Embed Size (px)
Citation preview
-HARSHA YADAV CT
MANAGEMENT OF INTESTINAL
OBSTRUCTION
ACUTE INTESTINAL OBSTRUCTION
It involves-
Supportive Management.
Surgical Management.
SUPPORTIVE
MANAGEMENT:
Nasogastric
Decompression.
Fluid and Electrolyte
replacement.
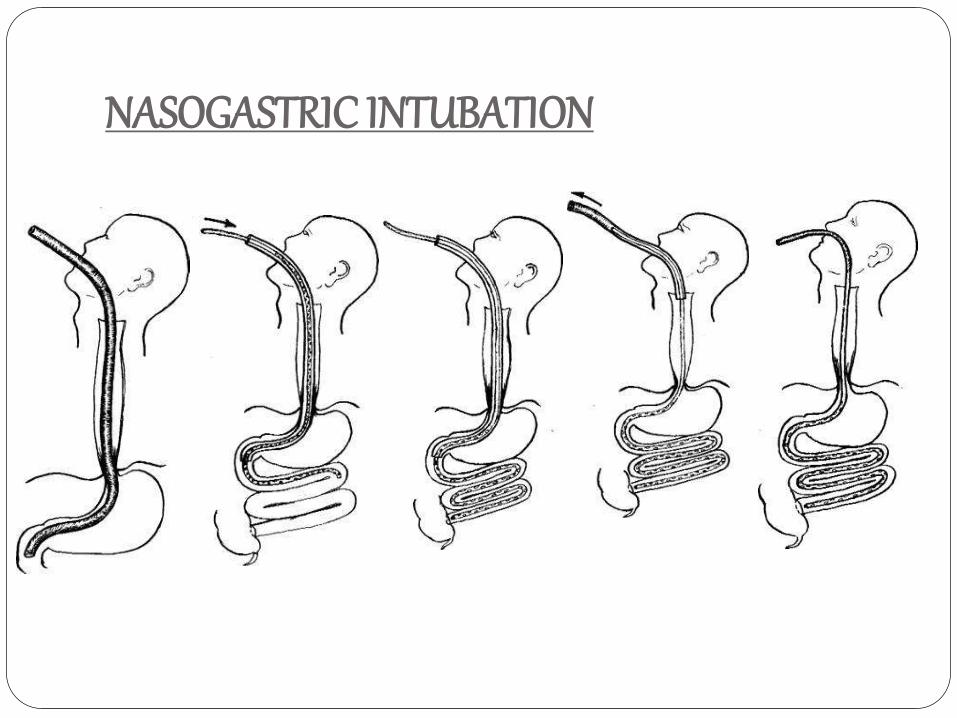
NASOGASTRIC INTUBATION
ACUTE INTESTINAL OBSTRUCTION
SURGICAL MANAGEMENT:
PRINCIPLES:
Management of segment at site of obstruction.
Management of distended proximal bowel.
Management of underlying cause of obstruction.
SURGICAL DECOMPRESSION:STEPS:
Nasogastric Intubation and suction.
Anaesthesia.
Incision.
Handling of the Gut.
Decompression of obstruction by Savage
Decompressor within purse-string sutures OR
Resection and Anastomosis.
Assess the viability of the bowel.
Prevention of Reperfusion Injury.
Closing of the Abdomen.
