Embed Size (px)
DESCRIPTION
Nov. 29th, 2011
Citation preview

Renal stones endoscopic Renal stones endoscopic managementmanagement
Dr sarwar noori Dr sarwar noori mahmoodmahmood
F.I.C.MS(urology), F.I.C.MS(urology), F.E.B.UF.E.B.U

Indications for treatmentIndications for treatment
Presence of symptoms and /or Presence of symptoms and /or obstruction obstruction
in a functioning kidneyin a functioning kidney

Treatment of Renal Treatment of Renal StonesStones
Four OptionsFour Options 1) conservative ,1) conservative ,
2) non-invasive:2) non-invasive: ESWL ESWL
3) minimal invasive : 3) minimal invasive : PCNL, URS PCNL, URS
4) open surgery4) open surgery
New technologyNew technology : : morbidity, morbidity, hospital stay,hospital stay,
invasivenessinvasiveness

Natural history of renal stones

SPONTANEOUS CLEARANCE OF STONES IN 3 MONTHS
< 4 m.m. 96%
4 to 6 m.m. 80%
6 to 8 m.m. 60%
8 to 10 m.m. 20%

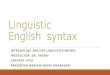
KIDNEYS
URETERS
BLADDER
PROSTATE
URETHRA
URINARY SYSTEMSpontaneous clearance of stones takes place
ONLY WHEN—
1.There is good flow of urine/function on the affected side
&
2.There is no distal obstruction

MANAGEMENT OF RENAL MANAGEMENT OF RENAL CALCULI by ESWLCALCULI by ESWL
<< 2cm in diameter and/or surface 2cm in diameter and/or surface area < 500 mmarea < 500 mm22
Treatment : ESWL mono-therapyTreatment : ESWL mono-therapy
>> 2cm in diameter and/or 2cm in diameter and/or surface area > 500 mmsurface area > 500 mm22
Treatment : PCNL +/- ESWLTreatment : PCNL +/- ESWL
Combination therapyCombination therapy

Treatment of Renal Treatment of Renal StonesStones

ESWLESWL

Generation of shock Generation of shock wavewave

T H E M A G I C W O R D--- LITHOTRIPSY
EXTRA CORPOREAL SHOCK WAVE LITHOTRIPSY
WHAT ARE SHOCK WAVES?



There should be a limited amount of gravel , which is expected to be passed out spontaneously within reasonable time limit , without causing much discomfort/colics .

IDEAL SITUATION FOR SUCCESSFUL
E.S.W.L.
Renal calculus of less than 2 cm having hetrogenous calcification/ architecture
In X- ray , in a well functioning renal unit with no distal obstruction


PROBLEMS WITH E.S.W.L.
Stones did not break:
obesity
*Chemical composition of stone
Stones did not pass –out:
*Poor or no function of this kidney
*Comparatively large amount of gravel got stuck and choked the system


Percutaneous nephrolithomy PCNL
The key-hole surgery

Indication of PCNL: Indication of PCNL: >2.5-3.0 cm>2.5-3.0 cm failure of ESWL (matrix,cystine,ca failure of ESWL (matrix,cystine,ca
oxalate monohydrate)oxalate monohydrate) cystine stone >1.5 cmcystine stone >1.5 cm lower calyx stone ≥ 2.0cm(narrow, lower calyx stone ≥ 2.0cm(narrow,
long, acute angel infuldibulopelvic long, acute angel infuldibulopelvic angel)angel)
caliceal diverticulumcaliceal diverticulum UU stone >1cm not respond to ESWL or UU stone >1cm not respond to ESWL or
difficult with URS.difficult with URS.

FUCTIONAL ANATOMY OF KIDNEYFOR
PERCUTANEOUS TECHNIQUE
1. VASCULAR
2. CALYCEAL
3. ANATOMIC RELATION


PERCUTANEOUS RENAL SURGERY
PRE – OP WORK UP
Urine culture
Renal function test
Haematological profile
Caogulation profile
KUB and IVU
US.

Steps for PCNLSteps for PCNL
Retrograde ureteric catheterization Retrograde ureteric catheterization Fluoroscopy-guided percutaneous Fluoroscopy-guided percutaneous
puncture(B-ultrasound for simple case)puncture(B-ultrasound for simple case) Tract dilationTract dilation LithotripsyLithotripsy Double-J stent and nephrostomy tube Double-J stent and nephrostomy tube
placementplacement

ANAESTHESIANAESTHESIAA
Epidural anesthesia (Most cases)Epidural anesthesia (Most cases) GGeneral anesthesiaeneral anesthesia (Obesity and lung (Obesity and lung
dysfunction)dysfunction) Local anesthesiaLocal anesthesia (( for second-lookfor second-look ))

Body positionBody position prone position (most prone position (most
cases)cases) side-lying side-lying
positionposition (( obesityobesity 、、 cardiorescardiorespiratory dysfunctionpiratory dysfunction ))
supine supine positionposition (( transplantetransplanted kidneyd kidney))


Retrograde ureteric Retrograde ureteric catheterizationcatheterization
6Fr ureteric catheter open end 6Fr ureteric catheter open end Wash out small stonesWash out small stones Prevent small stones moving from Prevent small stones moving from
pelvis into ureterpelvis into ureter


AMPLATZ SHEATH
- Metallic
- Teflon





X-rayX-ray UltrasonograpUltrasonographyhy
Which one is betterWhich one is better ?? 2 methods combination 2 methods combination better.why?better.why?














