Embed Size (px)
Citation preview
Missed breast cancers How to manage…
Thierry Pousse
HANOI 2015
¨ Interval cancer: occured after mammography before next MMG 7,5/10000 to 22/10000 ¡ no abnormality/MMG even looking back ¡ False negative : missed detection or caracterisation
on prior MMG
172 lesions /427 MMG: visible but not specific Birdwell Ikeda al Radiology al 2001:219;192-202 2003;226:494-503
¨ False negative interval cancer ¨ False negative with very poor signal ¨ Occult cancers ¨ True interval cancer
¨ Conditions ¡ « double » blind ¡ among normal MMG (%? ) ¡ false positive (%?) ¡ Seniors or juniors (L1 ? L2?)
¨ Retrospective second look ¨ Difference between:
¡ K really visible but with non specific signs present ¡ K that could not be proved as pathologic
¨ Subtle lesions: architecture break, density asymetry
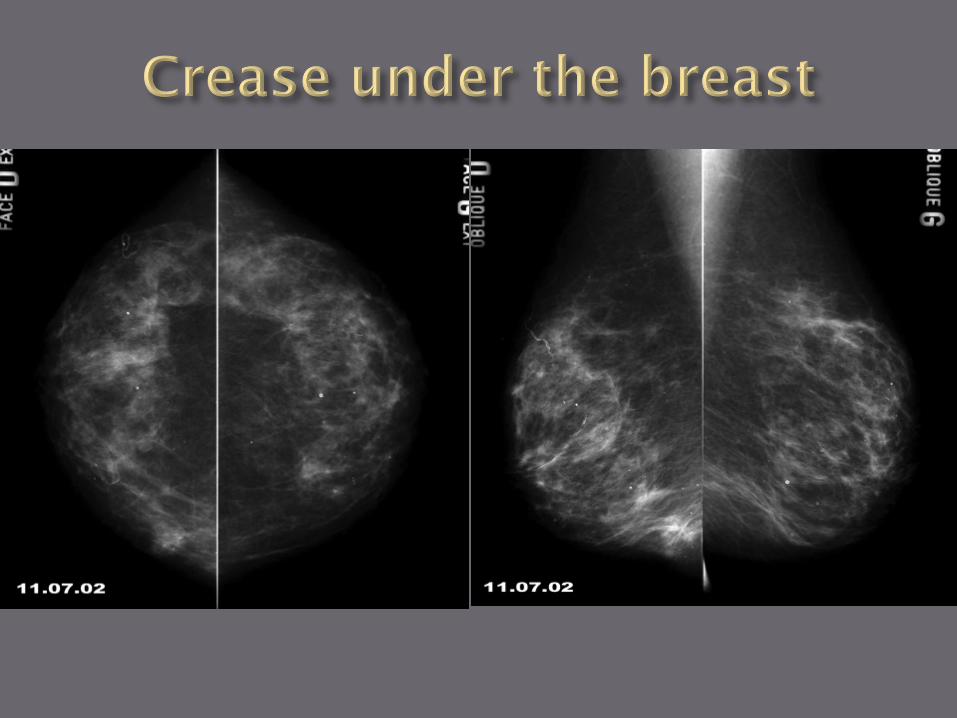
¨ Tricky spots: prepectoral, retrogland, retroareolar, crease under the breast
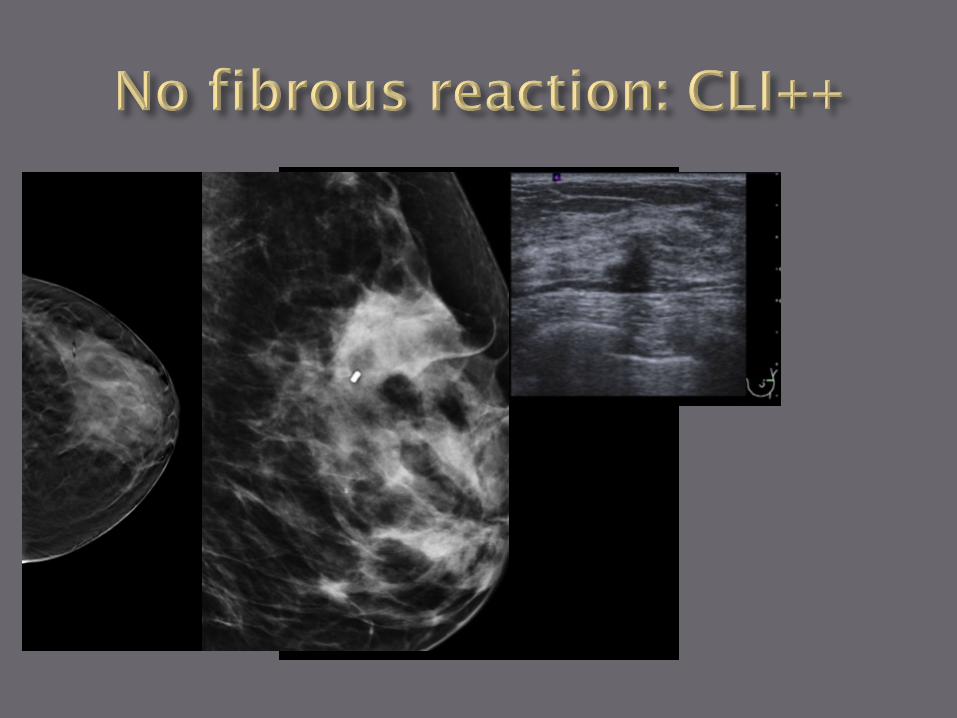
¨ Associated to evident lesion ¨ No stroma reaction or fibrous retraction
« Le seuil pour décider….est guidé par l’expérience et ne répond à aucune règle absolue. La seule certitude est qu’il faut compléter les investigations jusqu’à ce que l’on ait obtenu un degré de certitude suffisant » J Stinès. Les cancers du sein: les images visibles sur une seule incidence. J Radiol 2004; 85: 2083-94
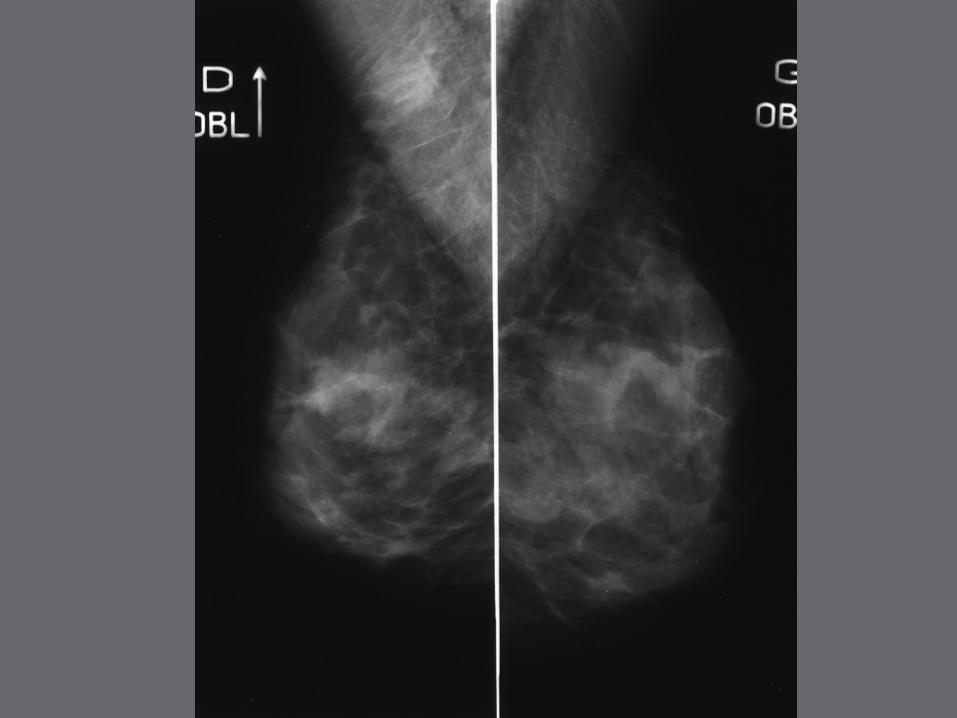
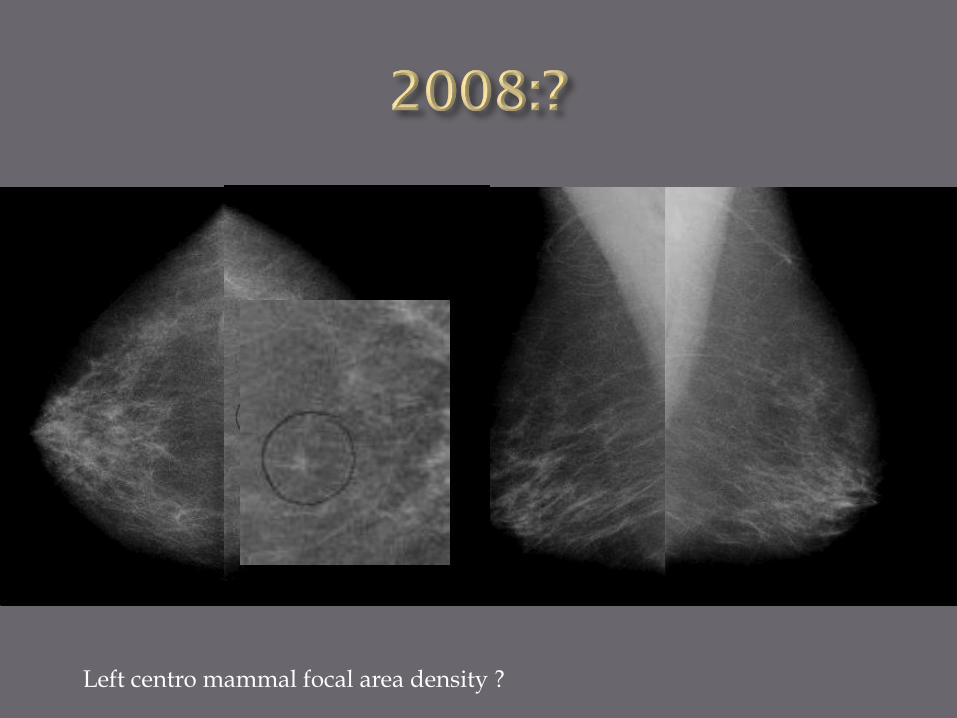
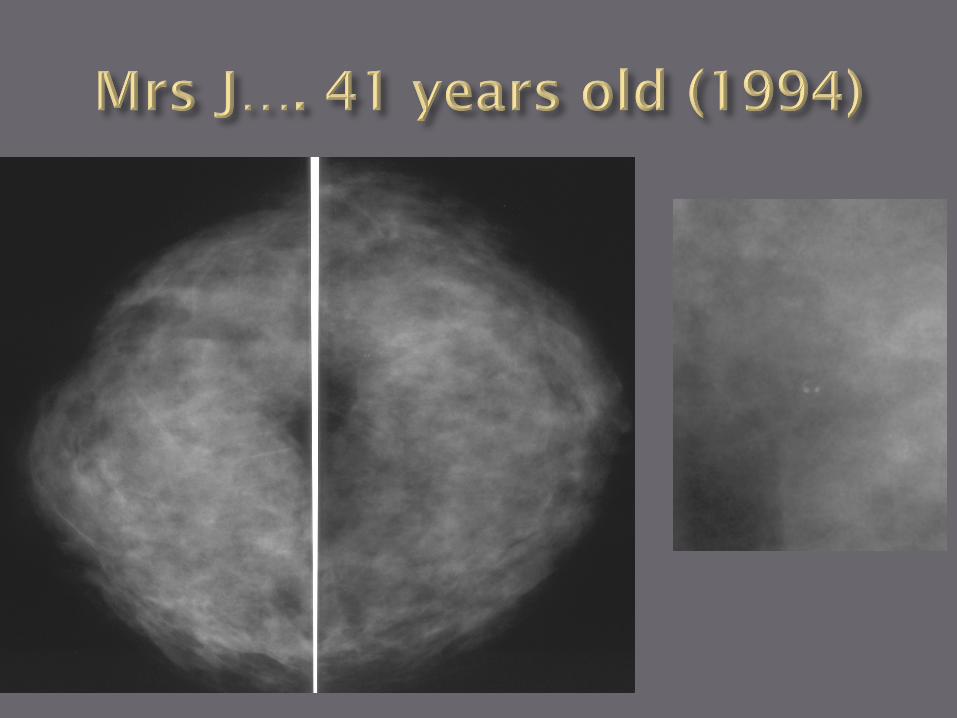
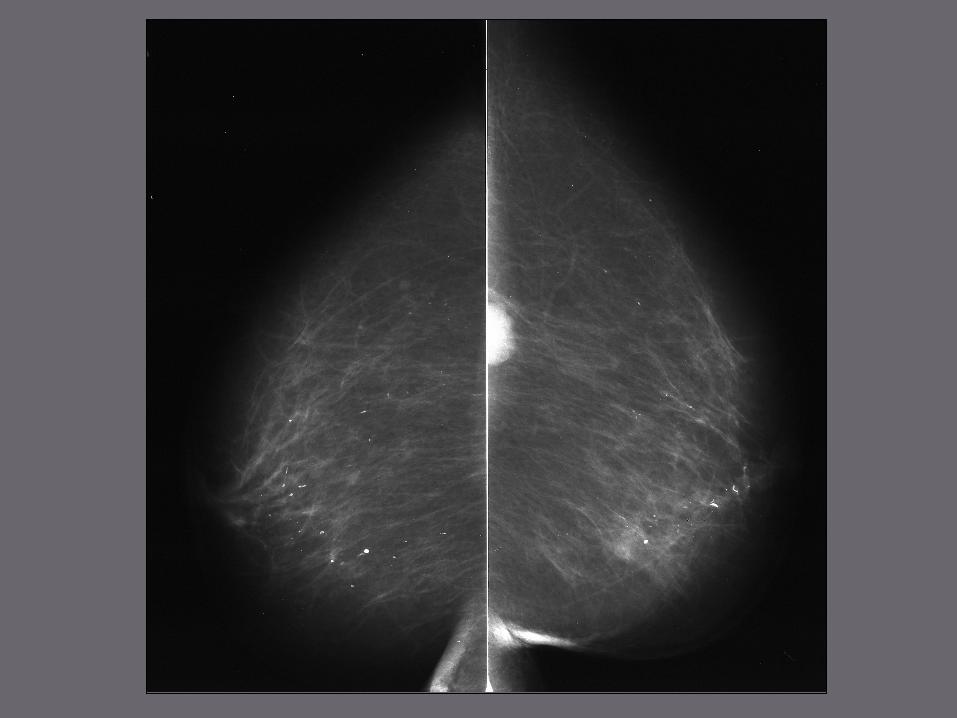
Left centro mammal focal area density ?
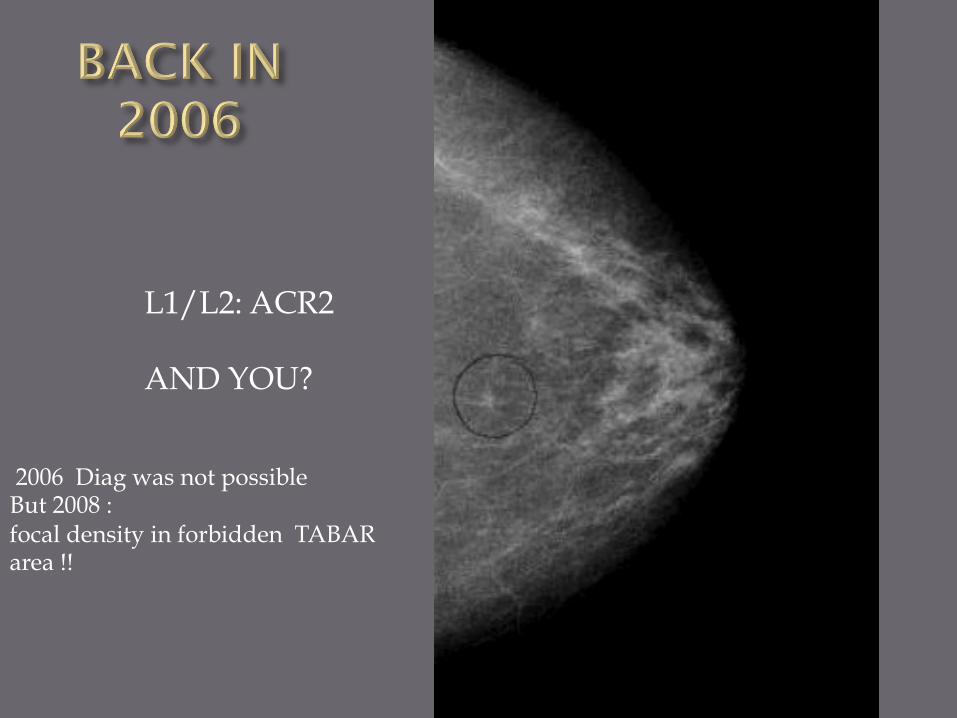
L1/L2: ACR2 AND YOU?
