Embed Size (px)
Citation preview

Diagnosis and Management of Stroke
Dr. Anoop K RAsst professor
Dept of general medicineMMCH,Calicut

Objectives
• Review etiology of strokes• Identify likely location/type of stroke based on
physical examination• Acute management of ischemic stroke• Acute management of hemorrhagic stroke

1. WHO - A NEUROLOGICAL DEFICIT OF• Sudden onset• With focal rather than global dysfunction• In which, after adequate investigations, symptoms are presumed to be of
non-traumatic vascular origin• and last for >24 hours
2. NINDS 2005 - When the blood supply to part of the brain is suddenly interrupted or when a blood vessel in the brain bursts
3. TIA - neurological deficit of vascular origin lasting from few minutes to hours and resolves within 24 hours
Definitions

Stroke
Atherosclerotic(20%)
Cryptogenic(30%)
Unusual causesProthrombotic
DissectionsArteritisMigraine
Drug abuse(5%)
HaemorrhageIntraparenchymal
Subarachnoid(15%)
Cardioembolic(20%)
Penetating arteryDisease
(lacunar)(25%)
ISCHEMIC 85%HEMORRHAGIC 15%

How to asses stroke?


NIHSS• NIHSS (National Institute of Health Stroke Scale)
– Standardized method used by health care professionals to measure the level of impairment caused by a stroke
– Purpose• Main use is as a clinical assessment tool to determine whether
the degree of disability is severe enough to warrant the use of tPA
• Another important use of the NIHSS is in research, where it allows for the objective comparison of efficacy across different stroke treatments and rehabilitation interventions
– Scores are totaled to determine level of severity– Can also serve as a tool to determine if a change in exam has
occurred

Possible Points: SummaryLOC 7Cranial Nerves (Portions of CN II,III,V,VI,VII) 8Motor 8x2 = 16Ataxia 2Sensory 2Language 5Inattention 2 =42

NIHSS and Patient Outcomes• Total scores range from 0-42 with higher values representing
more severe infarcts– >25 Very severe neurological impairment– 15-24 Severe impairment– 5-14 Moderately severe impairment– <5 Mild impairmentAdams, HP, et al. (1999). Neurology: 53: 126-131.
• A 2-point (or greater) increase on the NIHSS administered serially indicates stroke progression. It is advisable to report this increase.

TIA - ABCD2 Score
Symptom ScoreAge > 60 years 1 pointBlood pressure > 140/80 1 pointClinical (neurological deficit)
2 points for hemiparesis1 point for speech problem without weakness
Duration 2 points for >60 minutes1 point for 10-60 min
Diabetes 1 point
Maximal score is 7

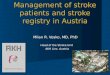
• The Alberta Stroke Programe Early CT Score (ASPECTS) is a 10-point quantitative topographic CT scan score used in patients with middle cerebral artery (MCA) stroke.
• Segmental assessment of MCA territory is made and 1 point is removed from the initial score of 10 if there is evidence of infarction in that region.
• caudate • putamen • internal capsule* • insular cortex • M1: "anterior MCA cortex," corresponding to frontal operculum • M2: "MCA cortex lateral to insular ribbon" corresponding to anterior
temporal lobe • M3: "posterior MCA cortex" corresponding to posterior temporal lobe

•M4: "anterior MCA territory immediately superior to M1"
•M5: "lateral MCA territory immediately superior to M2"
•M6: "posterior MCA territory immediately superior to M3"
(M1 to M3 are at the level of the basal ganglia and M4 to M6 are at the level of the ventricles immediately above the basal ganglia)
An ASPECTS score less than or equal to 7 predicts worse functional outcome at 3 months as well as symptomatic haemorrhage.

TIA – Management People who have had a suspected TIA who are at lower risk of stroke ABCD2 score of 3 or below: should have
•aspirin (300 mg daily) started immediately•specialist assessment and investigation as soon as possible, but definitely within 1 week of onset of symptoms •measures for secondary prevention introduced as soon as the diagnosis is confirmed, including discussion of individual risk
NB: People who have had a TIA but who present late (more than 1 week after their last symptom has resolved) should be treated as though they are at lower risk of stroke.

