Embed Size (px)
Citation preview

Streptococcus Streptococcus pneumoniaepneumoniaeHemophilusHemophilus influenzaeinfluenzae

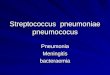
Streptococcus Streptococcus pneumoniaepneumoniae

Introduction
• gram positive lanceolate diplococci• Resemble viridans streptococci• Are normal inhabitants of upper RT• Cause pneumonia & otitis media in children• was first isolated simultaneously and
independently by the U.S. Army physician George Sternberg and the French chemist Louis Pasteur

Morphology• Gram positive diplococci• alpha-hemolytic, facultative anaerobic
member of the genus Streptococcus. • Individual cocci
– 1 um– Lanceolate in appearance
• Capsulated• Nonmotile• Non sporing• Non acid fast


Culture characteristics• Aerobe & facultative• Optimum temp. 37 o C ( 25 – 42 o C
)• Optimum PH – 7.6 ( 6.5 – 8.3)• Grow only in enriched media• Growth is improved by 5- 10 % co2

Characteristics ( contd..)• Glucose/ serum broth:
– Produce uniform turbidity– No pellicle formation– After 36 hours autolysis occurs
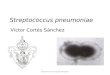
• Blood Agar: after 18 hours at 37o C• Small (0.5 to 1)• Round• Entire• Convex• With an area of greenish discolouration around them• On further incubation the colonies become flat with raised
edges and central depression, so that concentric rings are seen on the surface when viewed from above(draughtsman or carrom coin appearance)

“draughtsman” apperance

Biochemical reactions• Catalase- -ve• Oxidase- -ve• Ferment several sugars• Ferment inulin• Are bile soluble

Serotypes• Based on capsular polysaccharides
• More than 90 different serotypes are known
• these types differ in virulence, prevalence, and extent of drug resistance

• Toxins:Hemolysin (Pneumolysin O) and leucocidin
• Capsular polysaccharide– Protects the cocci from phagocytosis
virulence factors

Other virulence factors
• Ig A1 protease
• Protein adhesin
• Cell wall constituents

transmission• methods include
– sneezing, – coughing, and– direct contact with an infected
person.

Diseases• Pneumonia
– Lobar pneumonia (localised in the lower lobes of the lung) (more than 80% of cases)
– Broncho pneumonia (patchy involvment of the lung)
• bacteremia/septicaemia • meningitis• Conjuctivitis• Suppurative lesions:
– Otitis media– Paranasal Sinusitis

Diseases contd
• osteomyelitis, • septic arthritis, • endocarditis, • peritonitis, • cellulitis and• brain abscesses.• currently the leading cause of invasive
bacterial disease in children and the elderly.• Pneumonia and otitis media are the most
common infections


Symptoms of pneumococcal disease•depend on the part of the body that is infected.
•include fever, cough, shortness of breath, chest pain, stiff neck, disorientation, sensitivity to light, joint pain, chills, ear pain, sleeplessness, and irritability.
• In severe cases, pneumococcal disease can cause hearing loss, brain damage, and death.

Diagnosis• Laboratory diagnosis• Imaging

Laboratory diagnosis• Specimens
• Microscopic Examination
• Culture
• Serological test
• Animal pathogenicity test

Potential specimen• Blood• Cerebrospinal fluid• Sputum• Pleural fluid or lung aspirate• Joint fluid• Bone• Other abscess or tissue specimens

Gram Stain of a film of sputum from a case of lobar pneumonia

Culture• Culture in enriched media• Routinely in Blood agar with 5-10
% Carbondioxide• Alphahemolytic colony noted

Identification: Optochin sensitivity test

Quellung (capsular swelling) reaction/ serotyping

Bile solubility test

Animal pathogenecity• Highly pathogenic for mice and rabbits but less
for guinea pig.• Intraperitoneal inoculation (0.5) of homogenised
specimen of sputum or others leads to fatal infection
• Mice-intraperitoneally when injected die within 24 hrs
• Mice-intracerebally when injected die within 6 hrs• Organisms found in predominance in peritoneal
exudate and heart blood