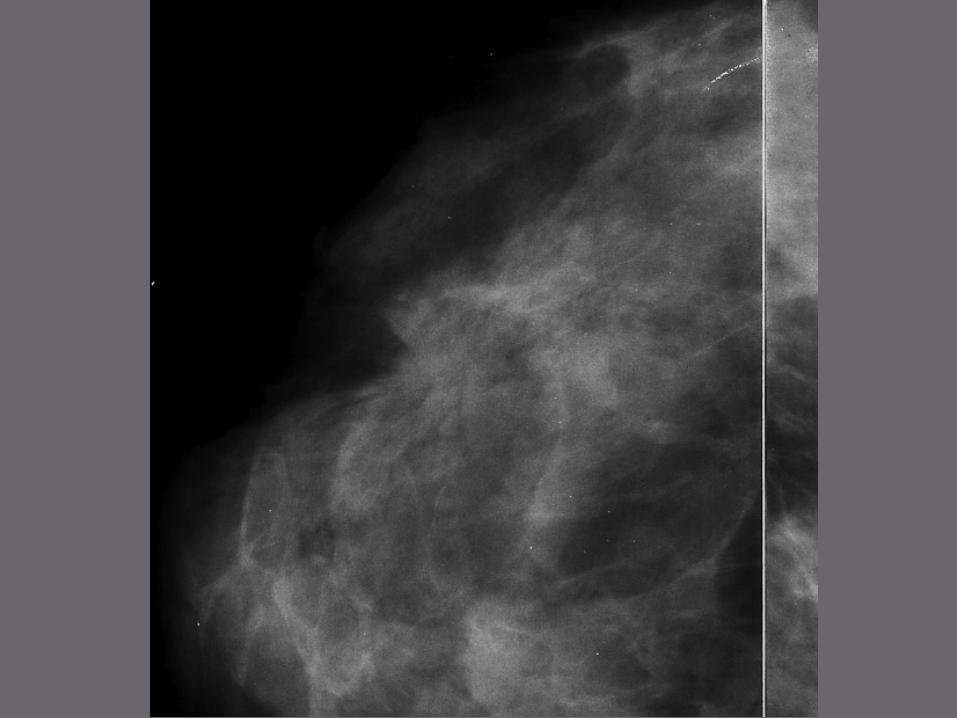
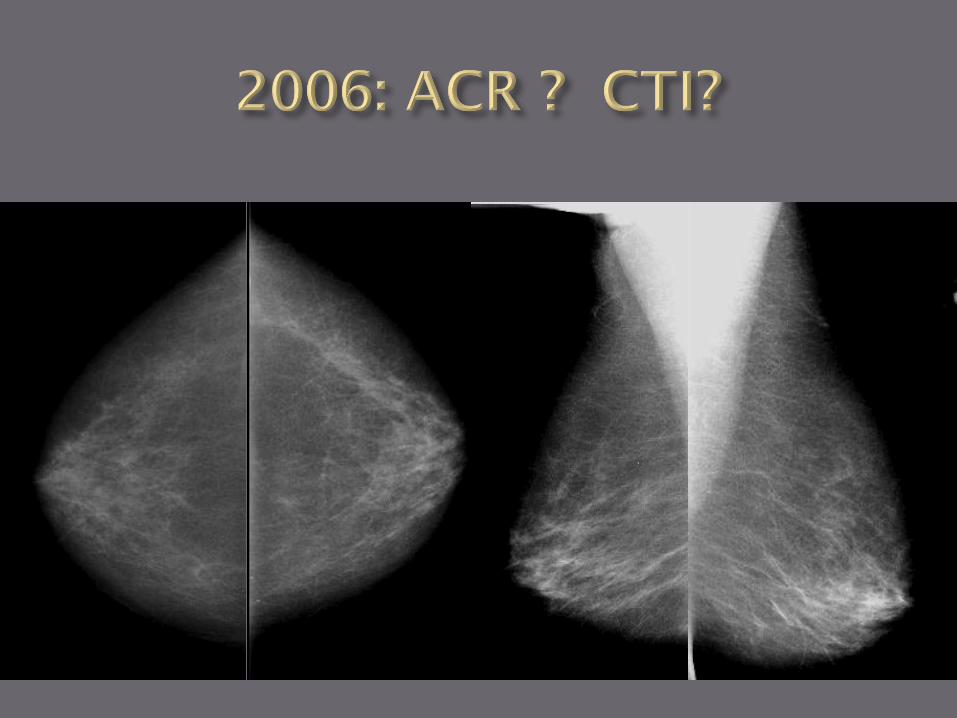
2006 Diag was not possible But 2008 : focal density in forbidden TABAR area !!
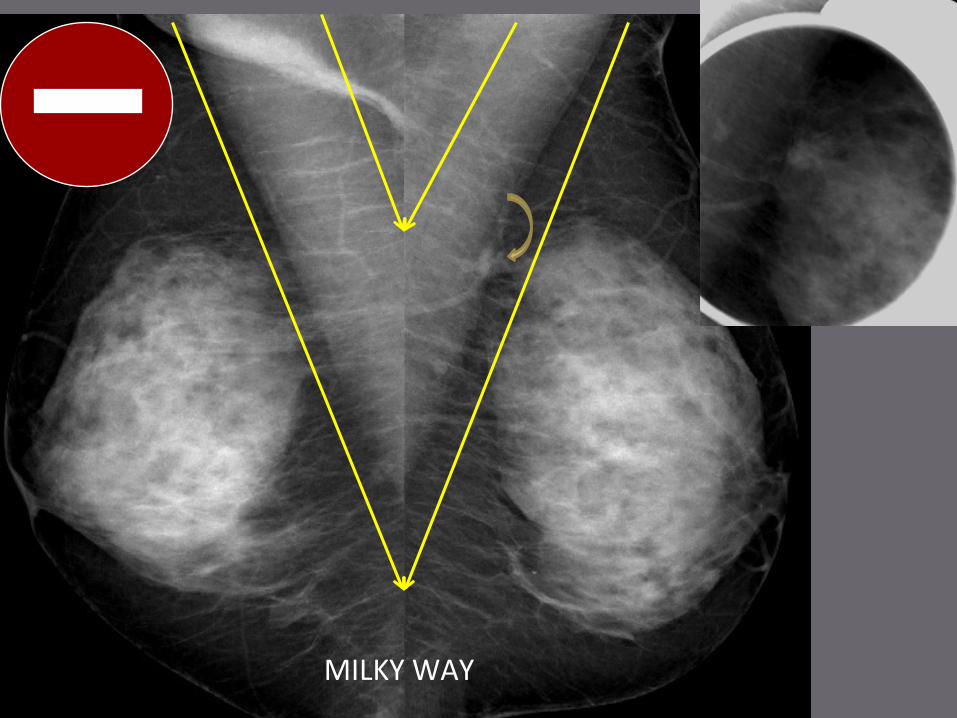
MILKYWAY
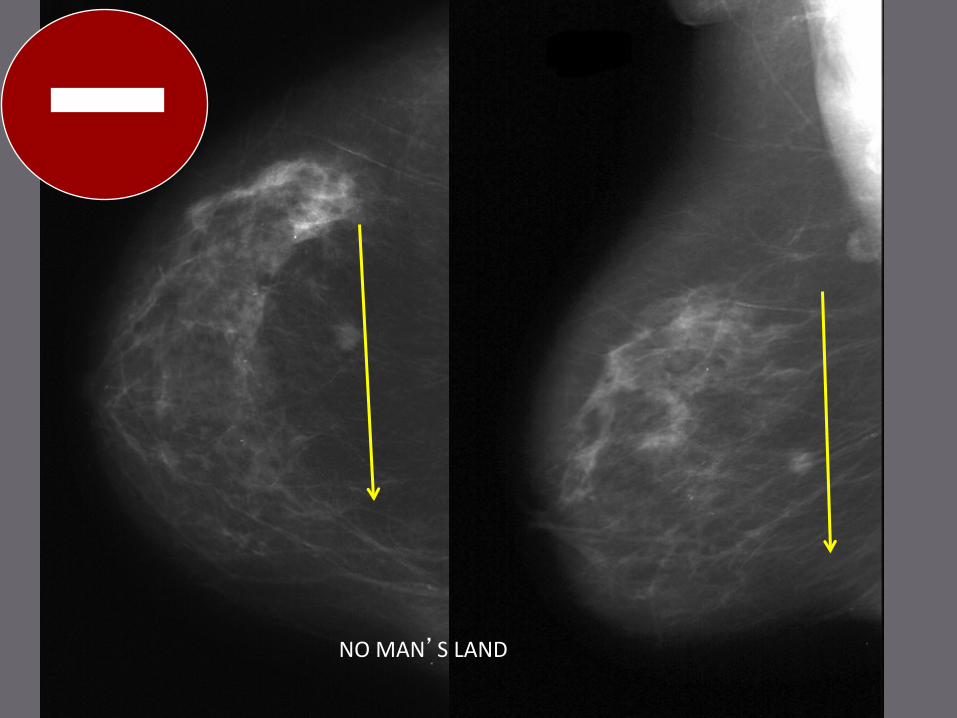
NOMAN’SLAND
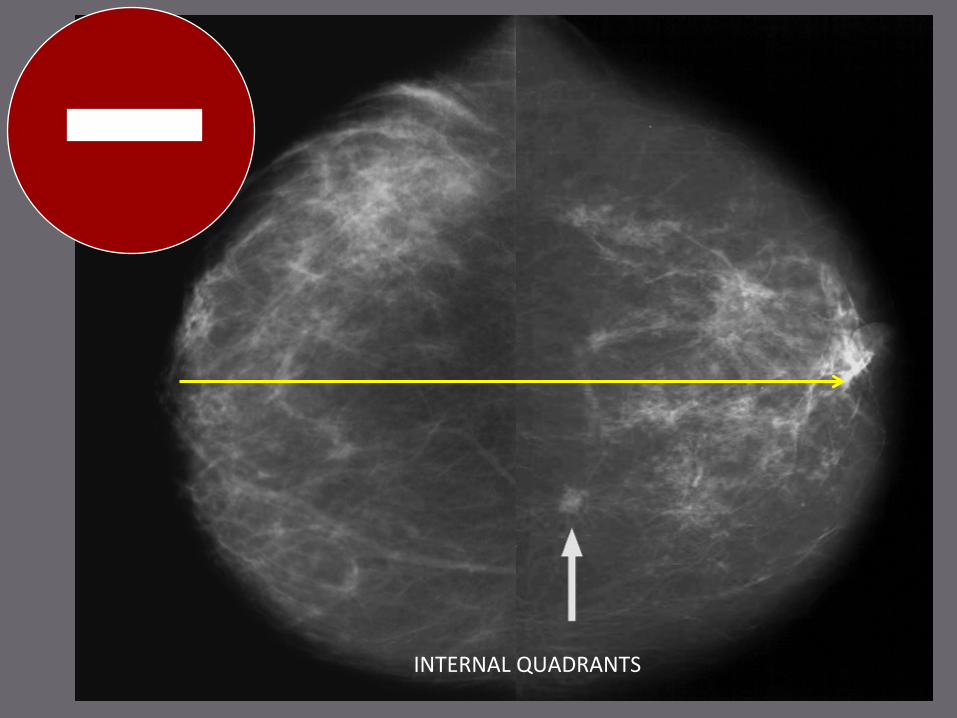
INTERNALQUADRANTS
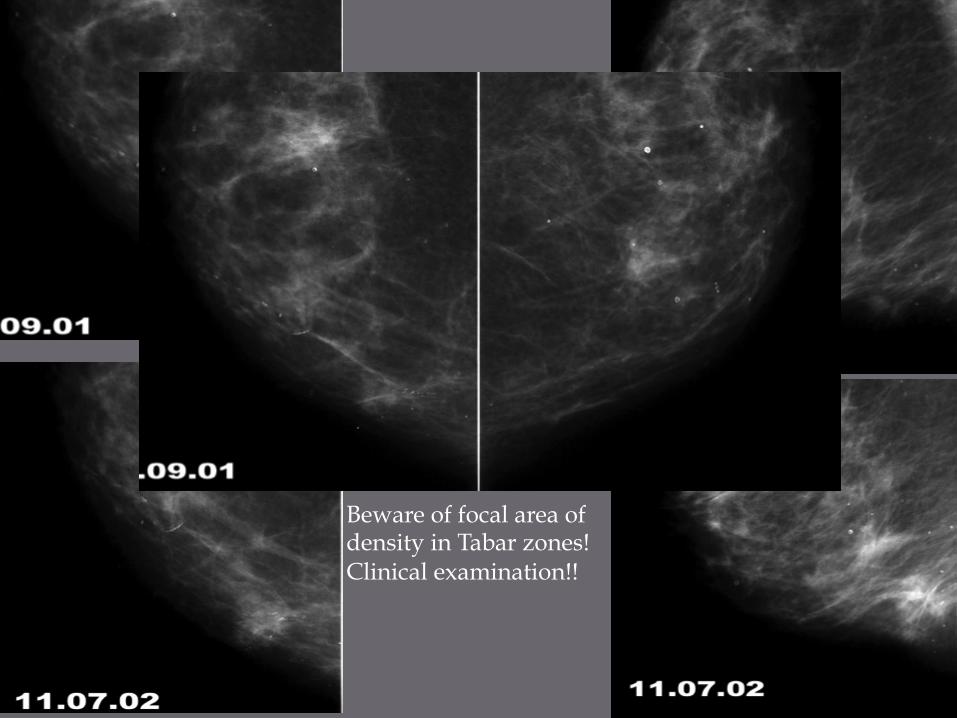
Beware of focal area of density in Tabar zones! Clinical examination!!
