Embed Size (px)
Citation preview

The Somatosensory System Csilla Egri, KIN 306 Spring 2012
“Activate my mechanoreceptive free nerve endings and Pacinian corpuscles” Elmo
Outline
Somatosensory system overview Sensory transduction Sensory receptors
Cutaneous mechanoreceptors Thermoreceptors Nociceptors
Central projections Dorsal column medial-lemniscus pathway Anterolateral pathway
Pain sensations Pain disorders
2
Somatosensory system: function
3
Receptors respond to mechanical, thermal & chemical stimuli within three broad categories: Proprioceptive (lecture 6,10)
Body and limb position Enteroreceptive (KIN 305)
Internal state of the body Exteroreceptive
Touch Temperature Pain (nociception)

Somatosensory fibers4
Afferent fibers carrying info of different modalities are of different sizes
What property of large diameter axons allows for increased speed of
conduction?

Somatosensory transduction 5
two classes: simple or complex mechanical deformation, heat or
chemical stimulus within receptive field opens ion channels causes a local depolarization
= receptor potential propagated by electrotonic
conduction to axon hillock Stimulus intensity coded by
number of receptors activated, and frequency of AP
Receptor potential
Somatosensory transduction 6
How to convey modality of sensation? Labelled line coding
Type of sensation felt when receptor is stimulated determined by where the fiber synapses in the CNS
Examples of “fooled” senses: Chewing minty gum activates cold sensitive
thermoreceptors sensation of cold Seeing stars after being hit on head forceful blow
activates photoreceptors see spots

Cutaneous mechanoreceptors: morphology
7
(rapid vibration)
(slow vibration, texture)
(rapid vibration)
(deep pressure)
(movement of hairs)
(sustained touch, pressure)
Cutaneous mechanoreceptors: adaptation
8
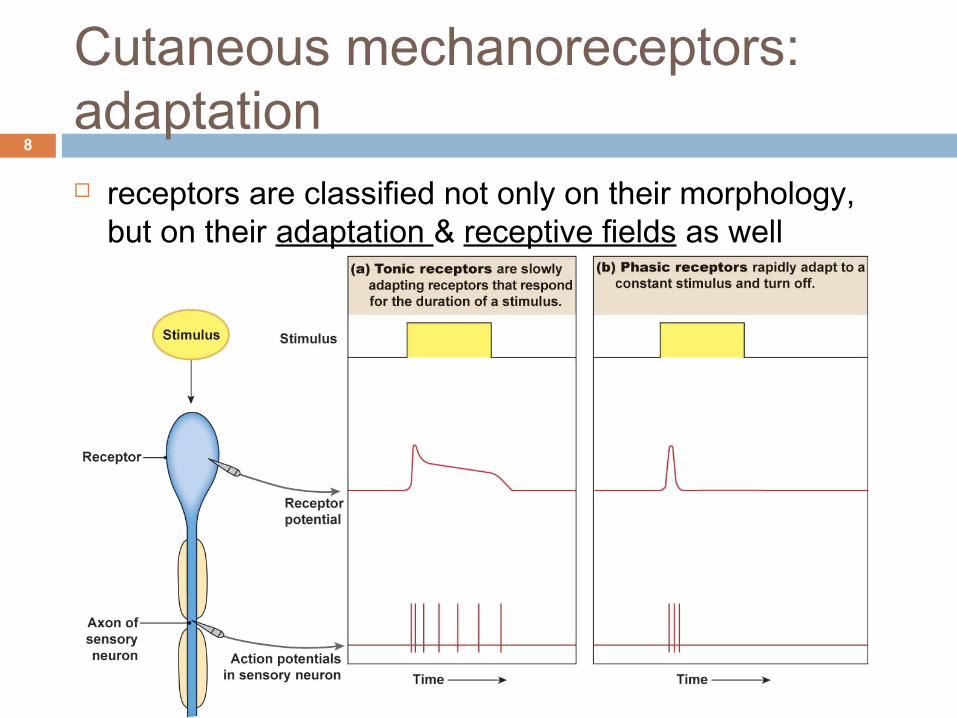
receptors are classified not only on their morphology, but on their adaptation & receptive fields as well

