Embed Size (px)
Citation preview

THROMBOEMBOLIC STROKEDR. IBEANU CHARLES

• DEFINITION• EPIDEMIOLOGY / BURDEN• CLASSIFICATION / ETIOLOGY• PATHOPHYSIOLOGY• RISK FACTORS• CLINICAL PRESENTATION• DIAGNOSIS• MANAGEMENT• PREVENTION / COMMUNITY IDENTIFICATION
OUTLINE

“Rapidly developing clinical signs of focal (or global) disturbance of cerebral function, with symptoms lasting 24 hours or longer or leading to death, with no apparent cause other than of vascular origin”
By this definition, TIA, which lasts <24 hours, and patients with stroke symptoms caused by subdural hemorrhage, tumors, poisoning or trauma are excluded.
DEFINITION(By WHO)

EPIDEMIOLOGY
• Annually, 15 million worldwide suffer a stroke- 5 million die and 5 million are permanently disabled
• WHO estimates a stroke occurs every 5 seconds• Stroke related disability is the sixth most common cause
of reduced DALYs• Accounts for 10% of all deaths worldwide
BURDEN OF STROKE
Stroke has assumed an epidemic proportion in developing countries especially sub-Saharan Africa (SSA)
World Stroke Congress declared stroke as an epidemic and called WHO and WSO combined efforts
The sub-Saharan Africa bears the brunt:
Two-thirds of cases
High case fatality

Ischemic Stroke — three subtypes:• Thrombosis : In situ obstruction of an artery. • Embolism : Particles of debris originating elsewhere that
block arterial access to a particular brain region.• Systemic hypoperfusion : More general circulatory problem,
manifesting itself in the brain and perhaps other organs.
Hemorrhagic Stroke due to intracerebral hemorrhage or subarachnoid hemorrhage
Data compiled by AHA show that strokes due to ischemia, intracerebral hemorrhage and subarachnoid hemorrhage are 87%, 10%, and 3 %respectively
CLASSIFICATION

CLASSIFICATION

TOAST Classification [9]
1. Large-artery atherosclerosis (embolus/thrombosis)*
2. Cardioembolism (high-risk/medium-risk)*
3. Small-vessel occlusion (lacune)*
4. Stroke of other determined etiology*
5. Stroke of undetermined etiology
a. Two or more causes identified
b. Negative evaluation
c. Incomplete evaluation*Possible or probable depending on results of ancillary studies.
STROKE SUBTYPES
Stroke Data Bank Subtype (NINDS) Classification [10]
Derived from the Harvard Stroke Registry classification, the National Institute of Neurological Disorders and Stroke (NINDS) Stroke Data Bank recognised -
1. Atherothrombosis
2. Tandem arterial pathology
3. Cardiac Embolism
4. Lacune
5. Unusual Cause
6. Infarction of undetermined cause
7. Parenchymatous haemorrhage
8. Subarachnoid Hemorrhage
SUBTYPES

Based on symptoms -
1.Total anterior circulation stroke (TAC)
2. Partial anterior circulation stroke (PAC)
3.Lacunar stroke (LAC)
4. Posterior circulation stroke (POC)
The type of stroke is then coded by adding a final letter to the above:• I – for infarct (e.g. TACI)• H – for haemorrhage (e.g. TACH)• S – for syndrome; intermediate pathogenesis, prior to imaging (e.g.
TACS) These four entities predict the extent of the stroke, the area of the brain affected, the
underlying cause, and the prognosis.
OXFORD CLASSIFICATION

A. ThrombosisLarge extracranial vessels
• Atherosclerosis• Dissection• Takayasu arteritis• Giant cell arteritis• Fibromuscular dysplasia
Small vessel disease • Lipohyalinosis ( due to hypertension) and fibrinoid
degeneration
ETIOLOGY

