3013063-10
5 years oftamoxifen(20 mg qd)+ 1 year of
fluoxymesterone(10 mg po bid)
5 years oftamoxifen(20 mg qd)+ 1 year of
fluoxymesterone(10 mg po bid)
5 years of tamoxifen5 years of tamoxifen
NCCTG 89-30-52NCCTG 89-30-52
RRAANNDDOOMMIIZZAATTIIOONN
Postmenopausal women
Postmenopausal women
5 years total therapy5 years total therapy
541 women accrued
541 women accrued
Early ER+
breast cancerEarly ER+
breast cancer

3013063-11
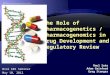
Time to Recurrence According to CYP2D6 MetabolizerStatus* in Women Receiving Adjuvant Tamoxifen
0
20
40
60
80
100
0 2 4 6 8 10 12 14
%
Years after randomization
P<0.001P<0.001
EM/EM, EM/IMEM/EM, EM/IMEM/PM, IM/IM, PM/IMEM/PM, IM/IM, PM/IMPM/PMPM/PM
(n=108)(n=108)
(n=65)(n=65)
(n=16) (n=16)
PM alleles: *3,*4,*6,
IM alleles: *10, *17, *41
Potent CYP2D6 inhibitor = PM/PM
Goetz et al J Clin Oncol. 2005;23(36):9312-8.Goetz M et al. Breast Cancer Res Treat 101:113-121, 2007Goetz et al J Clin Oncol. 2005;23(36):9312-8.Goetz M et al. Breast Cancer Res Treat 101:113-121, 2007

3013063-12
ABCSG Trial 8 structure
Primarysurgery
Randomize
Anastrozole (3 years)
Switching period
Sequencing periodJakesz R et al. Lancet 2005
Switch point
Tamoxifen
(2 years)
Tamoxifen(3 years)
Tamoxifen
(2 years)

3013063-13
Event-free survival following adjuvant therapy switch (n = 2529)
0
75
80
85
90
95
100
0 12 24 36 48 60 72
Time after switch (months)
EFS (%)
Anastrozole (A)Tamoxifen (T)
HR
0.62Events
p-value
0.011
T
69
A
44
Therapy switch(2 years after surgery)
92.8%
88.9%

3013063-14
ABCSG Trial 8 structure
Primarysurgery
Randomize
Anastrozole (3 years)
Switching period
Sequencing periodJakesz R et al. Lancet 2005
Switch point
Tamoxifen
(2 years)
Tamoxifen(3 years)
Tamoxifen
(2 years)

3013063-15
Arm A: Tamoxifen for 5 years (n=67 cases)
Risk relative toextensive metabolizers P value
CYP2D6 PM 3.83 (1.27-11.55) 0.017
CYP2D6 IM 0.87 (0.44-1.71) 0.689
CP1229323-18
Arm B: Tamoxifen to anastrozole (n=55 cases)
Risk relative to extensive metabolizers P value
CYP2D6 PM 1.02 (0.21-4.83) 0.985
CYP2D6 IM 0.81 (0.40-1.61) 0.538
CYP2D6 and Relative Risk of Breast Event
Goetz et al. SABC 2008

3013063-16
Arm A: Tamoxifen Years 3-5 (n=55 cases)
Risk relative toextensive metabolizers P value
CYP2D6 PM 2.81 (0.88-8.97) 0.081
CYP2D6 IM 0.75 (0.36-1.55) 0.431
CP1229323-18
Arm B: Anastrozole Years 3-5 (n=31 cases)
CYP2D6 and Relative Risk of Breast Event
Risk relative toextensive metabolizers P value
CYP2D6 PM 0.71 (0.06-8.39) 0.782
CYP2D6 IM 0.57 (0.21-1.54) 0.269
Goetz et al. SABC 2008

3013063-17
Mayo Clinic Rochester: Treatment of Postmenopausal, ER + Breast Cancer
Women should be informed 1) data in support of CYP2D6 as key
enzyme involved in the activation of tamoxifen
2) Discontinuation of potent CYP2D6 inhibitors
3) CYP2D6 genotyping: CYP2D6 PM do not receive tamoxifen

3013063-18
New identified Mechanism of Action (Endoxifen)
• Does endoxifen differ from Tamoxifen or 4-HT in its interaction with the estrogen receptor?

3013063-19
Tamoxifen Mechanism of Action
ER
ER
ERER
ER
SRC
D1
Coregulators
Transcription
GeneERE
Tamoxifen

3013063-20
Endoxifen but not 4HT Results in Increased ERα Protein Turnover
Wu et al: Cancer Res, 2009

3013063-21Jin Y et al: J Natl Cancer Inst 97:30, 2005
Tamoxifen Metabolic Pathway (Humans)
CP1230355-21
400-600 nM
5-10 nM
20-180 nM
200-300 nM
Binding affinity relative to estradiol
1.00 for metabolites 4-OH TAM and endoxifen 0.01 for tamoxifen and N-desmethyl tamoxifen

3013063-22
High Concentrations of EndoxifenSuppress MCF-7 Cell Proliferation at Clinically
Relevant Conditions
Wu et al: Cancer Res, 2009
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
Re
lati
ve
fo
ld c
ha
ng
efr
om
ve
hic
le
Vehicle E2 E2+com-
bination(TAM+4HT
+NDT)
E2++20 nM
endoxifen
E2+com-
bination+40 nM
endoxifen
E2+com-
bination+100 nM
endoxifen
E2+com-
bination+1,000 nMendoxifen

3013063-23
True Personalized Medicine: You need to account for all sources of
variation: germ line, tumor, environmental