Cutaneous mechanoreceptors: receptive fields
9
small receptive fields permit high resolution of spatial detail (two point discrimination)
Discrimination enhanced by lateral inhibition

Cutaneous mechanoreceptors: adaptation + receptive fields
10
Kandel Fig. 21-1
Adaptation
Cutaneous mechanoreceptors: summary
11
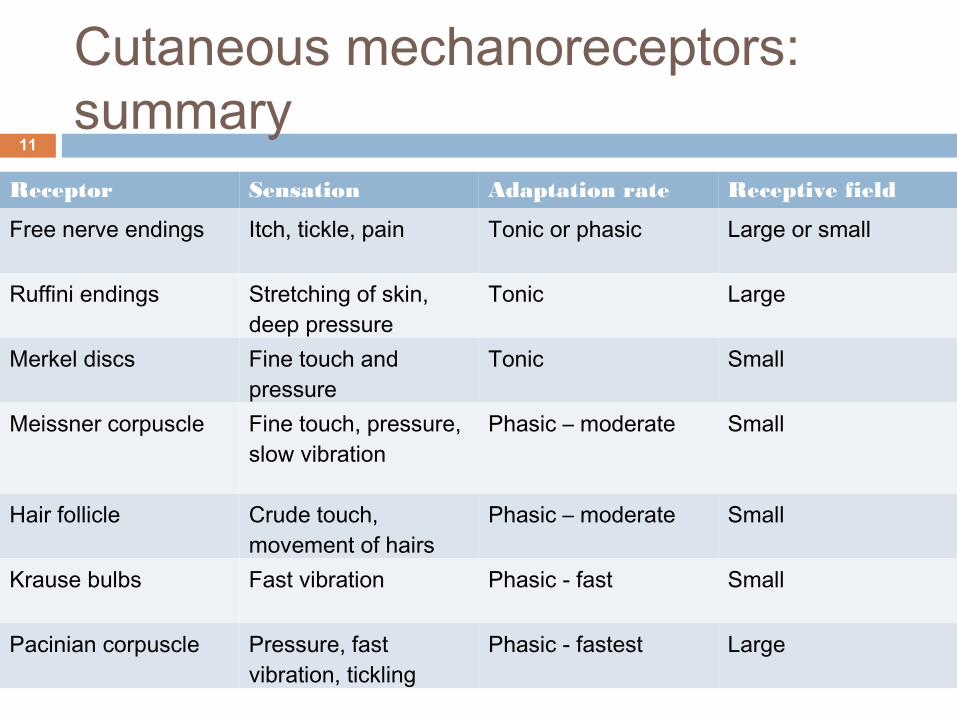
Receptor Sensation Adaptation rate Receptive field
Free nerve endings Itch, tickle, pain Tonic or phasic Large or small
Ruffini endings Stretching of skin, deep pressure
Tonic Large
Merkel discs Fine touch and pressure
Tonic Small
Meissner corpuscle Fine touch, pressure, slow vibration
Phasic – moderate Small
Hair follicle Crude touch, movement of hairs
Phasic – moderate Small
Krause bulbs Fast vibration Phasic - fast Small
Pacinian corpuscle Pressure, fast vibration, tickling
Phasic - fastest Large