1. Cardiac sources definite - antithrombotic therapy generally used
Left atrial thrombus
Left ventricular thrombus
Atrial fibrillation
Sustained atrial flutter
Recent myocardial infarction (within 1 month)
Rheumatic mitral or aortic valve disease
Bioprosthetic and mechanical heart valve
Chronic myocardial infarction with ejection fraction <28 percent
Symptomatic heart failure with ejection fraction <30 percent
Dilated cardiomyopathy
B.Cardioaortic embolic stroke
2. Cardiac sources possible
Mitral annular calcification
Patent foramen ovale
Atrial septal aneurysm
Atrial septal aneurysm with patent foramen ovale
Left ventricular aneurysm without thrombus
Isolated left atrial smoke (no mitral stenosis or atrial fibrillation)
Mitral valve strands
3. Cardiac sources definite - anticoagulation hazardous
Bacterial endocarditis
Atrial myxoma
4. Ascending aortic atheromatous disease

Obstruction caused by development of fatty deposits lining the vessel walls. It mainly affects the vessels of the brain and heart. Thrombosis refers to thrombus usually blood clot that develops at clogged part of the vessel usually heart & large arteries of upper chest & neck. Embolism refers generally to blood clot that breaks loose enter the blood stream & travel through the brain blood vessel until it reaches the vessel too small to let it pass. Another cause is an irregular heart beat known as atrial fibrillation where clot can form in the heart, dislodge & travel to the brain.
Silent stroke is a brain injury likely caused by blood clot interrupting blood flow in the brain. It’s a risk factor for future strokes which could lead to progressive brain damage`
PATHOPHYSIOLOGY

Ischemic stroke reduces energy availability and therefore membrane ionic primes fail rapidly. The increase in extracellular potassium can reach levels sufficient to release excitotoxic neurotransmitters (e.g., glutamate and aspartate) to stimulate sodium/calcium channels coupled to glutamate receptors that can facilitate developing cytotoxic edema. The significant influx of calcium through calcium channels increase free cytosolic calcium that causes mitochondrial calcium overload, cessation of already compromised ATP production, and extensive breakdown of cellular phospholipids, proteins, and nucleic acids owing to Ca2+ activation of phospholipases, proteases, and endonucleases. Free radicals are produced in the process and contribute to membrane lipid peroxidation, protein and nuclear DNA toxic changes, and cellular injury (i.e., necrosis and/or apoptosis).
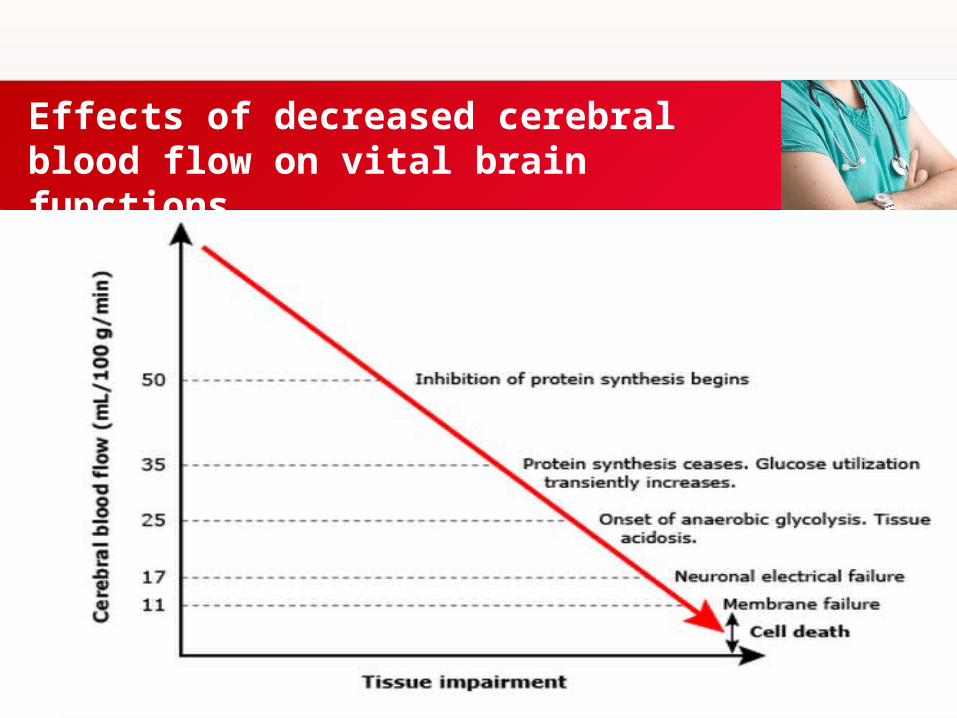
Effects of decreased cerebral blood flow on vital brain functions