-cont People who have had a suspected TIA who are at high risk of stroke TIAs with ABCD2 score ≥ 4 or above should have:
•aspirin (300 mg daily) started immediately •specialist assessment and investigation within 24 hours of onset of symptoms•measures for secondary prevention introduced as soon as the diagnosis is confirmed, including discussion of individual risk
TIAS with a score of 5 or greater to be admitted for immediate Dx and Tx (within 24 Hrs)

• Most likely related to decreased level of consciousness (LOC), dysarthria, dysphagia
• GCS < 8 - INTUBATE• Avoid Hyperventilation or Hypoventilation• NPO until swallow assessment completed- high aspiration risk • Begin mobilization as soon as clinically safe• Keep HOB greater than 30 degrees
Airway Mx

ImagingCT scan• Non- contrast CTH remains
the gold standard as it is superior for showing IVH and ICH
• CT with contrast may help identify aneurysms, AVMs, or tumors but is not required to determine whether or not the patient is a tPa candidate
MRI• Superior for showing
underlying structural lesions• Contraindications



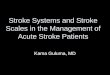
Watershed zones


Acute (4 hours)Infarction
Subtle blurring of gray-white junction & sulcal effacement
Subacute (4 days) Infarction
Obvious dark changes & “mass effect” (e.g.,
ventricle compression)
RR L L

Multimodal Imaging
Multimodal CT• Typically includes non-
contrast CT, perfusion CT, and CTA
• Two types of perfusion CT– Whole brain perfusion CT– Dynamic perfusion CT
Multimodal MRI• Standard MRI sequences
(T1 weighted, T2 weighted, and proton density) are relatively insensitive to changes in cerebral ischemia
• Multimodal adds diffuse-weighted imaging (DWI) and PWI (perfusion- weighted imaging)

Treatment


tPa
Fast Facts• Tissue plasminogen
activator• “clot buster”• IV tpa window 3 hours• IA tpa window 4.5 hours • Disability risk 30% despite
~5% symptomatic ICH risk
Contraindications• Hemorrhage• SBP > 185 or DBP > 110• Recent surgery, trauma or
stroke • Coagulopathy• Seizure at onset of symptoms• NIHSS >21 • Age?• Glucose < 50

Patients should receive endovascular therapy with a stent retriever if they meet all the following criteria (Class I). (New recommendation):– pre-stroke Modified Rankin Scale score 0 to 1– acute ischemic stroke receiving IV r-tPA within 4.5
hours of onset according to guidelines from professional medical societies
– causative occlusion of the ICA or proximal MCA– age ≥18 years– NIHSS score of ≥6– Alberta Stroke Program Early CT score (ASPECTS) ≥6– treatment can be initiated (groin puncture) within 6
hours of symptom onset

Administration of rTPAMain eligibility criteria
FOR IV INFUSION
Treatment given within 3hrs) Intracranial bleeding excluded Age <80 Early major infarction excluded (parenchyma hypo-attenuation or brain swelling
>1/3rd MCA territory)
NIHSS SCORE <22
BP < 185/110 Not on warfarin or heparin, platelets and coagulation normal
Treatment given by a specially trained physician Facilities for close monitoring

Mechanical Thrombolysis
• Often used in adjunct with tPa• MERCI (Mechanical Embolus Removal in
Cerebral Ischemia) Retrieval System is a corkscrew-like apparatus designed to remove clots from vessels
• PENUMBRA system aspirates the clot

Blood Pressure Management
– The goal is to maintain cerebral perfusion!!– CPP = MAP – ICP (needs to be at least 70)– Higher BP goals with Ischemic stroke– Lower BP goals with Hemorrhagic stroke (avoid
hemorrhagic expansion, especially in AVMs and aneurysms)

BP Relationship• BP increase is due to
arterial occlusion (i.e., an effort to perfuse penumbra)
• Failure to recanalize (w/ or w/o thrombolytic therapy) results in high BP and poor neuro outcomes
• Lowering BP starves penumbra, worsens outcomes
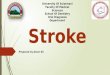
Penumbra
Core
Clot in Artery

Save the Penumbra!!
CEREBRALBLOODFLOW(ml/100g/min)
CBF< 8
CBF8-18
TIME (hours)1 2 3
20
15
10
5
PENUMBRA
CORE
Neuronal dysfunctio
n
Neuronal death
Normal function