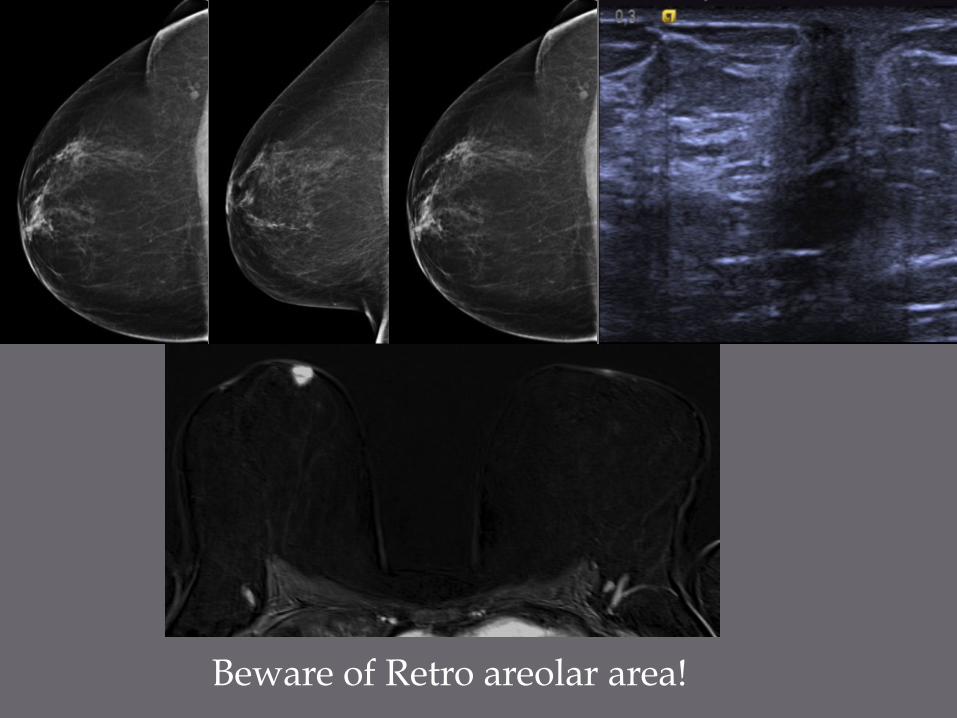
Beware of Retro areolar area!
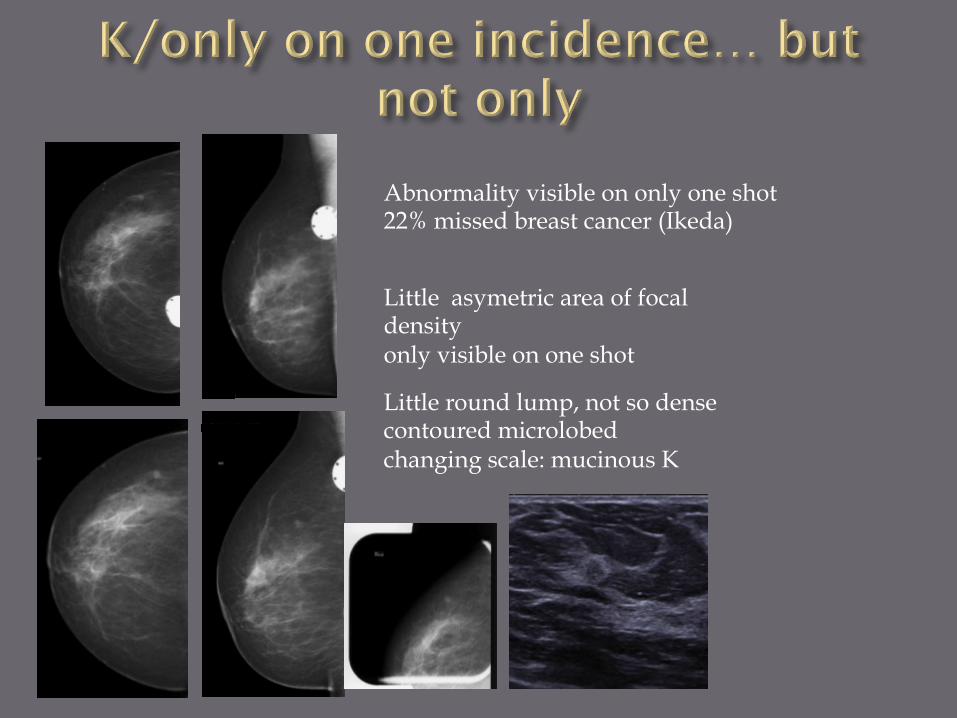
Little asymetric area of focal density only visible on one shot
Little round lump, not so dense contoured microlobed changing scale: mucinous K
Abnormality visible on only one shot 22% missed breast cancer (Ikeda)
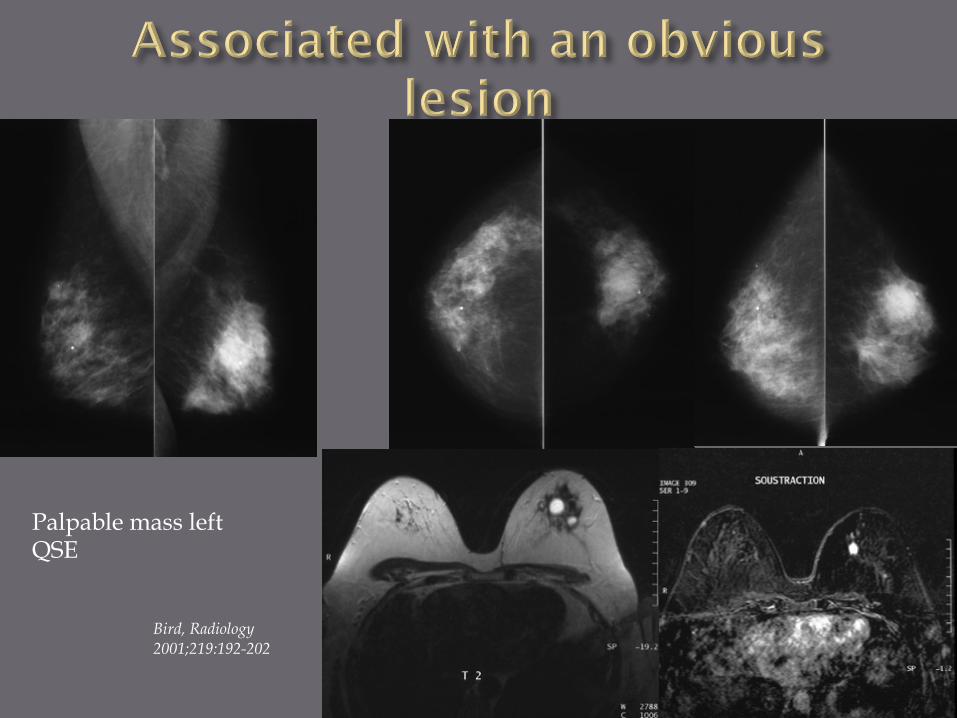
Palpable mass left QSE
Bird, Radiology 2001;219:192-202
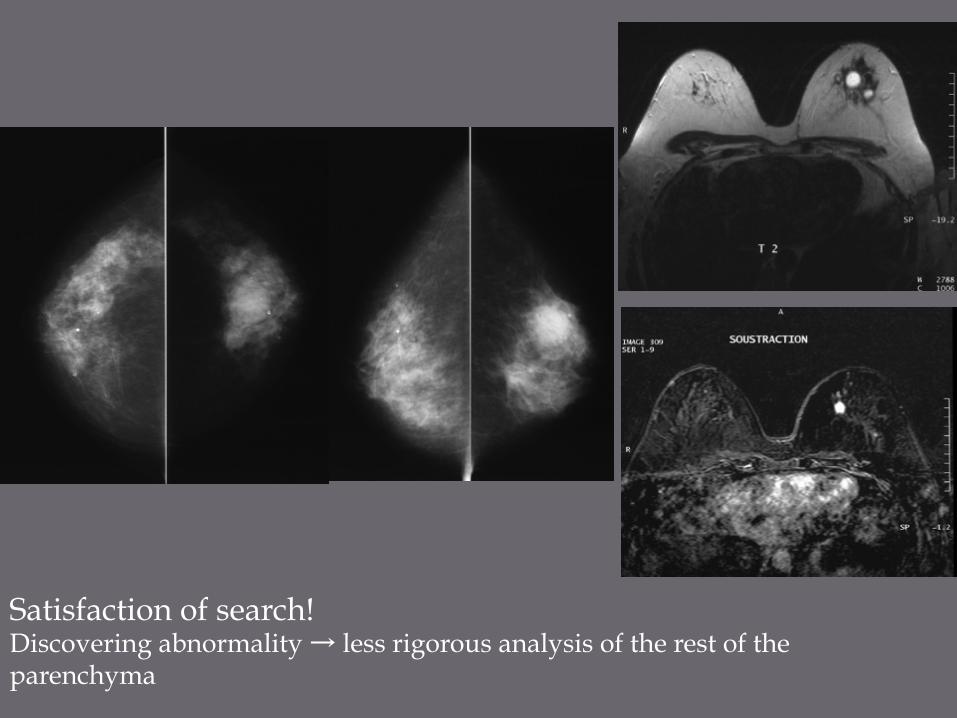
Satisfaction of search! Discovering abnormality → less rigorous analysis of the rest of the parenchyma

¨ unchanged lesions - microcalcifications→ 63 months LevToaf Radiology 1994
- lumps → 54 months Meyer AJR 1981
¨ Opacity benin-like 5% tumors → 6.3 years Vx2 according to Weedon Fekiger Breast Cancer Research 2008