• Family history of stroke: non-modifiable• Male gender: non-modifiable• History of TIAs: non-modifiable
– Warning events– Risk 1-2% at 1 wk; 2-4% at 1 mth– Canadian study: 6-7% at 30days; 9.5% at 90days;
stroke resulting in death/yr 21.8%– OXVASC 8.6% in 1 wk, 11.5% in 1mth,17.3% in
3mths– Prognosis
• Age>60; symptom duration; diabetes; weakness; speech impairment
RISK FACTORS
• Homocystinuria: non-modifiable– Recessive/dominant enzyme def– Most common recessive cystathione β synthase on chrm 21q22.3– Premature atherosclerosis, ectopia lentis, mental retardation, skeletal deformities,
osteoporosis, recurrent venous thrombosis
• Hypertrophic cardiomyopathy: non-modifiable• Hereditary hyperlipidemias: non-modifiable
– Types II & IV– Alpha lipoproteinemia– Tangier’s disease; familial hypercholesterolemia
• Mitochondrial encephalomyopathy (MELAS): non-modifiable

• Carotid stenosis stenting, endarterectomy, angioplasty
• Aortic arch atheroma• Arterial dissection
– Vaso-occlusive disease (Moyamoya)– Aneurysmata– Vascular fistulae– Type IV Ehler-Danlos (type III collagen deficit; autosomal dominant)
• Carotid-carvenous fistulae• Intracranial aneurysmata• Arterial dissection

• Marfans syndrome: non-modifiable– Autosomal dominant; defect in fibrillin type 1 or TGFβ receptor type II
gene (chrm 15, 3)– Characteristic habitus– Aortic dissection & carotid arteries– Intra/extracranial aneurysmata
• Pseudoxanthoma elasticum: non-modifiable• Autosomal dominant/recessive• Elastic fibers of skin, eye,vasculature• Occlusive lesions of carotid/cervical arteries• Moyamoya• Intracranial aneurysmata• Arterial dissection rarely
• Neurofibromatosis type I– Autosomal dominant; mutation in tumor suppressor gene, neurofibromin– Stenosis/occlusion of supraclinoid ICA with moyamoya– AV fistulae, aneurysmata
• Osteogenesis imperfecta– autosomal dominant, mutations in the α1 or α2 chain of type 1 collagen– Dissection of cerebral vessels
• Fabry’s disease– X-linked; def α-galactosidase; accumulation of glycosphingolipids in vascular
endothelium– Ischemic stroke 2/3 of infarcts in vertebro-basilar region– Large vessel disease – dotrichoectasia – thrombosis– Widespread small vessel disease; asymptomatic strokes– Cardio-embolic strokes (premature MI or valvular involvement)– Age 21-30– Angiokeratomata, painful acroparaesthesia, renal failure

Estimates of Long-term Risk of Stroke After Ischemic Stroke or TIA
TimeAfter TIA1
(%)
After Stroke2
(%)
30 days 4–8 3–10
1 year 12–13 10–14
5 years 24–29 25–40
Percentage of Patients Experiencing Stroke

A Age ≥60 years 1 point
B Blood pressureSBP >140 mm Hg or DBP ≥90 mm Hg
1 point
C Clinical features Unilateral weakness 2 points
Speech disturbance without weakness
1 point
D Duration of symptoms ≥60 minutes 2 points
10–59 minutes 1 point
D Diabetes Diabetes 1 point
Predicting Risk of Stroke After TIA:
ABCD2 Score for 2- or 7-Day Risk of Stroke