STROKE SURGERYHEMORRHAGIC
A. Lobar hemorrhage STICH Trial - Mendelow AD et al. Lancet 2005 -No difference in outcome in stable patients -Surgery Outcome better than conservative RX in progressive Neurological deterioration. B. Basal ganglia Hemorrhage Endoscopy Evacuation better than conservative treatment, Vol.> 50cc, age < 50 years
C. Cerebellar Hemorrhage with obstructive hydrocephalus Surgical Emergency

UROKINASE OR TPA INSTILATION AND MINIMALLY INVASIVE ASPIRATION

ISCHEMIC
People with middle cerebral artery (MCA) infarction who meet all of the criteria below should be considered for decompressive hemicraniectomy (decimal trial).
• They should be referred within 24 hours of onset of symptoms and treated within a maximum of 48 hours
• aged 60 years or under• clinical deficits suggestive of infarction in the territory of the MCA with a
score on the NIHSS of above 15• decrease in the level of consciousness to give a score of 1 or more on item
1a of the NIHSS• signs on MRI of an infarct of at least 50% of the MCA territory, with or
without additional infarction in the territory of the anterior or posterior cerebral artery on the same side, or
• infarct volume greater than 145 cm3 as shown on diffusion-weighted MRI

Supportive Therapy
Glucose Management– Infarction size and edema increase with acute and chronic
hyperglycemia– Hyperglycemia is an independent risk factor for hemorrhage
when stroke is treated with t-PA
Antiepileptic Drugs– Seizures are common after hemorrhagic CVAs– ICH related seizures are generally non-convulsive and are
associated to with higher NIHSS scores, a midline shift, and tend to predict poorer outcomes

Hyperthermia
• Treat fevers!– Evidence shows that fevers > 37.5 C that persists
for > 24 hrs correlates with ventricular extension and is found in 83% of patients with poor outcomes

• Every hospital should have a stroke unit• A stroke should be managed by a multidisciplinary stroke
team• An efficient referral and rehabilitation system to be
established for the success of a stroke unit• Stroke units significantly reduce death, dependency,
institutionalization and length of hospital stay.
STROKE UNIT

Thank you for your attention!

Etiology of Ischemic Strokes
LARGE VESSEL THROMBOTIC:Virchow’s Triad….• Blood vessel injury
- HTN, Atherosclerosis, Vasculitis• Stasis/turbulent blood flow
- Atherosclerosis, A. fib., Valve disorders• Hyper coagulable state
- Increased number of platelets- Deficiency of anti-coagulation factors - Presence of pro-coagulation factors- Cancer

LARGE VESSEL EMBOLIC:• The Heart
– Valve diseases, A. Fib, Dilated cardiomyopathy, Myxoma
• Arterial Circulation (artery to artery emboli)– Atherosclerosis of carotid, Arterial dissection, Vasculitis
• The Venous Circulation – PFO w/R to L shunt, Emboli

Determining the Location• Large Vessel:
– Look for cortical signs
• Small Vessel:– No cortical signs on exam
• Posterior Circulation:– Crossed signs– Cranial nerve findings
• Watershed:– Look at watershed and border zone areas– Hypo-perfusion

Cortical Signs
RIGHT BRAIN: LEFT BRAIN:
- Right gaze preference - Left gaze preference
- Neglect - Aphasia
• If present, think LARGE VESSEL stroke

Large Vessel Stroke Syndromes
• MCA: – Arm>leg weakness– LMCA cognitive: Aphasia– RMCA cognitive: Neglect, topographical difficulty, apraxia,
constructional impairment
• ACA: – Leg>arm weakness, grasp– Cognitive: muteness, perseveration, abulia, disinhibition
• PCA: – Hemianopia– Cognitive: memory loss/confusion, alexia
• Cerebellum: – Ipsilateral ataxia

Aphasia• Broca’s
– Expressive aphasia– Left posterior inferior
frontal gyrus
• Wernicke’s– Receptive aphasia– Posterior part of the superior temporal gyrus– Located on the dominant side (left) of the brain

Etiology of ICH
• Traumatic• Spontaneous (non traumatic)
– Hypertensive– Amyloid angiopathy– Aneurysmal rupture– Arteriovenous malformation rupture– Bleeding into tumor– Cocaine and amphetamine use