Thermoreceptors12
Free nerve endings with high thermal sensitivity Temperature change activates family of ion channels on the
receptor membrane = TRP (transient receptor potential) channels
Each TRP channel has a unique temperature threshold of firing, and is sensitive to various chemical agonists
Thermoreceptors: tonic responses
13
Guyton Fig. 48-10
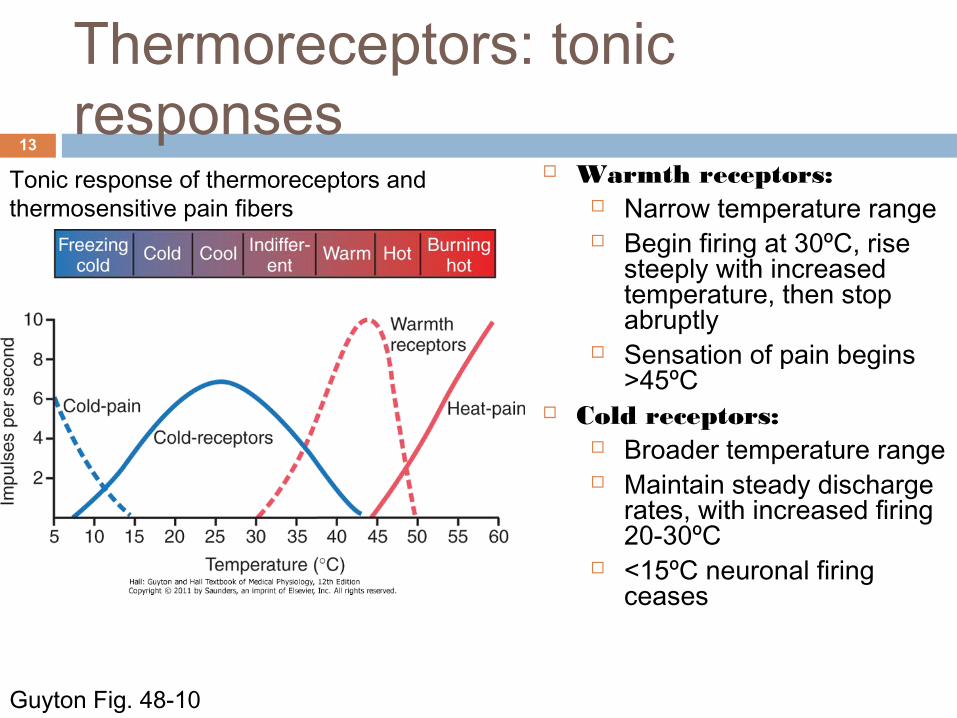
Warmth receptors: Narrow temperature range Begin firing at 30ºC, rise
steeply with increased temperature, then stop abruptly
Sensation of pain begins >45ºC
Cold receptors: Broader temperature range Maintain steady discharge
rates, with increased firing 20-30ºC
<15ºC neuronal firing ceases
Tonic response of thermoreceptors and thermosensitive pain fibers

Thermoreceptors: phasic responses
14
Kandel Fig. 22-9
Thermoreceptors are more responsive to changes in temperature than to constant temperature
A phasic response in both warm and cold receptors occurs when the temperature is changed
Thermoreceptors adapt to a new steady state firing level is stimulus is maintained

Nociceptors15
Free nerve endings that respond to intense stimuli Types:
Mechanical Strong pressure, sharp objects
Thermal Burning heat (>45ºC) Noxious cold (variable)
Chemical pH extremes Environmental irritants Internal neuroactive substances
Polymodal Sensations mediated by Aδ fibers (sharp, intense pain) and C fibers
(persistent, dull pain).
Check: Which fibers are myelinated?

Nociceptors: hyperalgesia of inflammation
16
Nociceptors are non adapting receptors Primary hyperalgesia: damaged tissue
has increased sensitivity to pain Reduced threshold to pain
If normally non painful stimuli felt as painful: allodynia
Increased intensity of sensation Spontaneous pain
Inflammatory response releases bradykinin, prostaglandins, serotonin, substance P, K+, H+
Substance P activates mast cells release histamine activates nociceptors
B&B Fig. 13-26

Somatosensory projections: dermatomes
17
Sensory neurons (dorsal root ganglion cells) enter the spinal cord through the dorsal roots
Each dorsal root innervates a field of skin called a dermatome
Dermatomal map used to determine level of lesion of spinal injury
Epidural analgesia blocks sensations thru out several dermatomes
B&L Fig. 7-4

Somatosensory projections: tracts
18
2. Anterolateral pathway1. Dorsal column-medial lemniscus pathway

1. Dorsal column-medial lemniscus pathway
19
Carry signals from mechanoreceptors of the skin, joints & muscle fine, discriminatory touch
Information has high spatial & temporal resolution Large, myelinated fibers with rapid conduction velocities 1º afferents terminate & form synaptic connections with
2nd order neurons in the dorsal column nuclei within the medulla
2nd order neurons cross over at the medulla and continue to the thalamus via the medial lemniscus pathway
After thalamic processing, 3rd order neurons project to the primary somatosensory cortex