• Other laboratory values that may be helpful in diagnosis and treatment include the following:– Complete blood count and differential– Erythrocyte sedimentation rate (ESR)– C-reactive protein (CRP)

Imaging studies• Chest radiography• Ultrasonography of the chest• Computed tomography (CT) of the chest,
sinuses, face, or affected bones or joints• Magnetic resonance imaging (MRI) of the
brain (in meningitis) or affected bones and joints

Griffith Tranformation

Prophylaxis
• A polysaccharide vaccine containing 23 serotypes is available
• Useful •for children above 2 years of age•Elderly , debilited &
immunosuppressed•Contraindicated in pts with
Lymphomas & children under 2 year

Treatment• Penicillin:
– the drug of choice for many years– Until recently 10 -15 % resistant strains– Therefore AST should be done
• Other antibiotics:– Cephalosporins– Erythromycin– Chloramphenicol– Vancomycin –for highly resistant strains

Pneumococcus Vs other Streptococci
• Morphology• Quellung test• Colony
characteristics• Growth in liquid
media• Bile solubility
• Inulin fermentation
• Optochin sensitivity
• Intraperitoneal inoculation in mice (Mouse pathogenicity test)

properties Pneumococcus Viridians strepto.Morphology Capsulated,lanceolate-
shaped diplococciNon-capsulated,oval or round cells in short chains
Colony on BA Raised/flat initially later “draughtsman”
Dome-shaped
Broth culture Uniform turbidity granularwith powdery deposit
Bile solubility test + -Optochin sensitivity Sensitive Resistant
Inulin fermentation ferments Donot
Quellung reaction + -Mice/rabbbit pathogenicity
pathogenic Non -pathogenic

Hemophilus Hemophilus influenzaeinfluenzae

Definition• Haemophilus influenzae (formerly called
Pfeiffer's bacillus or Bacillus influenzae) is a Gram-negative, coccobacillary, facultatively anaerobic pathogenic bacterium belonging to the Pasteurellaceae family.
• H. influenzae was first described in 1892 by Richard Pfeiffer during an influenza pandemic
• Greek haemal, blood; philos, friendly)• present in the nasopharynx of approximately 75
percent of healthy children and adults.

Haemophilus influenzae• gram-negative coccobacillus(short rod) and long
filamentous form in CSF in meningitis.• 0.2 to 0.3 to 0.5 to 0.8 um• Nonmotile, nonsporing pleomorphic• Oxidase positive• aerobic and facultative anaerobe.• In vitro growth requires accessory growth factors,
including “X” factor (hemin) and “V” factor (nicotinamide adenine dinucleotide [NAD]).
• Chocolate agar media are used for isolation. H. influenzae will generally not grow on blood agar, which lacks NAD.

Special media• Levanthal agar• Filde’s peptic digest• Brain and Heart Infusion broth
with hemin and nicotinamide supplements

Satellitism• H. influenzae will grow in the hemolytic zone
of Staphylococcus aureus on blood agar plates; the hemolysis of cells by S. aureus releases factor V which is needed for its growth. H. influenzae will not grow outside the hemolytic zone of S. aureus due to the lack of nutrients such as factor V in these areas.

Classification/Serotypes• In 1930, two major categories of H. influenzae were
defined: the unencapsulated strains and the encapsulated strains.
• Encapsulated strains (typeable)– The outermost structure of encapsulated H. influenzae
is composed of polyribosyl-ribitolphosphate (PRP), a polysaccharide that is responsible for virulence and immunity.
– on the basis of distinct capsular antigens six types : a, b, c, d, e, and f.
– 95% of invasive disease caused by type b (prevaccine)

• Unencapsulated strains (also termed nontypeable (NTHi) lack capsular serotypes
– less invasive; they can, however, produce an inflammatory response in humans

Diseases• Most strains usually live in host without causing disease
• but other factors (such as a viral infection, mycoplasma, reduced immune function or chronically inflamed tissues, e.g. from allergies) create an opportunity.
• infect the host by sticking to the host cell using trimeric autotransporter adhesins

• H. influenzae type b (Hib) – In infants and young children,
causes bacteremia, pneumonia, epiglottitis and acute bacterial meningitis.
– On occasion, it causes cellulitis, osteomyelitis, and infectious arthritis.