Hypertensive ICH
• Spontaneous rupture of a small artery deep in the brain• Typical sites
– Basal Ganglia– Cerebellum– Pons
• Typical clinical presentation– Patient typically awake and often stressed, then abrupt
onset of symptoms with acute decompensation

Ganglionic Bleed
• Contralateral hemiparesis• Hemisensory loss• Homonymous hemianopia• Conjugate deviation of eyes toward the side of the bleed or
downward• AMS (stupor, coma)

Cerebral Hemorrhage
JPG

Cerebellar Hemorrhage
• Vomiting (more common in ICH than SAH or Ischemic CVA)• Ataxia• Eye deviation toward the opposite side of the bleed • Small sluggish pupils• AMS

Pontine Hemorrhage
• Pin-point but reactive pupils• Abrupt onset of coma• Decerebrate posturing or flaccidity • Ataxic breathing pattern

Subarachnoid Hemorrhage• “Worst headache of my life”• AMS• Photophobia• Nuchal rigidity • Seizures• Nausea and vomiting

Case 1 • 74 year old African American female with sudden
onset of left-sided weakness
• She was at church when she noted left facial droop
• History of HTN and atrial fibrillation
• Meds: Losartan

• BP- 172/89, P– 104, T- 98.0, RR– 22, O2- 94%
• General exam: Unremarkable except irregular rate and rhythm
• NEURO EXAM:- Speech dysarthric but language intact- Right gaze preference- Left facial droop- Left- sided hemiplegia- Neglect


Answer
• Right MCA infarct, most likely cardioembolic from atrial fibrillation• Patient underwent mechanical thrombectomy with intra-arterial
verapamil, clot removal successful• Excellent recovery – patient was discharged 48 hours later on
Coumadin• Small vessel disease – since there are no cortical signs on exam• Risk factors – HTN, DM, tobacco use, sleep apnoea

Case 2
• 85 year old male who woke up with left face, arm, and leg numbness
• History of HTN, DM, and tobacco use
• Meds: Insulin, aspirin

• BP- 168/96, P– 92
• General exam: Unremarkable, RRR
• NEURO EXAM:- Decreased sensation on left face, arm, and leg

Case 2

Answer
• Right thalamic lacunar infarct• Not a candidate for intervention• Discharged to rehab 72 hours after admission• location – posterior circulation – due to crossed signs, cranial
nerve findings.

Brainstem Stroke Syndromes
• Rarely presents with an isolated symptom
• Usually a combination of cranial nerve abnormalities, and crossed motor/sensory findings such as:
– Double vision– Facial numbness and/or weakness– Slurred speech– Difficulty swallowing– Ataxia– Vertigo– Nausea and vomiting– Hoarseness

Case 3• 55 year old male with acute onset of right sided numbness
and tingling, left sided face pain and numbness, gait imbalance, nausea/vomiting, vertigo, swallowing difficulties, and hoarse speech
• History of CAD s/p CABG, DM2, HTN, HLD, OSA
• Meds: Aspirin, plavix, insulin, lipitor, metoprolol, lisinopril

• NEURO EXAM: BP- 194/102, P– 105
• General exam: Unremarkable, RRR
• NEURO EXAM:- Decreased sensation on left face- Decreased sensation on right body- Left ataxia on FNF, and unsteady gait- Voice hoarse- Nystagmus


Answer
• Brainstem Stroke• Received IV tPa• Post-tPa symptoms greatly improved
regained sensation, ataxia resolved• Discharged home with out patient PT/OT• Location – watershed pattern

Case 4• 56 year old female who upon waking post-op after elective
surgery was found to have L sided weakness and neglect
• History of HTN
• Meds - Lisinopril

• BP- 132/74, P– 84
• General exam: Unremarkable, RRR
• NEURO EXAM:- Left face, arm, and leg weakness- Neglect- DTR’s brisk on the left, toe up on left




• Right hemisphere watershed infarct secondary to hypoperfusion in the setting of Right ICA stenosis
• On review of anesthesia records, blood pressure dropped to 82/54 during the procedure
• Patient was discharged to in-patient rehab
Answer