Embed Size (px)
Citation preview

VinhVinho de o de PortPort
oo

General ObjectiveGeneral
Objective
Specific Objectives
Specific Objectives
To recognize symptoms of Sturge Weber Syndrome.To discuss the management and treatment and prognosis of patients diagnosed with the Sturge Weber Syndrome.
To Study the etiology, clinical and pathological features, diagnosis and treatment of Sturge-weber syndrome

GENERAL DATA
Filipino, Born again Christian ,Marikina City
Admitted on Dec 11 for the 1st time at ARMMC
J.S., 3 months old Male

• Chief Complaint: Upward rolling of eyeballs with stiffening of extremities

History Of Present Illness

Review of Systems

Review of Systems

y
Birth History & Maternal History
Born to a 32 year old G4P4 (4004) mother
Normal spontaneous delivery, lying in Clinic ,assisted by midwife, denies maternal illness.
patient had spontaneous cry and good activity



Physical Examination (ER)



DIFFERENTIAL DIAGNOSIS
Rule in Rule Out
Klippel-Trenaunay-Weber Syndrome
Port wine Stain
Soft Tissue Hypertrophy
Solid visceral tumors Soft tissue hypertrophy

Rule in Rule out
Beckwith-Wiedemann Syndrome
Port wine stain
Prominent occiput
Macroglossia
Omphalocele

Rule in Rule out
Dyke-davidoff-masson syndrome
Seizure Facial asymmetry
contralateral hemiparesis

Upon Admission
Breast feeding with strict aspiration precautions IVF: D5IMB (maintenance) Diagnostics: CBC with platelet count Urinalysis Chest x-ray CSF Analysis Cranial CT Scan (with contrast) EEG Therapeutics: Ampicillin (200 mkd) Paracetamol drops (10mkdose) Diazepam (0.2mkdose) PRN
Phenobarbital (5mkd)O2 inhalation at 2-3 LPM PRN


CBC with APC (12/11)
CSF Analysis (12/15)
WBC 7.6
Hgb 10.4
Hct 32.7
Pl. ct. 490
Segmenters 46
Lymphocytes 49
Neutrophils 5
color colorless, clear fluid with small red precipitate
WBC 965 cells/ uL
RBC 289,500 cells / uL with segmenters of 0.03
lymphocytes 0.97
sugar 2.83mmol/l (2.2- 3.9)
protein 2,885mg mg/L;
culture no growth


1st – 2nd Hospital Day
• BP 90/50-60 mmHg• HR= 128-142bpm• RR = 28-42 cpm• Temp = 36.7 –37c • (-) seizure• Meds and IVF were
continued• Patient was
transferred to regular ward
3rd Hospital Day• BP 90/50-60 mmHg• HR= 132-148 bpm• RR = 28-42 cpm• Temp = 36.7 - 37C• (+) seizure one
episode= afebrile• IVF was consumed and
was shifted to heplock• IV meds were
continued

4th-7th Hospital Day
• BP 90/50-60 mmHg• HR= 128-142bpm• RR = 28-42 cpm• Temp = 36.7 –37c • (-) seizure• Meds and IVF were continued.• Cranial CT Scan with contrast was done.• Referral to ophthalmology service was done.

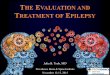
Cranial CT Scan with Contrast (12/19)

8th Hospital Day
Diagnosis: STURGE-WEBER SYNDROME
•Patient was referred to Ophthalmology Service for evaluation of probability of having glaucoma
OPHTHA NOTES
Patient is recommended to be seen by a Glaucoma Specialist in other institution for further evaluation and management.
Patient may start with Timolol maleate Eye drops, 2 drops OU BID
Patient is for possible Goniotomy
•IOP - OD soft
OS hard
Assessment: Congenital Glaucoma secondary to Sturge-Weber Syndrome
9th Hospital Day
DISCHARGED:
Home meds
1. Timolol maleate eye drops BID
2. Phenobarbital 13mg pptab, 1 tab BID


DISCUSSION.


Etiology

Masanori Takeoka, MD, et al (Pediatric Sturge-Weber Syndrome Medication) January 5, 2010Nelson text book of Pediatrics 19th edition.

Pathophysiology
residual vascular tissue
angiomata
neurological dysfunction
neurological deterioration with ocular manifestation

Sujansky and Conradi, American Journal of Med 57:35-45 (1995.)

Diagnosis
Tram track appearance

Classification

Treatment
Sturge weber syndrome, som.unm.edu/coc/docs/Sturge.pdf cited July3,

Prognosis
Sturge weber syndrome, som.unm.edu/coc/docs/Sturge.pdf cited July3,

Summary
• The patient is classified as type I.
• Seizures were controlled with diazepam and Phenobarbital.
• CNS imaging and Ophthalmology consultation confirms SWS.
• Advised for close follow up in pediatrics OPD and refer to Glaucoma specialist for possible Goniotomy.