Air pneumatic lithotripterAir pneumatic lithotripter Ho:YAG laser Ho:YAG laser 3th generation EMS3th generation EMS
Which one is better?Which one is better?

Double-J stent and nephrostomy tube Double-J stent and nephrostomy tube placement,Tubeless PCNL NOT placement,Tubeless PCNL NOT
commoncommon



PERCUTANEOUS RENAL SURGERY
COMPLICATIONS
1. RENAL PELVIC PERFORATION 2. HAEMORRHAGE 3. INJURY ADJACENT ORGANS 4. UROSEPSIS 5. FLUID ABSORPTION 6. AV MALFORMATION


Ureteric stoneUreteric stone

INDICATIONS FOR INTERVENTION:INDICATIONS FOR INTERVENTION:The classical indications for intervention are well The classical indications for intervention are well
known & include the following:known & include the following:* Presence of infection* Presence of infection* Presence of obstruction* Presence of obstruction* Persistent colic with no advancement of the stone* Persistent colic with no advancement of the stone* A stone more than 0.5 cm in diameter* A stone more than 0.5 cm in diameterThe classical indications have recently been modified The classical indications have recently been modified
because of the advent of new technology & the high because of the advent of new technology & the high expectations of today's patients.expectations of today's patients.
THERAPEUTIC OPTIONS:THERAPEUTIC OPTIONS:These include:These include:* Surgery* Surgery* Percutaneous surgery* Percutaneous surgery* Ureteroscopy with Electrohydraulic lithotripsy(EHL), * Ureteroscopy with Electrohydraulic lithotripsy(EHL),
Ultrasound lithotripsy, Ultrasound lithotripsy, Laserlithotripsy, Electro-mechanical Impactor Laserlithotripsy, Electro-mechanical Impactor
lithotripsy, & Lithoclast lithotripsy.lithotripsy, & Lithoclast lithotripsy.* ESWL* ESWL* Spontaneous passage* Spontaneous passage

MANAGEMENT OF MANAGEMENT OF URETERIC STONESURETERIC STONES
-Stones < 0.5 cm in diameter doesn’t -Stones < 0.5 cm in diameter doesn’t pass pass
spontaneously 4 to 6 weeks and /or spontaneously 4 to 6 weeks and /or causing symptoms : ESWL causing symptoms : ESWL monotherapymonotherapy
-Stones > 0.5 cm in diameter & < 1 -Stones > 0.5 cm in diameter & < 1 cm in cm in
diameter : ESWL monotherapydiameter : ESWL monotherapy

MANAGEMENT OF MANAGEMENT OF URETERIC STONESURETERIC STONES
Stones > 1 cm in diameter : trial of Stones > 1 cm in diameter : trial of ESWL monotherapyESWL monotherapy
Patient counselled:Patient counselled:
1.1. Repeat session may be Repeat session may be necessarynecessary
2.2. URS/PCNL/ureterolithotomy URS/PCNL/ureterolithotomy

RESULTS OF RESULTS OF URETROSCOPIC URETROSCOPIC
LITHOTRIPSY (URS)LITHOTRIPSY (URS)Achieved stone free status = 85% to 90%Achieved stone free status = 85% to 90%
Failures:Failures:
1.1. Access problemsAccess problems
2.2. Stone migrationStone migration
Flexible URS for upper third ureteric Flexible URS for upper third ureteric calculicalculi
especially in the maleespecially in the male

URS complications:URS complications: pain ,sepsis ,damage to ureteral pain ,sepsis ,damage to ureteral
mucosa and wall, failuremucosa and wall, failure

RENAL STONESRENAL STONES

NephrolithotomyNephrolithotomy

PREVENTION OF PREVENTION OF STONESSTONES
1.1. Treatment of causesTreatment of causes
2.2. Dietary manipulationsDietary manipulations
3.3. Medications - indication Medications - indication durationduration

DIETARY ADVICEDIETARY ADVICE
1.1. HydrationHydration
2.2. Avoid oxalate-rich foodAvoid oxalate-rich food
3.3. Avoid calcium-rich food ?Avoid calcium-rich food ?
4.4. Avoid refined carbohydratesAvoid refined carbohydrates
5.5. Increase crude fibresIncrease crude fibres

MEDICATIONSMEDICATIONS
1.1. ThiazidesThiazides
2.2. AllopurinolAllopurinol
3.3. AntibioticsAntibiotics
4.4. Sodium bicarbonateSodium bicarbonate
5.5. Potassium citratePotassium citrate
6.6. Magnesium saltsMagnesium salts
7.7. PyridoxinePyridoxine