• Unencapsulated H. influenzae strains: – cause invasive disease similar to type b
infections but less virulent than encapsulated strains
– are unaffected by the Hib vaccine – cause ear infections (otitis media), eye
infections (conjunctivitis), and sinusitis in children, and are associated with pneumonia.
– bronchitis in adults.

Virulence • no exotoxins • neuraminidase and an IgA protease• Fimbriae adherence to human mucosal cells • capsular polysaccharide, (polyribosyl ribitol
phosphate (PRP) capsule )– antiphagocytic, ineffective complement-mediated bacteriolysis.

Diagnosis
• Laboratory testing• Imaging studies

Laboratory diagnosis
• Specimens: – CSF, blood, pleural fluid, joint fluid,
and middle ear aspirates should be cultured on Chocolate agar

Gram staining of body fluids from various sites of infection

Culture• chocolate agar, with added X (
hemin) and V (nicotinamide adenine dinucleotide) factors at 37 °C in a CO2-enriched incubator – convex, smooth, pale, grey or
transparent colonies.• Fildes agar is best for isolation.• In Levinthal medium, capsulated
strains show distinctive iridescence.

X and V factors requirements
• Haemophilus influenzae requires X and V factors for growth. In this culture haemophilus has only grown around the paper disc that has been impregnated with X and V factors. There is no bacterial growth around the discs that only contain either X or V factor.

Immunological test– Detection of the polyribosyl ribitol phosphate
(PRP) polysaccharide capsule • countercurrent immunoelectrophoresis,• latex particle agglutination,• co-agglutination, and enzyme-linked
immunosorbent assay
– The most confirmatory method of establishing the diagnosis; slide agglutination with type-specific antisera

Laboratory testing• Others
• Acute phase reactants:– Characteristic elevated erythrocyte sedimentation
rates (ESRs) and C-reactive protein (CRP) levels in patients with septic arthritis

Molecular methods– Polymerase chain reaction (PCR) – Countercurrent
immunoelectrophoresis•

Imaging studies• Computed tomography (CT) scanning of the
head• • Chest radiography: For suspected pulmonary
disease (eg, pneumonia)
• Lateral neck radiography: To confirm epiglottitis
• • Echocardiography: For suspected pericarditis

Treatment• A combined therapy with ampicillin plus
chloramphenicol or third generations cephlosporine(Cefotaxime/ceftriaxone)
• Fluoroquinolones• Macrolide antibiotics (e.g., clarithromycin)
may be used in patients with a history of allergy to beta-lactam antibiotics

Prevention• Effective vaccines for Haemophilus influenzae
Type B have been available since the early 1990s, and is recommended for children under age 5 and asplenic patients.
• World Health Organization recommends a pentavalent vaccine, combining vaccines against diphtheria, tetanus, pertussis, hepatitis B and Hib.

• Doses of Hib vaccine are usually recommended at these ages:– First Dose: 2 months of age – Second Dose: 4 months of age – Third Dose: 6 months of
age (if needed, depending on brand of vaccine)
– Final/Booster Dose: 12–15 months of age– Children over 5 years old and adults usually
do not need Hib vaccine.

Haemophilus influenzae type b
Epidemiology• Occurrence: worldwide• Reservoir : human –asymptomatic carriers• Transmission : commonly respiratory droplets
– neonates • aspiration of amniotic fluid • genital track secretions during delivery
• Temporal pattern : peaks in Sept-Dec and March-May
• Communicability - generally limited but higher in some circumstances

Thank You