ABCD2 Score Level of Risk2-Day Stroke Risk
(%)
6–7 High 8.1
4–5 Moderate 4.1
0–3 Low 1.0
ABCD2 Is Predictive of 2-Day Risk of Stroke in Patients with TIA

Modifiable risk factors
• Elevated blood pressure
• Diabetes mellitus
• Atrial fibrillation
• Carotid artery disease
• Hyperlipidaemia
• Cigarette smoking
• Obesity
• High alcohol consumption
Summary of risk factors for stroke

Paraplegia or paresis (hemi, mono, quadri)
Hemisensory deficits
Mono or binocular visual loss
Visual field deficits
Diplopia
Dysathria
Facial drooping
Ataxia
Vertigo
Aphasia
Sudden loss of consciousness
PRESENTATIONSymptoms and signs

• Proper history taking• Vital signs:Blood pressure• MAP usually elevated in acute stroke. • Represents response to maintain brain perfusion. • Decision to treat requires balance between severe increases in blood pressure, and decline in neurologic functioning with
decreased BP.
Breathing• Raised ICP (ICH/vertebrobasilar ischemia/ bihemispheric ischemia) - decreased respiratory drive /muscular airway
obstruction.• Hypoventilation (increase in PCO2) - cerebral vasodilation -further elevates ICP.• Intubation- to restore adequate ventilation and protect airway.• Especially in vomiting with increased ICP
Fever • Worsens brain ischemia • Normothermia should be maintained.
DIAGNOSIS

• Absent pulses (inferior extremity, radial, or carotid) - favours atherosclerosis with thrombosis
• Sudden onset of cold, blue limb- favours embolism.• Occlusion of common carotid artery in the neck with bruit -occlusive extra
cranial disease• Temporal arteritis- temporal arteries irregular and with dilatation, tender,
pulseless• Cardiac findings(especially atrial fibrillation, murmurs, cardiac
enlargement) - favour cardiac-origin embolism.• Carotid artery occlusion –iris speckled, ipsilateral pupil dilated and poorly
reactive, retinal ischemia• Fundus - cholesterol crystal, white platelet-fibrin, or red clot emboli.
PHYSICAL EXAMINATION

Transcranial Doppler US• Echocardiography (cardiogenic embolism suspicion)• ECG• CXR• Single-proton emission CT (SPECT) • Conventional angiography (Gold standard for CVD)• Conventional MRI, MRA• noncontrast CT scanning, CTA, CT perfusion scanning• Blood tests (FBC, coagulation studies, cardiac biomarkers)
INVESTIGATION

• ACUTE phase– Ambulance– Emergency room– Neuro-ICU– Stroke Unit
• SUBACUTE phase– Stroke Care ward
• CHRONIC phase– Clinic– Rehabilitation – Domiciliary
MANAGEMENT
• Fibrinolytic therapy: Fibrinolytics restore cerebral blood flow. Recombinant tissue-type plasminogen activator (rt-PA) attempt to establish revascularization so that cells in the penumbra can be rescued before irreversible injury occurs. Should be used 3 hours of onset of stroke & CT scan ruled out hemorrhagic stroke. Not to be used if >80yrs, Hx of stroke or DM, SBP/DBP > 185/110mmHg, head trauma, ICH, INR>1.7, Plt<100,000/µL , Blood glucose< 50mg/dL, Major surgery < 14days etc. E.g: Streptokinase, Urokinase, Alteplase

• Antiplatelet Agent: AHA/ASA guidelines recommend giving aspirin, 325mg orally within 24-48 hours. The benefit of aspirin is modest but statistically significant and appears principally to involve the reduction of recent stroke
• Statins have both neuroprotective as well as neurorestorative effects. Statins improve endothelial function and have anticoagulant, antiinflammatory, and antithrombogenic properties, all of which may foster neuroprotective effects. The antiinflammatory effects of statins suggest that these agents may also be effective when used in combination with thrombolytic therapies, such as with recombinant tissue plasminogen activator, possibly extending the therapeutic window and reducing hemorrhagic transformation.

