Embed Size (px)
Citation preview
SPRING CATARRAH
BY: YOHANANTH SIVANANTHANROLL NO:132
NEPALGUNJ MEDICAL COLLEGENEPAL
AUG 10 BATCHOPTHALMOLOGY SEMINAR SERIES
VERNAL KERATOCONJUNCTIVITIS[SPRING CATARRH]
It is a recurrent, bilateral, interstitial, self limiting allergic inflammation of the conjunctiva may have a periodic seasonal incidence.
It is a type of allergic conjunctivitis. Occuring with the onset of hotweather,
during summer rather than spring. Sporadic and non contagious in nature. Recently it also called as warm weather
conjunctivitis.
INCIDENCE Sporadically occur in wide geographical
incidence. More common in indian subcontinent and
africa like tropical countries than europe. Coloured races are more prone to form
limbal form of disease. Essentially disease of youth occuring more
frequently in between ages of 5-10 years. Sex incidence very high pecentages are
seen in males Family history of allergy found in 40-60
percentages.
ETIOLOGY Three theories are found currently
Due to the action of physical factors like Heat Humidity Light
Due to the endocrine glands and vagotonic states Manifestation of an allegic condition.
Pollens Toxins Dusts Animal debris,hair Inhalants Injestants
Mostly pathogenesis IgE mediated allegic reaction
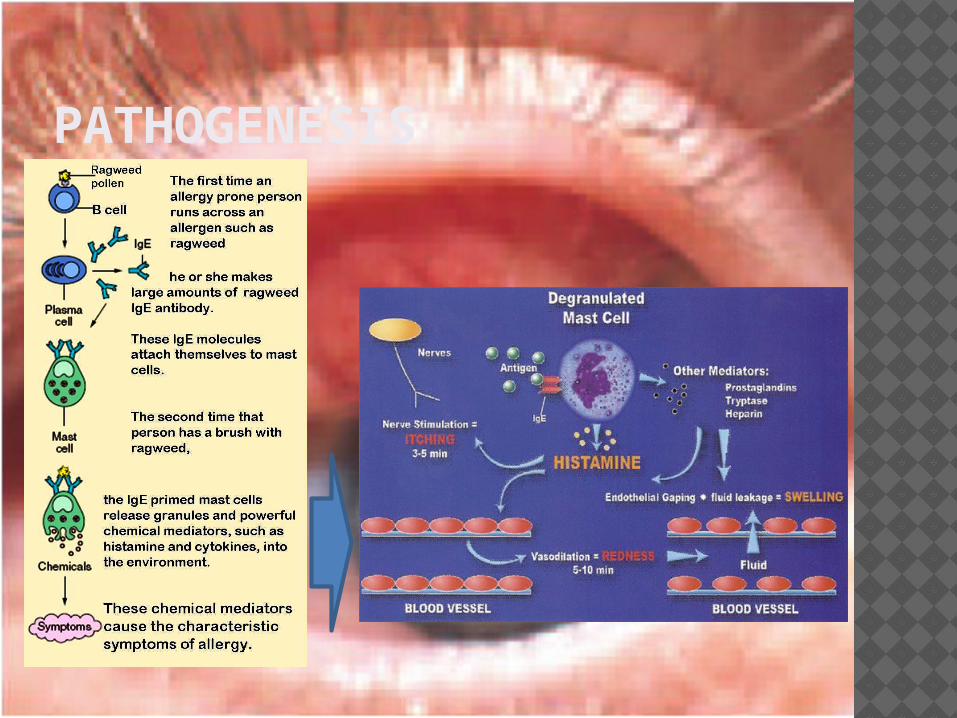
PATHOGENESIS

PATHOLOGY Conjunctval epithelium
Undergoes hyperplasia Sends downwards projections into the sub epithelial
tissue Adenoid layer
Marked cellular infiltrations Eosinophils, plasmacells, lymphocytes,and histiocytes
Fibrous layer Shows proliferation Later on undergoes hyaline changes
Conjunctival vessels Proliferation Increased permeability and vasodilation. All these lead to formation of multiple papillae in the
upper tarsal conjunctiva…
SYMPTOMS Marked burning and foreignbody sensation. Itching sensation. Mild photophobia. Lacrimation+watering Stringy( thick ropy white) discharge and
heaviness of lids.
in the cooler months the conditions subsides and symptoms persits and is symptomsless although the lesions persists,but recur with the return of the heat.