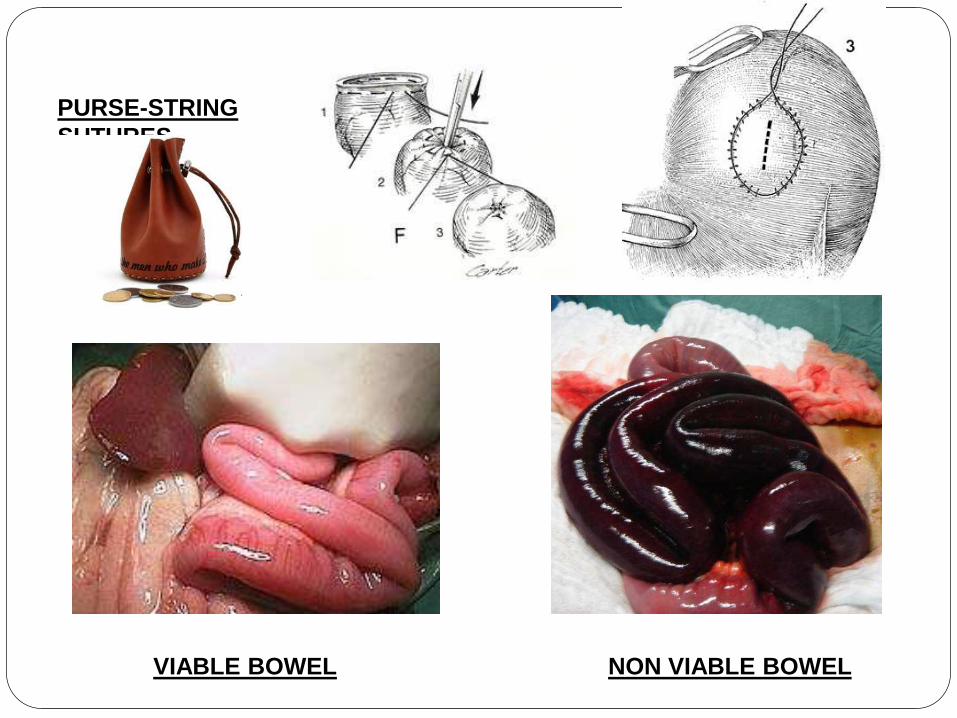
PURSE-STRING
SUTURES
VIABLE BOWEL NON VIABLE BOWEL
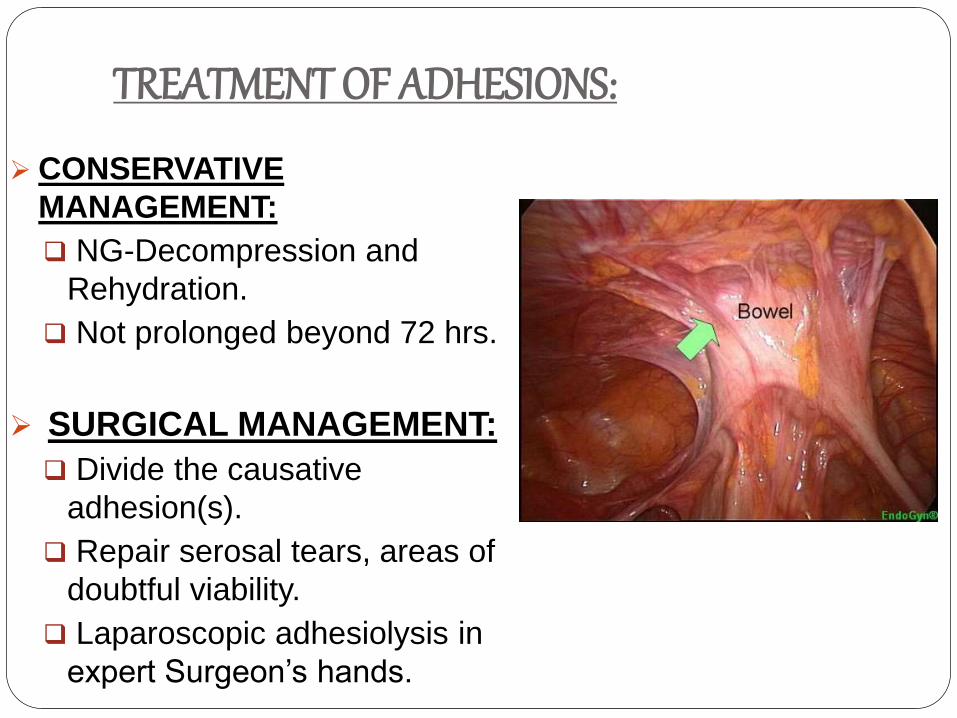
TREATMENT OF ADHESIONS:
CONSERVATIVE
MANAGEMENT:
NG-Decompression and
Rehydration.