¨ Microcalcifications benin-like
¨ Cluster of benin microcalcifications will change ¨ 25% cluster of malignant microcalcifications
stable between 6-60 months ¨ 9% microcalcifications stable 2 years CCIS high
grade Lev Toaf Radiology 1994

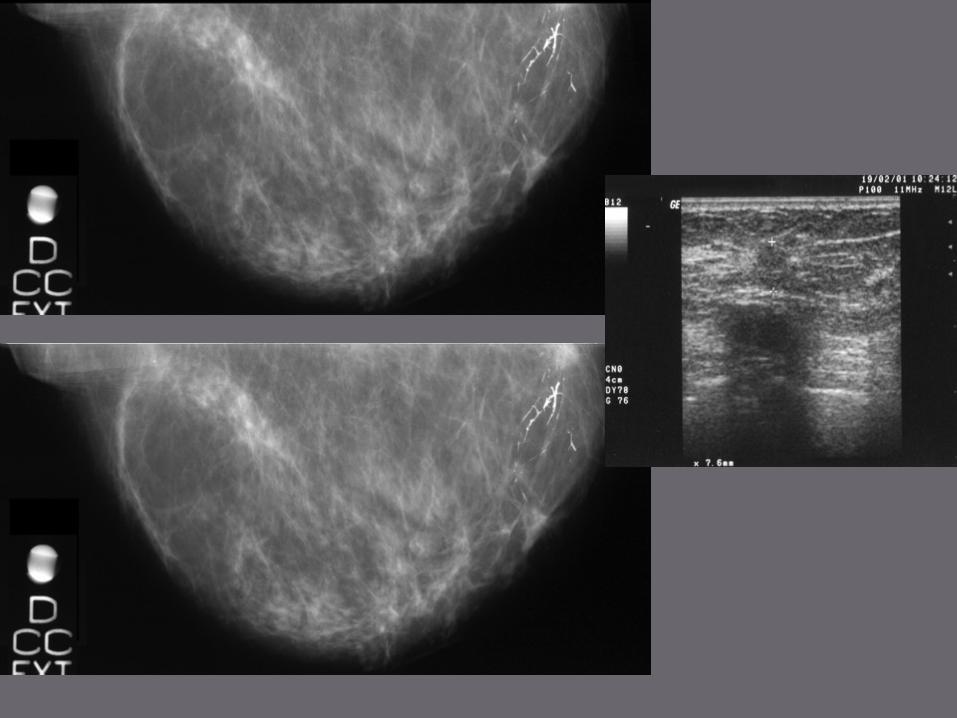
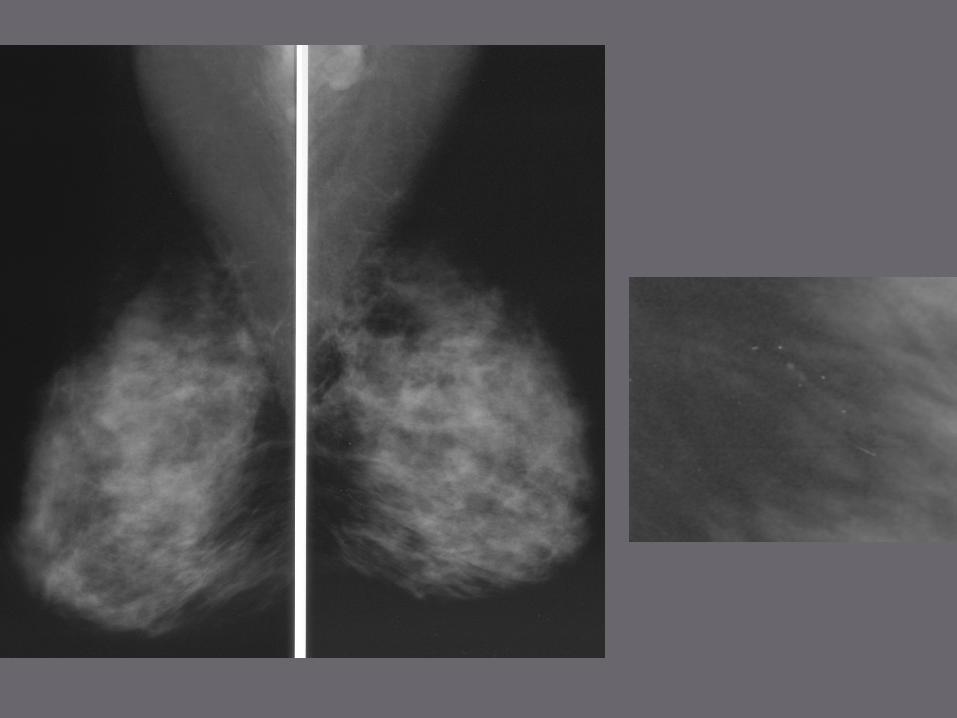
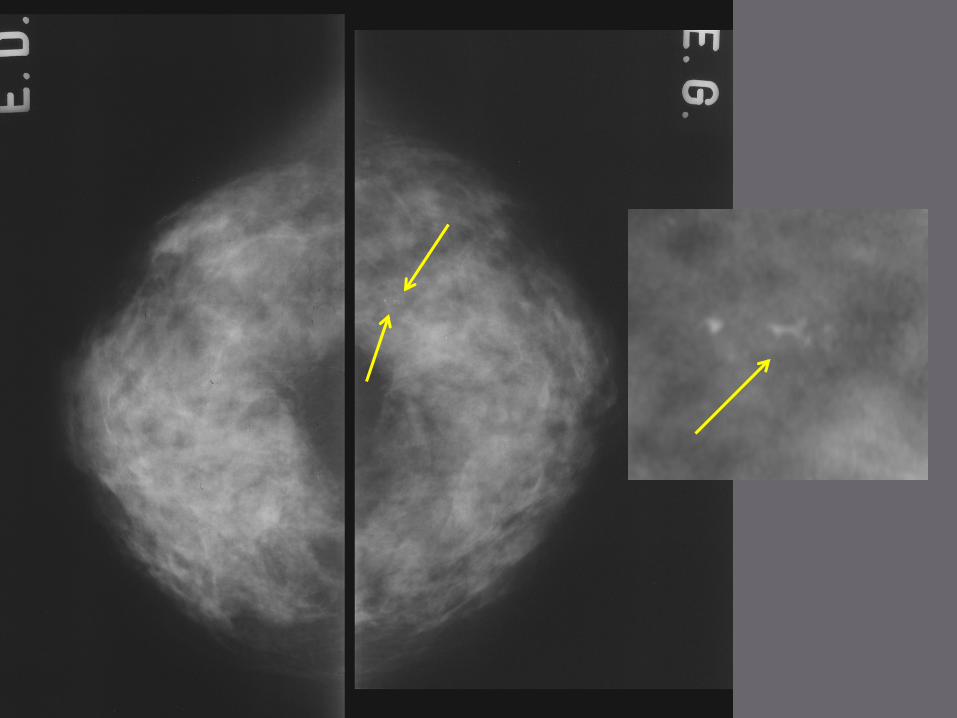
Sparse linear microcalcifications / one shot only Incomplete record Miscaracterisation : ACR 2
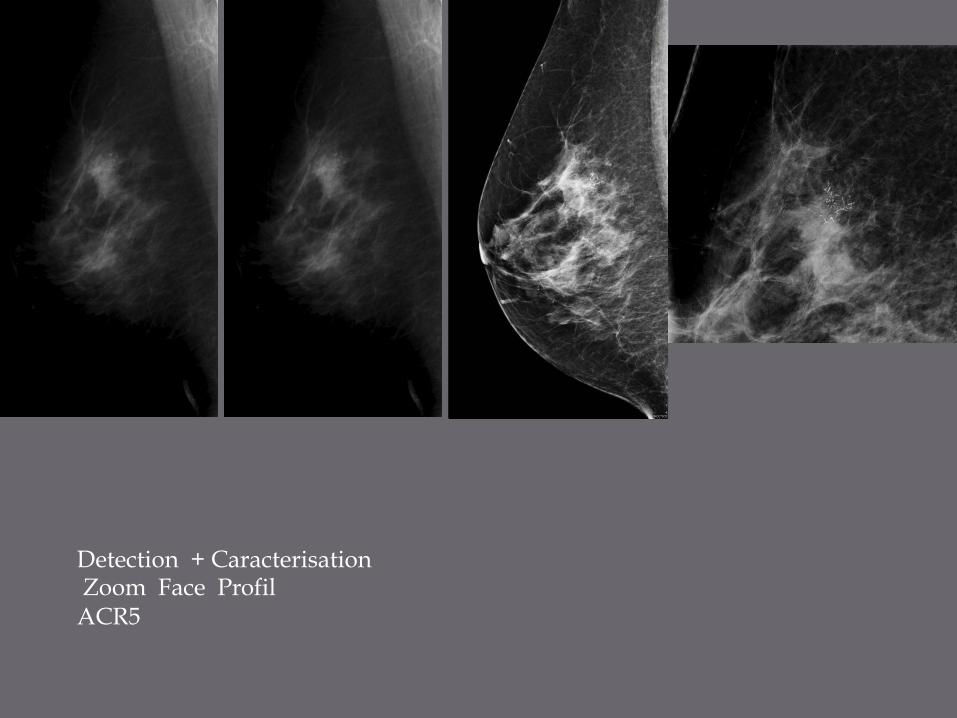
Detection + Caracterisation Zoom Face Profil ACR5
¨ Benin like microcalcifications ¨ Heterogeneous distribution of fibroconjonctive
tissue
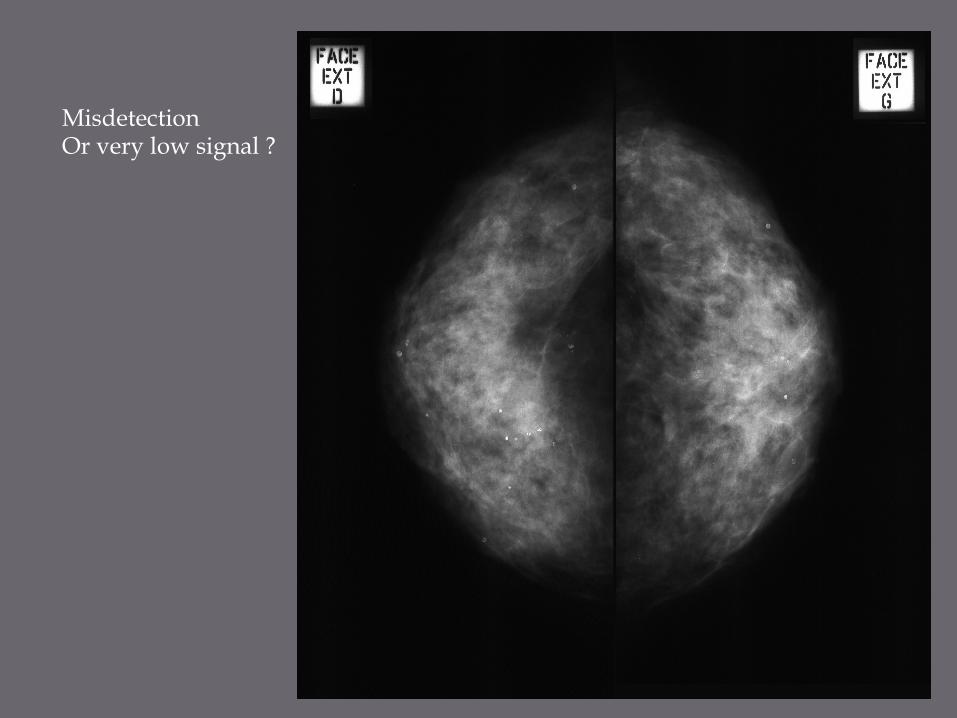
Misdetection Or very low signal ?