SIGNS Signs may be described under 3 clinical
forms of disease
Palperbral form
Bulbar form
Mixed form

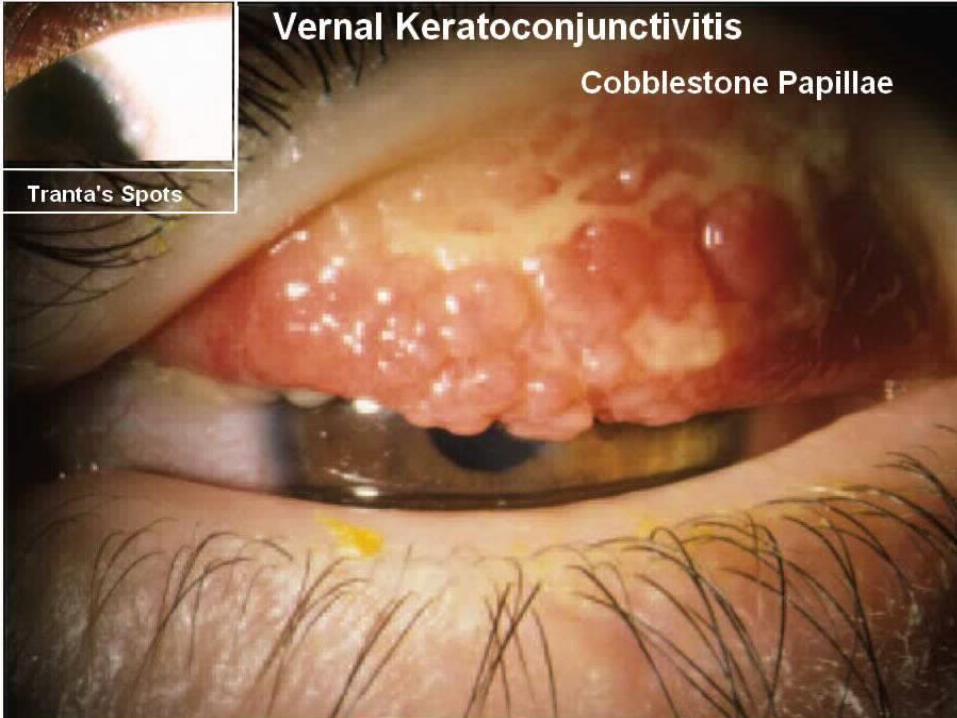
PALPERBRAL FORM Usually upper tarsal conjunctiva of
both eyes involved. Easily recognised On everting upper lid the palperbral
conjunctiva is seen to be hypertropied and mapped out into polygonal raised are like cobblestones or pavement stones fashion.
In severe cases papillae may hypertropy-produce giant papillae,cauliflower like excresenses.
The colour is bluish white,like milk,and this apppearancce may also be seen over the lower palperbral conjunctiva.
The flat topped nodules are hard consist cheifly of dense fibrous tissue,but the epithelium over them thickned giving rise to milky hue.
Histologically they are hypertrophied papillae not follicles
Eosinophillic leukocytes are present in them in great numbers and found in the secretion
Infiltrationof lymphocytes,plasmacells,macrophages,basophills.
Palperbral form cannot be mistaked if typical but may resemble trachoma.
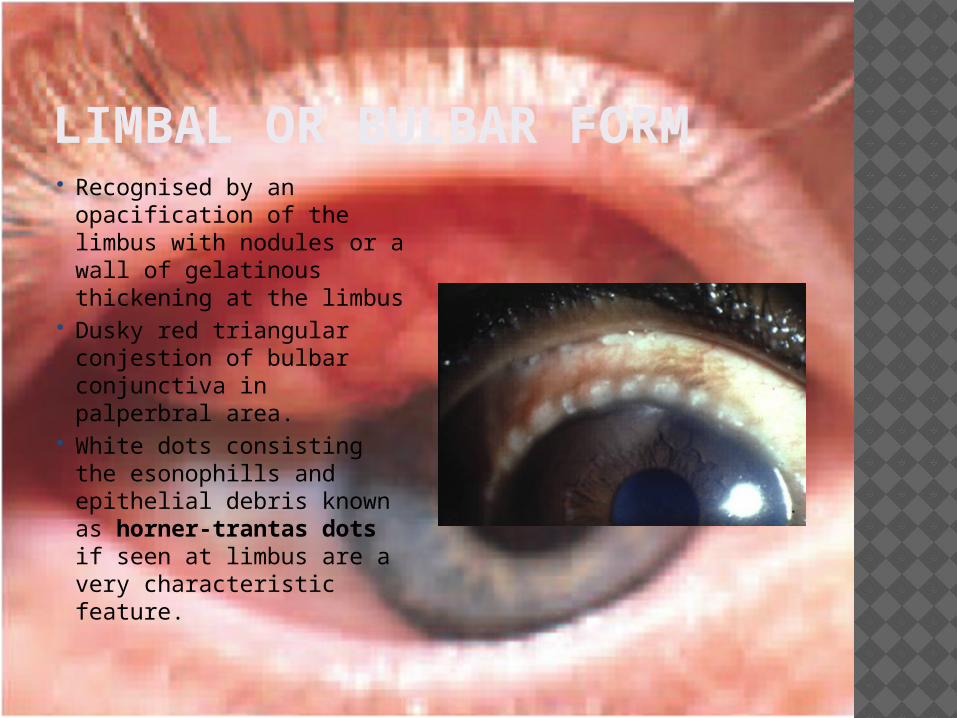
LIMBAL OR BULBAR FORM Recognised by an
opacification of the limbus with nodules or a wall of gelatinous thickening at the limbus
Dusky red triangular conjestion of bulbar conjunctiva in palperbral area.
White dots consisting the esonophills and epithelial debris known as horner-trantas dots if seen at limbus are a very characteristic feature.