Not prolonged beyond 72 hrs.
SURGICAL MANAGEMENT:
Divide the causative
adhesion(s).
Repair serosal tears, areas of
doubtful viability.
Laparoscopic adhesiolysis in
expert Surgeon’s hands.
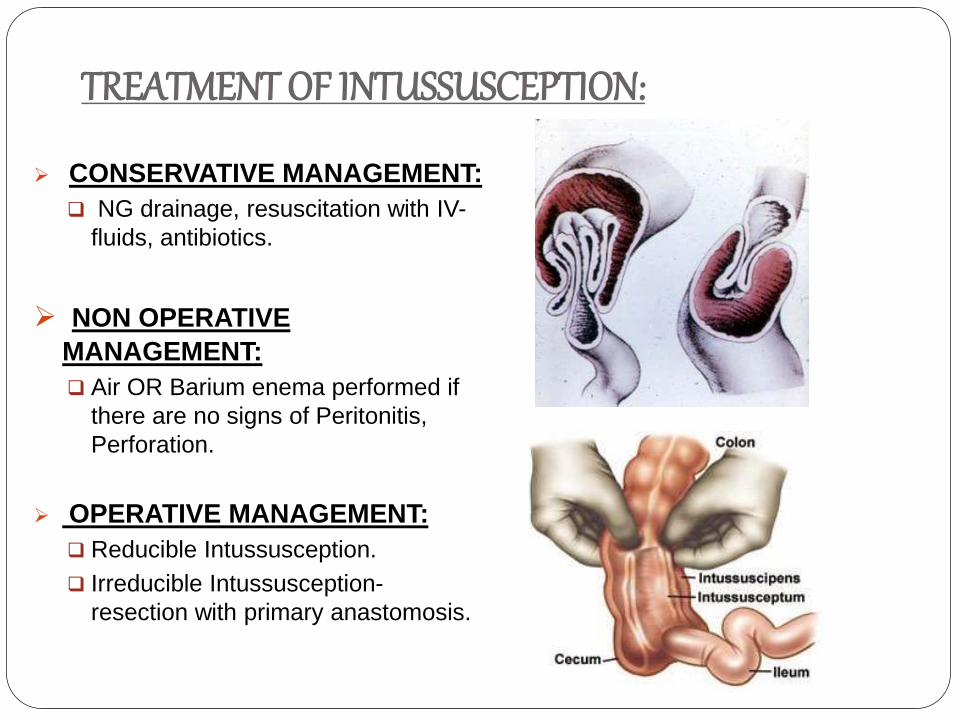
TREATMENT OF INTUSSUSCEPTION:
CONSERVATIVE MANAGEMENT:
NG drainage, resuscitation with IV-
fluids, antibiotics.
NON OPERATIVE
MANAGEMENT:
Air OR Barium enema performed if
there are no signs of Peritonitis,
Perforation.
OPERATIVE MANAGEMENT:
Reducible Intussusception.
Irreducible Intussusception-
resection with primary anastomosis.
LARGE BOWEL OBSTRUCTION:
Ususal cause is Carcinaoma, Diverticular
diseases, IBD.
But however should be differentiated with pseudo
obstruction.
Depends on the extent of the lesion.