• Blood pressure control: BP should not be crashed because it is needed for brain perfusion. It should be decreased if the MAP < 140mmHg after 1-2week but if MAP > 140mmHg there should be gradual reduction in the blood pressure. Early lowering of blood pressure with low dose labetalol and Lisinopril slightly improved outcome and did not increase serious adverse events.
• Cerebral edema control: In emergency situations IV 20% mannitol 350ml (10-15mins) then 150ml 6hrly alternate with N/S 500ml 4hrly.
• Anticoagulation and prophylaxis: Patients with embolic stroke who have another indication for anticoagulation (eg, atrial fibrillation) may be placed on anticoagulation therapy nonemergently, with the goal of preventing further embolic disease; however, the potential benefits of that intervention must be weighed against the risk of hemorrhagic transformation. Immobilized stroke patients in particular are at increased risk of developing deep venous thrombosis (DVT) and should receive early efforts to reduce the occurrence of DVT. The use of low-dose, subcutaneous unfractionated or low–molecular-weight heparin may be appropriate in these cases.
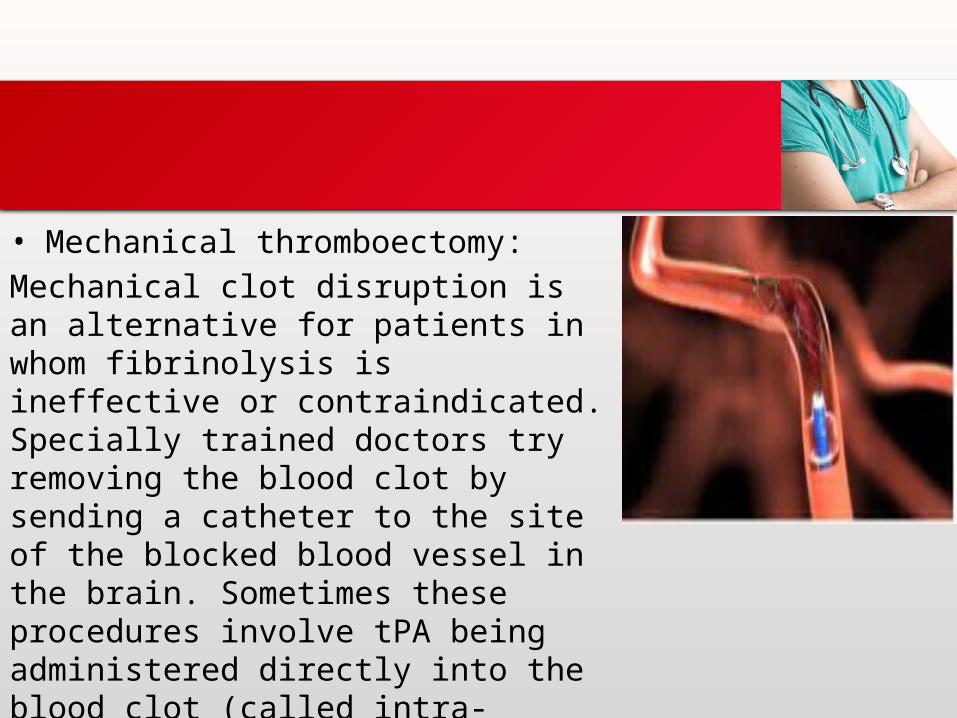
• Mechanical thromboectomy:
Mechanical clot disruption is an alternative for patients in whom fibrinolysis is ineffective or contraindicated. Specially trained doctors try removing the blood clot by sending a catheter to the site of the blocked blood vessel in the brain. Sometimes these procedures involve tPA being administered directly into the blood clot (called intra-arterial treatment) to help dissolve the blockage.

• A: Alcohol/smoking • B: Blood pressure• C: Cholesterol• D: Diet/drugs• E: Exercise
PREVENTION

• F: facial deviation• A: arm or leg weakness• S: slurred speech• T: timing
COMMUNITY IDENTIFICATION

THANK YOU!Спасибо за внимание