3013063-24
van't Veer LJ et al: J Clin Oncol 23:1631, 2005van't Veer LJ et al: J Clin Oncol 23:1631, 2005
Gene Expression Profiling
Unfixed sample of tumor tissueUnfixed sample of tumor tissue
Surgical removal of tumor tissue
Surgical removal of tumor tissue
Labeled tumor cDNA or cRNALabeled tumor cDNA or cRNA
Tumor RNATumor RNA
Comparative analysis
of gene expression
Molecular signatureMolecular signature
Poor Poor prognosisprognosis
Good Good prognosisprognosis
Labeled control cDNA or cRNA
Labeled control cDNA or cRNA
DNA microarray
DNA microarray

3013063-25
Sorlie et al: Proc Natl Acad Sci USA 100:8418, 2003Sorlie et al: Proc Natl Acad Sci USA 100:8418, 2003
Gene Expression ProfilingIdentifies Molecularly Distinct Subtypes
Gene Expression ProfilingIdentifies Molecularly Distinct Subtypes
AA BB
CC
DD
EE
FF

3013063-26
Overexpression of HER-2 in Human Breast Cancer Cells
Human breast cancer cells
Transfect withHER2 gene
DNA synthesisCell growthrateGrowth in soft agar
TumorigenicityMetastaticpotential
Transformed breast cancer cell
Multiple copies of HER2,
high expressor
Single copy of HER2,
low expressor

3013063-27
Tamoxifen Stimulates the in Vivo Growth ofHER-2 Expressing, ER+ Xenographs
Shou J et al:J Natl Cancer Inst 96:926, 2004
P-MAPKTHr202/Tyr204)
T-MAPK
E2 TAM -E2
1 9030 60
Tumorvolume(mm3)
Days
1,400
1,000
200
0
600
-E2
TAME2

3013063-28
Tamoxifen, Endoxifen in MCF-7 HER2 expressing Breast Cancer Cells
MCF7-HER2
0
20
40
60
80
100
120
140
160
1 10 100 1000
Drug concentration (nM)
% o
f C
on
tro
l (D
MS
O o
nly
)
TAM
END
Goetz, Reinicke, Ames et al. unpublished

3013063-29
Tamoxifen versus Endoxifen in HER-2 positive cells
• Does CYP2D6 status (metabolic activation to endoxifen) impact the outcomes of patients with HER-2 positive breast cancer?

3013063-30
5 years oftamoxifen(20 mg qd)+ 1 year of
fluoxymesterone(10 mg po bid)
5 years oftamoxifen(20 mg qd)+ 1 year of
fluoxymesterone(10 mg po bid)
5 years of tamoxifen5 years of tamoxifen
NCCTG 89-30-52NCCTG 89-30-52
RRAANNDDOOMMIIZZAATTIIOONN
Postmenopausal women
Postmenopausal women
5 years total therapy5 years total therapy
541 women accrued
541 women accrued
Early ER+
breast cancerEarly ER+
breast cancer

3013063-31
HER-2, CYP2D6 and Recurrence Free-Survival
0
20
40
60
80
100
0 2 4 6 8 10 12 14
%%
Years from randomizationYears from randomization
EM/EM, EM/IMEM/PM, IM/IM, PM/IM, PM/PMP=0.006
EM/EM, EM/IMEM/PM, IM/IM, PM/IM, PM/PMP=0.006
n=9n=9
n=10n=10
CP1347559-1
PM alleles: *3, *4, *6IM alleles: *10, *17, *41Potent CYP2D6 inhibitor = PM/PM
PM alleles: *3, *4, *6IM alleles: *10, *17, *41Potent CYP2D6 inhibitor = PM/PM

3013063-32
Pharmacology 101
• Which tamoxifen molecule is occupying the estrogen receptor – tamoxifen, 4-hydroxy tamoxifen, endoxifen?
• Who cares?
• Pharmacology is boring – if the drug doesn’t work, just use a different drug

3013063-33
Summary
• The metabolic activation of tamoxifen precludes use for many women
• In HER2 expressing breast cancer, tamoxifen activates but endoxifen potently inhibits tumor growth
• Administration of endoxifen would bypass the genetic and concomitant drug effects on metabolism

3013063-34
Murine Endoxifen PlasmaConcentrations After PO Adminstration
1
10
100
1,000
10,000
0 240 480 720 960 1,200
En
do
xife
n (
nM
)E
nd
oxi
fen
(n
M)
MinutesMinutes
4 mg/kg4 mg/kg
200 mg/kg200 mg/kg
Reid, JR, Goetz, MP, Ames MM

3013063-35
• How do we develop Endoxifen?• No intellectual property, thus no
drug company interest• Can NCI facilitate the development
of endoxifen?
Next Steps

3013063-36
Endoxifen Drug Development Timeline
2009 2010 2010-2011 2012-2015
Precl
inic
al p
harm
acolo
gy
and to
xico
logy
in m
ice
NCI and M
ayo complete preclin
ical
Toxicology; clin
ical gra
de drug availa
ble
Phase II stu
dies begin
Human p
hase I stu
dy begin
s

3013063-37
Acknowledgments
Matthew Ames LabJoel Reid Katherine ReinickeStephanie SafgrenMary Kuffel Sarah Buhrow
James Ingle Vera J. Suman
Tom Spelsberg labJohn HawseXiaglin WuMalayannan Subramaniam
Richard Weinshilboum labAnn Moyer
OthersRobert JenkinsCarol Reynolds

3013063-38
• Mayo Clinic Cancer Center
• North Central Cancer Treatment Group
• ABCSG
• Mayo Clinic Cancer Center
• North Central Cancer Treatment Group
• ABCSG
• 1R01CA133049-01 (Goetz)
• Mayo Clinic Breast Cancer SPORE
• K-12 (Paul Calabresi Scholar)
• Pharmacogenetics Research Network (Dick Weinshilboum)