Depends on whether lesion is removable or
irremovable.
situation of lesion:
CEACUM
COLON
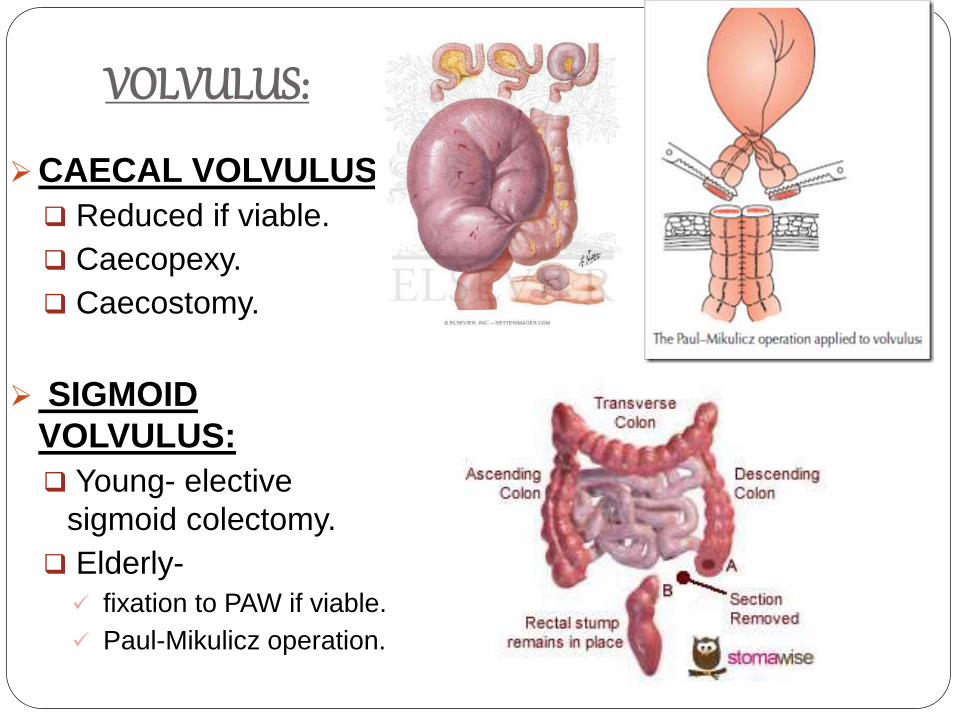
VOLVULUS:
CAECAL VOLVULUS:
Reduced if viable.
Caecopexy.
Caecostomy.
SIGMOID
VOLVULUS:
Young- elective
sigmoid colectomy.
Elderly-
fixation to PAW if viable.
Paul-Mikulicz operation.
ADYNAMIC OBSTRUCTION:
PARALYTIC ILEUS:
Failure of transmission of peristaltic waves
secondary to neuromuscular failure.
CAUSES:
Post-operative, Infection, Reflex Ileus, Metabolic.
MANAGEMENT:
NG-suction, Fluid replacement,
Use prokinetics (Domperidone/Erythromycin) in
resistant case
Laparotomy- if inactivity persists >7days, only after
confirmation of abdominal sepsis/mechanical
obstruction.
ADYNAMIC OBSTRUCTION:
PSEUDO-OBSTRUCTION:
Obstruction in absence of mechanical cause or acute intra-abdominal disease.
ASSOCIATIONS:
Metabolic, Severe Trauma, Shock, Retroperitoneal irritation, Drugs.
Radiographs show colon obstruction and distension.
If no obstruction, confirm by colonoscopy & Barium ennema.
MANAGEMENT: Treat the identifiable cause. IV-Neostigmine 1mg. (make patient sit on commode) Repeat with second dose after few minutes if first dose is ineffective. Colonoscopic decompression. Surgery is associated with high mortality and morbidity.
Thank you...







![Intestinal Obstruction Due to Retained, Eroding Surgical ... · Intestinal Obstruction Due to Retained, Eroding Surgical Sponge: A Case Report 131 [7] Wattanasirichaigoon S. Transmural](https://img.pdfslide.us/doc/110x75/5e8cd279baba4b78b8137e03/intestinal-obstruction-due-to-retained-eroding-surgical-intestinal-obstruction.jpg)