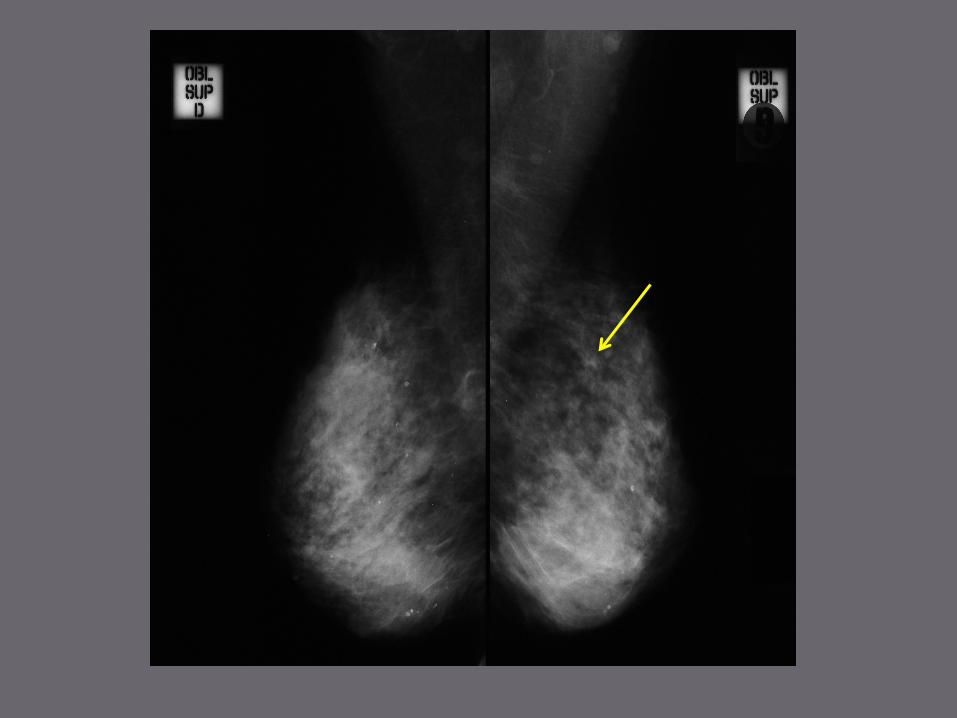
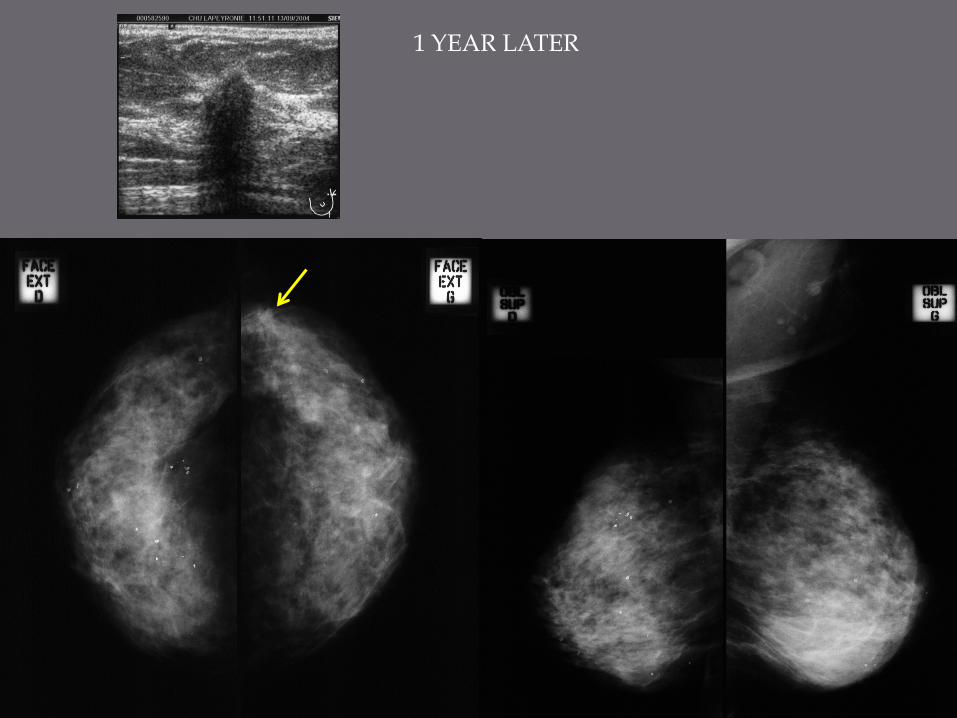
1 YEAR LATER
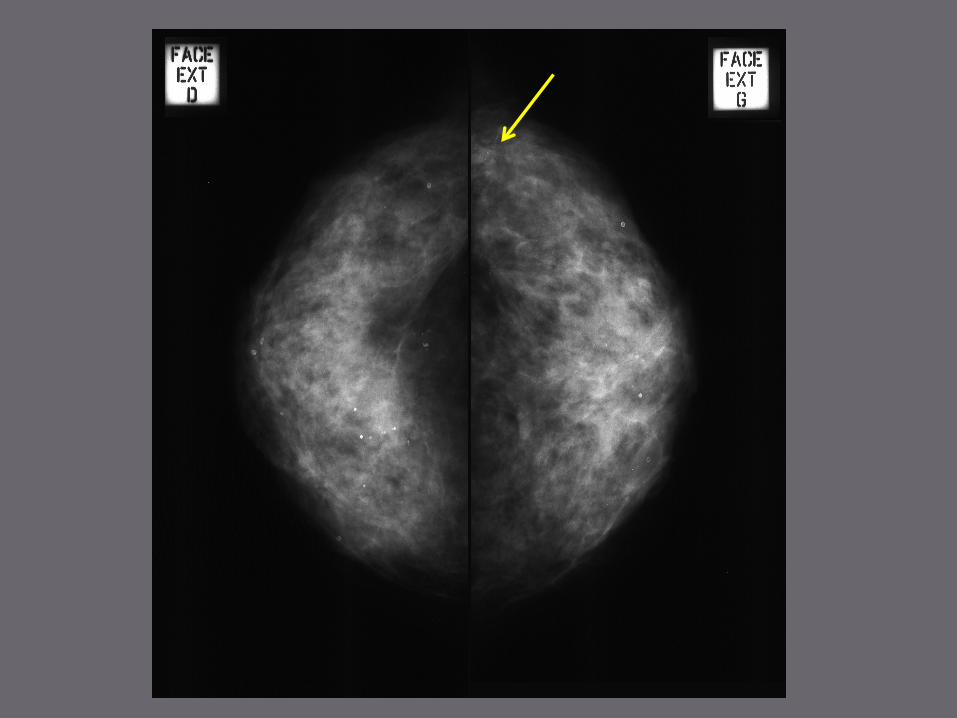
¨ K non visible/ MMG when diagnostic done even looking back ¡ Clinical examination+++ ¡ Causes conventionnally cited
ú Density of breast tissue ú Size and topography of the lesion ú Presence of CLI Incidence * 5%K SIM study **7% k retrospective study 1757 K ***24% high risk cancer patients *SIM Study CHU Lapeyronnie Montpellier¨Pr TAOUREL 2010
**Foxcroft LM and al. Breast cancers invisible on mammography. Aust N Z J Surg 2000 ; 70 : 162-7. ***Morris EA and al. MRI of occult breast carcinoma in a high-risk population. AJR 2003 ; 181 : 619-26
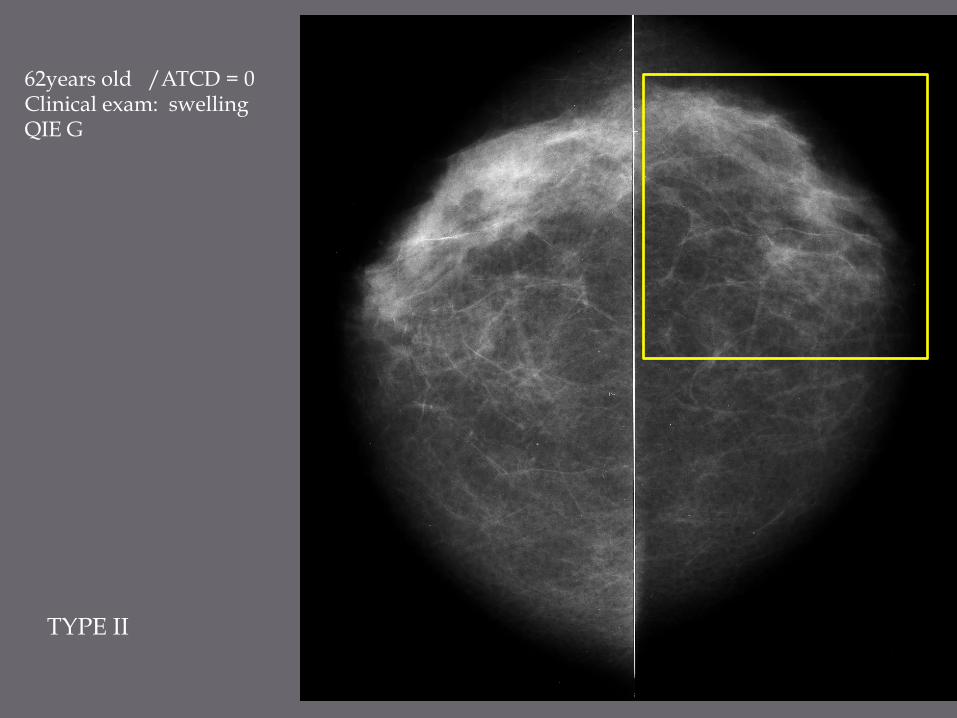
62years old /ATCD = 0 Clinical exam: swelling QIE G
TYPE II
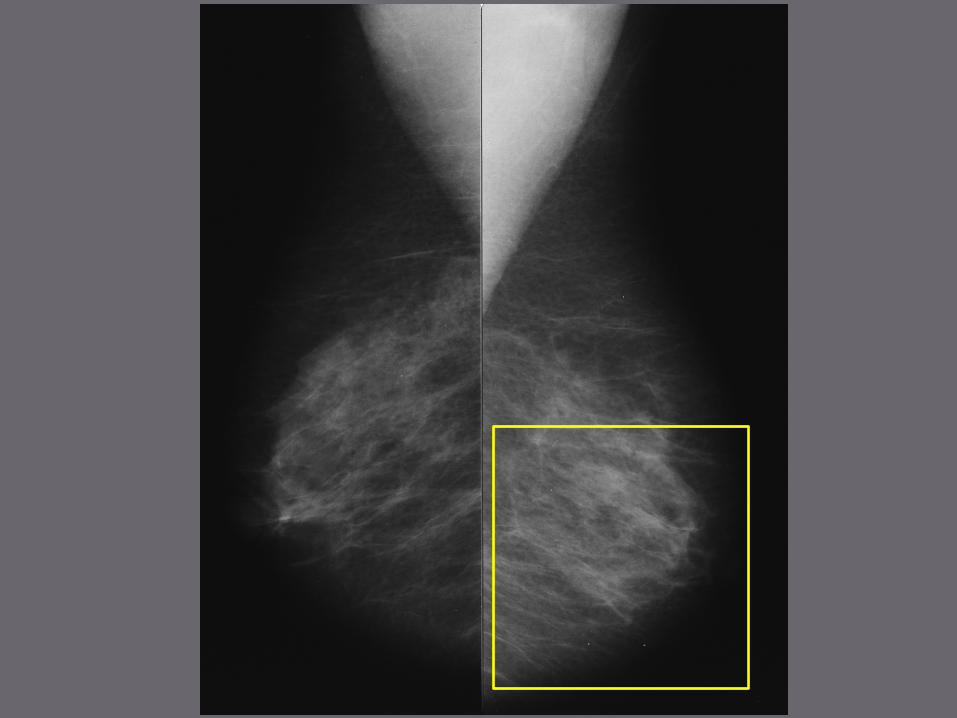
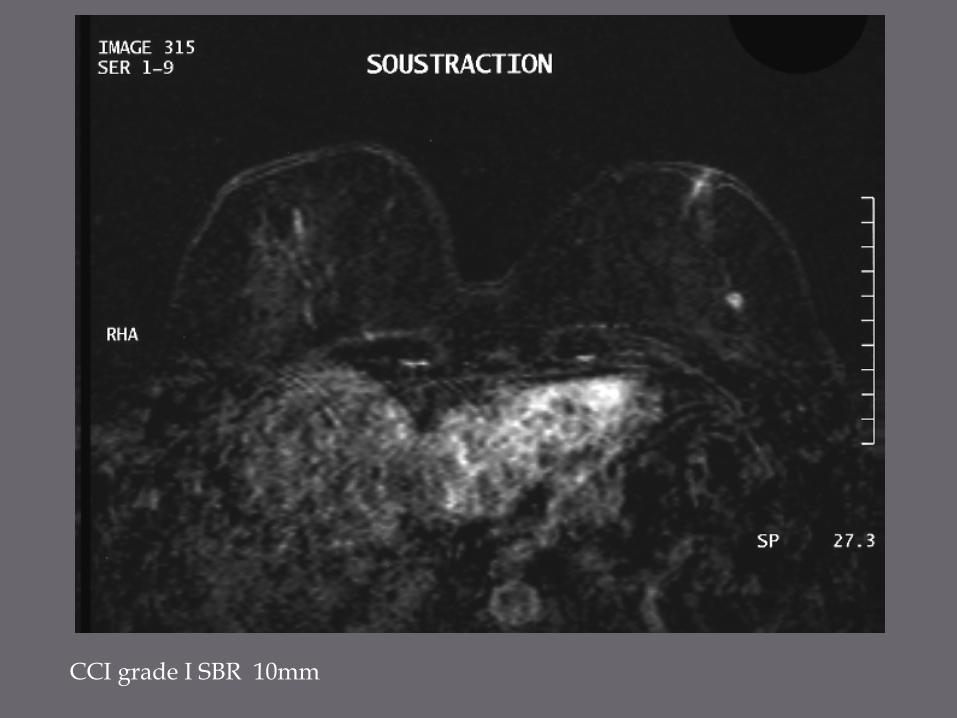
CCI grade I SBR 10mm
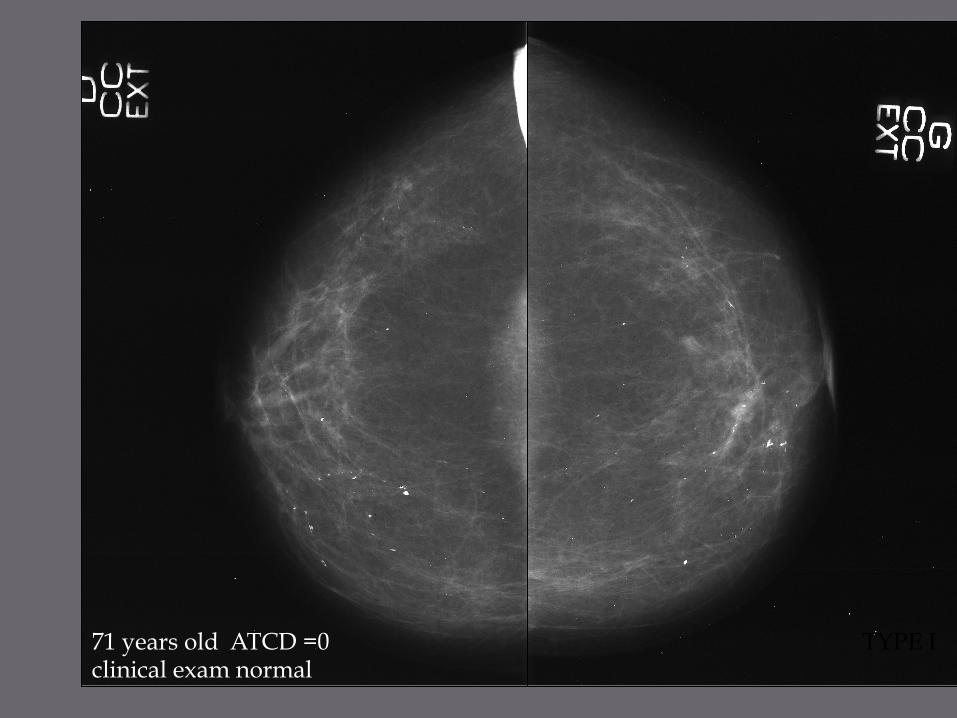
71 years old ATCD =0 clinical exam normal
TYPE I

Colloidal carcinoma SBRII 22mm
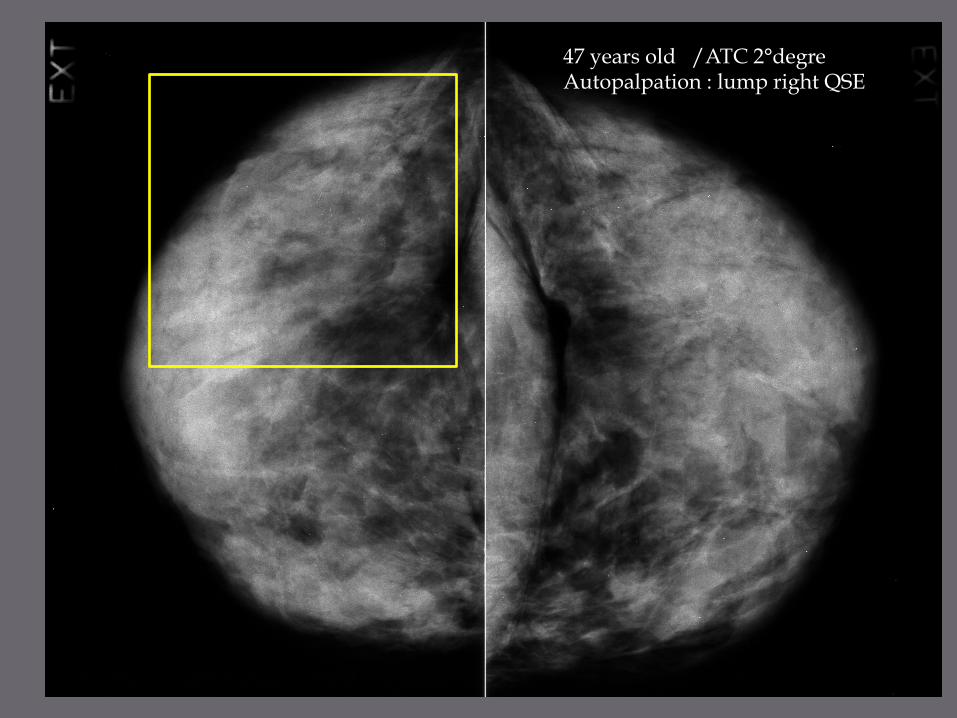
47 years old /ATC 2°degre Autopalpation : lump right QSE
TYPE IV
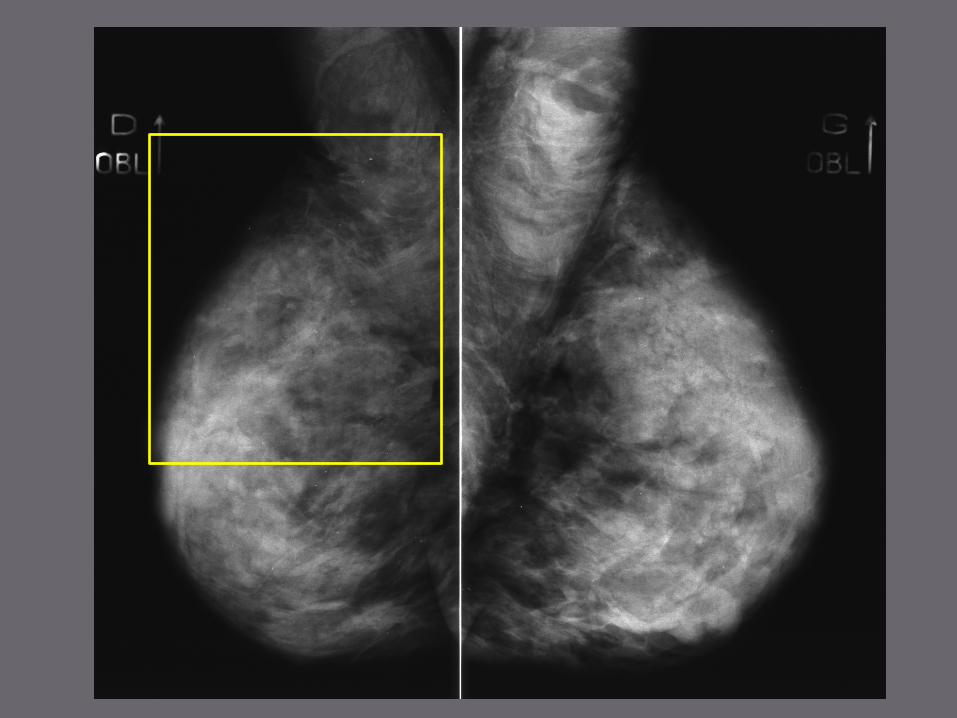
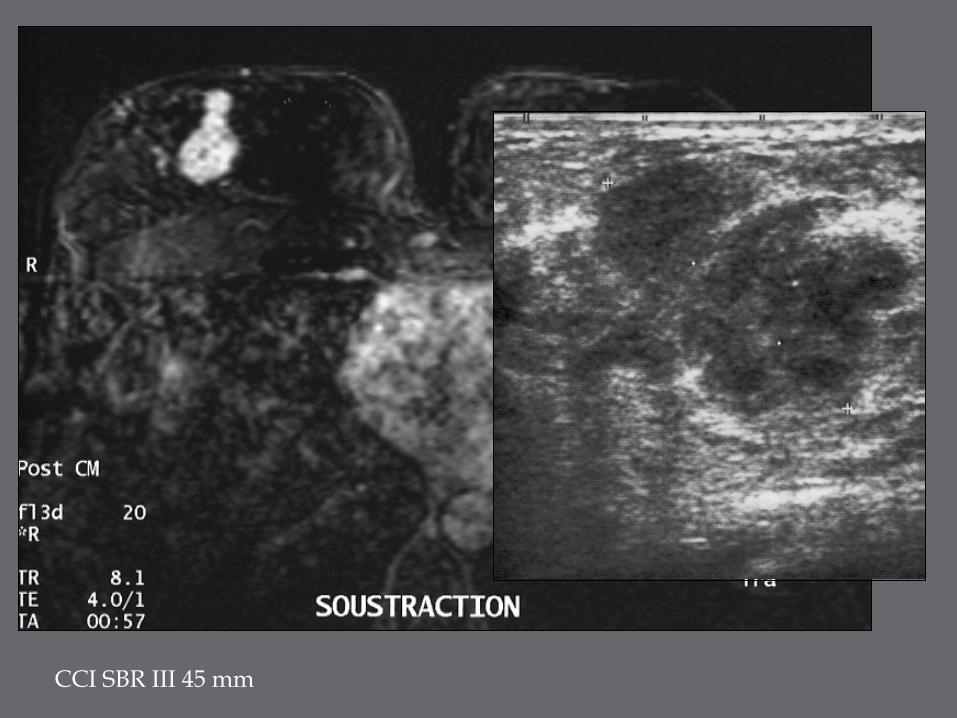
CCI SBR III 45 mm
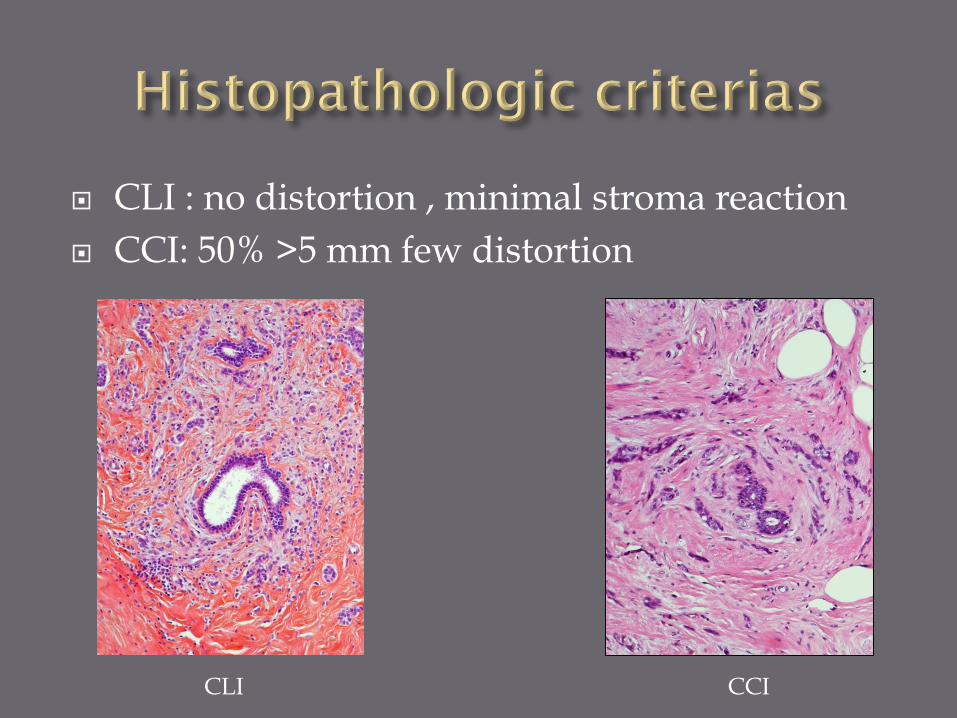