2. Anterolateral pathway20
Pain, temperature, crude touch, tickle, itch, sexual sensations
Low spatial or temporal resolution Small, myelinated/unmyelinated fibers with slower
conduction velocities 1° afferents terminate upon entering spinal cord &
synapse on 2nd order neurons 2nd order neurons cross to contralateral side, ascend to
brain via anterolateral quadrant in spinal cord & project to thalamic nuclei
After thalamic processing, 3rd order neurons project to the primary somatosensory cortex and other cortical areas

Somatosensory cortex: somatotopy
21
B&B Fig. 14-11
Spatial orientation of signals form different parts of the body: somatotopy
Size of somatotopic areas is proportional to density of sensory receptors in that body region
Map is plastic (modifiable) size of cortical region representing
particular portion of body surface can expand or contract depending on use of that body region
Pain and temperature localization not as precise Integration probably happens more in
the reticular formation and thalamus

Pain sensation: referred pain22
Pain from visceral nociceptors is poorly localized, can be felt as pain on surface areas Knowledge of referred pain maps important in clinical diagnosis Somatic and visceral afferents may converge on same 2nd order neuron
Guyton Fig. 48-6Kandel Fig. 24-3

Pain sensation23
Sensation of pain intensity not necessarily linked to activation of nociceptors; under CNS control Perception of pain and pain tolerance is subjective Gate control theory of pain
Activation of non-painful fibers (Aα) sends inhibitory signals to nociceptive afferents traveling to the CNS
Mechanism of acupressure analgesia? Phantom limb pain
Pain felt even though nociceptors no longer present in missing limb Peripheral sensitization Somatosensory reorganization
Neuropathic pain Damage to Aδ or C fibers may increase sensitivity or cause
spontaneous AP firing

Pain disorders: CRPS24
Complex regional pain syndrome (CRPS) Neuropathic pain disorder involving peripheral
and central mechanisms (autonomic nervous system)
Changes in somatosensory systems processing thermal, tactile, noxious stimuli Local edema, altered sweating, redness,
skin temperature changes, burning pain, hyperalgesia, allodynia
Acute: warm, red extremities Chronic: cool, bluish extremities
CRPS I – no documented nerve injury CRPS II – presence of nerve injury
Surgery, fracture, crush injury, sprains, but can develop even after minimal injury
WebCT readings: Complex Pain Syndrome
Left arm affected by CRPS
Right foot affected by CRPS

Pain disorders: CRPS pathophysiology
25
Peripheral and central sensitization Tissue injury release of substance P and
bradykinin increased excitability of nociceptive neurons in periphery and spinal cord
Increased local, systemic, and CSF inflammatory factors
Reduced density of Aδ and C fibers Altered SNS function and sympatho-afferent
coupling Expression of adrenergic receptors on
nociceptors Symptoms worsened by emotional arousal Reduced representation of affected limb in
somatosensory cortex Genetic predisposition
Increased susceptibility to above mentioned changes?
Bruehl S. Anesthesiology 2010WebCT readings: Complex Pain Syndrome

ObjectivesAfter this lecture you should be able to: List the structure and function of the various cutaneous
mechanoreceptors Describe the mechanism of somatosensory transduction,
including modality coding and receptor adaptation Differentiate between tonic and phasic responses of
thermoreceptors Compare and contrast the function and anatomy of the dorsal
column-medial lemniscus pathway with the anterolateral pathway
List the factors affecting pain sensation Relate what we’ve learned in this course so far to the different
theories of CRPS pathophysiology
26

27
1. Predict on which side of the body and what sensations would be impaired if there was a spinal cord transection at T4 of:
a) The left dorsal column-medial lemniscus pathwayb) The left anterolateral pathway
2. Describe what would happen to both cold and warm thermoreceptors in response to an increase in temperature from 35ºC to 40ºC , sustained for 5 min, and removed.
3. Meissners corpuscles are __________________ adapting receptors with __________________ receptive fields.
Test your knowledge