MIXED FORM It shows combined features of both
palperbral and bulbar form

COMPLICATIONS Mainly due to corneal involvement
otherwise prognosis is good
Vernal keratopathy Due to corneal involvement in vernal
kerato conjunctivitis May be primary or secondary due to
extension of limbal lesions. Includes 5 types of lesions

PUNCTATE EPITHELIAL KERATITIS INVOLVE UPPER CORNEA MOSTLY WITH PALPERBRAL FORM STAIN WITH ROSEBENGAL INVARIABLY WITH
FLOURESCEIN ULCERATIVE VERNAL KERATITIS
SHALLOW TRANSVERSE ULCER IN UPPER CORNEA VERNAL CORNEAL PLAQUES
DUE TO COATING OF BARE AREAS OF EPITHELIAL MACRO EROSIONS WITH A LAYER OF ALTERED EXUDATES
SUBEPITHELIAL SCARRING IN A FORM OF RING SCAR
PSEUDOGERONTOXON. CHARACTERISED BY CUPID BOW OUTLINE.


CLINICAL COURSE SELF LIMITING USUALLY BURNS OUT SPONTANEOUSLY
AFTER 5 TO 10 YEARS.

DIFFERENTIAL DIAGNOSIS TRACHOMA
Mainly trachoma with predominant papillary hypertrophy from palperbralform of spring catarrah
It can be differentiated as follows
Papillae are large and usually cobblestone appearance in spring catarrah.
Ph of tears alkaline in spring catarrah while in trachoma acidic.
Discharge ropy in spring catarrah
Conjunctival cytology and labtest in difficult cases.

TREATMENT Local therapy
Topical steroids. Used for all type of spring
catarrah Beware of steroid induced
glucoma in prolonged use Measure IOP during
treatment Frequent instillation 4 houly
for 2days, then 3-4times a day for 2 weeks
Fluorometholone medrysone.
Betamethosone. Dextramethosone Medrysone and
flurometholone are most safest.

Local theraphy Mast cell stabilizers.
Sodium chromoglycate 2% drops 4-5 times a day
Topical antihistaminics. Acetyl cysteine 0.5%
Mucolytic properties In early plaque formation
Topical cyclosporine 1% In un responsible cases Steroid resistant cases.

Systemic therapyOral antihistamininics
Anti allergic Relive from itching
Oral steroids Short duration recommended for advanced,very
severe non responsive cases.

Treatment for large papillae. Giant papillae can be tackled by
Supratarsal injection of long acting steroids. Cryo application Sugical excision recommended for extra ordinary large papillae
General measures Dark goggles for photophobia Coldcompression for soothing effect Change of place to hot to cold area if possible
Desensitization Treatment for vernal keratopathy
Punctate epithilial type-no extra treatment instillation of steroid must be increased.
Large vernal plaque-surgery(superficial keratectomy) Severe shied ulcer-resistant to medical theraphy
Sugery is preffered in debridement,superficial keratectomy,eximer laser,therapeutic keratectomy.
Prophylaxisbeta radiation,disodium chromoglycate 2% 3 to 4 times.