¨ CLI : no distortion , minimal stroma reaction ¨ CCI: 50% >5 mm few distortion
CLI CCI
¨ MMG negative even looking backyard but MMG positive when diagnosis is done
¨ K +/ MMG but non visible and K developped between 2 MMG
¨ K developed between 2 MMG ¡ Young women ¡ % CLI ¡ SBR ¡ Biological index tumoral proliferation ¡ RH -
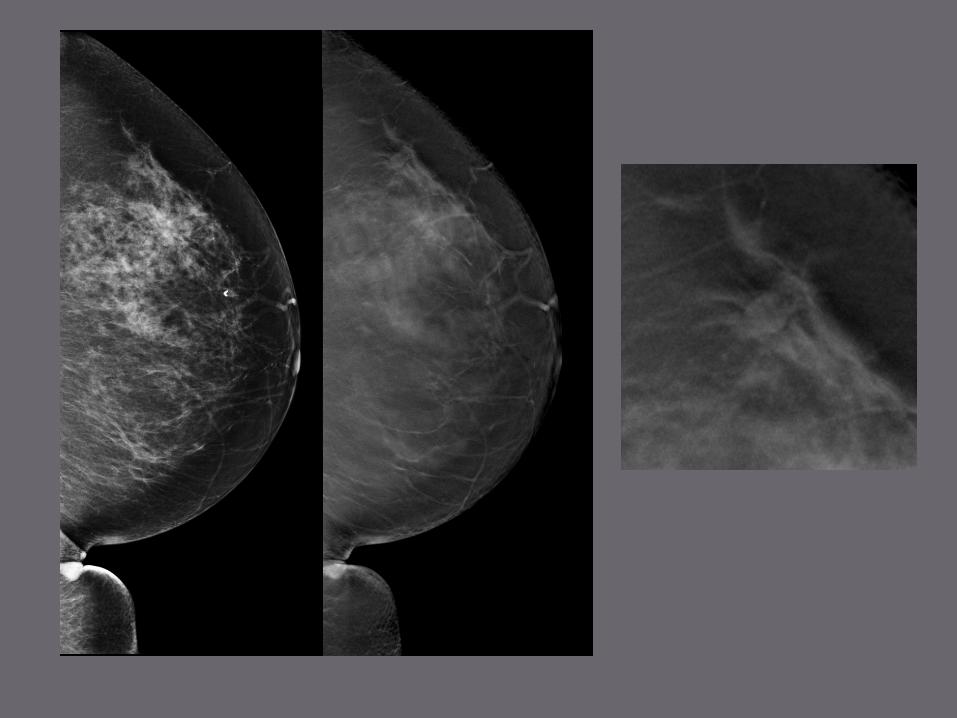
DIGITAL MAMMOGRAPHY TOMOSYNTHESIS
¨ Contrast resolution ¡ Microcalcifications ¡ < 50 years old ¡ breast density - Pisano NEJM 2005
¡ Architecture break Hambly AJR 2009
¨ Second line /selected patients ACR 0,3,4,5 ¡ true lesion ¡ caracterisation architecture break ,
masse, microcalcifications
¨ Breast cancer screening program
¨ Consecutive serie 158 patients recalled after MMG/ bresast cancer screening program(recall rate 6.6%-2.4%) screening program conditions
¨ 21K:13% ¨ 137 negative ¨ TS performance
¡ 0 FN ¡ Negative 102/137 - : 75%
¨ It works for BIRADS 1-2 and BIRADS 3-4 Breast Cancer Res Treatment 2012, projet TOMMY
¨ Single institutionnal retrospective reader study ¨ Data enriched- increasing number combination
of FFDM and DBT of cases BIRADS 3 ¨ Study including combination of FFDM and
DBT images
Radiology:volume276;number1_july2015-65-72
¨ The availability of prior FFDM and DBT images during interpretation is a largely independent contributing factor leading to a reduction in the frequency of recommandations to recall a woman without cancer for diagnostic work up
¨ The avaibility of DBT had a larger effect on radiologists performance levels than did the avaibility of prior FFDM images
¨ Publication and analysis of norwegian study ¨ Quality control ¨ 2D reconstruction from the 3D acquisition ¨ Diffusion of the technique to other companies ¨ Creativity of scientific community
¨ Frequency ¨ Mistakes : detection , caracterisation ¨ Performance improvement ¨ Technical parameters ¨ Subtles images ¨ Conditions of reading mammography ¨ CAD, Second reading
Majid AS, de Paredes ES, Doherty RD et al. Missed breast carcinomas: pitfalls and peals. Radiographics 2003;23:881-95
« For a lawyer, lawsuits are a way of life.For a physician, it strikes at the core of our being Kopans D. Mammography screening is saving thousands of lives, but will it survive medical malpractice? Radiology 2004; 230: 20-4
Cent choses entendues ne valent pas une chose vue. (Trăm điều nghe không bằng một điều thấy)
Cette présentation n aurait pas été possible sans l’aide de Dr Martine BOISSERIE LACROIX Fondation Bergonié BORDEAUX Dr Luc CEUGNART Fondation O . Lambret LILLE Pr Patrice TAOUREL CHU Lapeyronnie MONTPELLIER





























