Embed Size (px)
Citation preview

SMALLPOXA DEAD DISEASE
Dr.T.V.Rao MD

Small Pox - Variola
Variola - Small pox
• WHO 1977 ended
• 8th May 1980 WHO declares Global eradication
• Most Fatal – Small pox Variola Major
• Non fatal - Alastrim – Variola minor
• Vaccine – Virus – Cow pox used for vaccination
• Vaccina – Viral vector.

Origin of Smallpox
• The name Variola was first used in the 6th century. Derived from the Latin word varius (spotted) or varus (pimple).
• Anglo-Saxons in the 10th century used the word poc or pocca (bag or pouch) to describe an exanthemous disease, possibly smallpox.
• In the 15th century, the English used the prefix small to distinguish variola the smallpox from syphilis, the great pox.

First Case of Smallpox• There is no animal
reservoir, and no human carriers.
• First certain evidence comes from the mummified remains of Ramses. (1157 B.C.)
• Written descriptions did not appear until the 10th century in Southwestern Asia.

History of Variolation and Vaccine
• Known that survivors became immune to the disease.
• As a result, physicians intentionally infected healthy persons with smallpox organisms.
• Variolation is the act of taking samples (pus from pustules or ground scabs) from patients whose disease had been benign, and introducing it into others through the nose or skin.

Species of the Genus Orthopoxvirus
Species Animals Infected Host Range Geographic Range
Variola Human Narrow Formerly worldwide
Vaccinia Human,a cow, pig, buffalo, rabbit, etc. Broad Worldwideb
Cowpox Rodent,a cow, human, cat, etc. Broad Europe
Monkeypox Squirrel,a monkey, ape, human Broad Western and central Africa
Ectromelia Mouse, mole Narrow Europe
Camelpox Camel Narrow Africa and Asia
Taterapox Gerbil Narrow Western Africa
Volepox Vole ? United States
Raccoonpox Raccoon ? United States
Skunkpox Skunk ? United States
Uasin Gishu Horse Medium Eastern Africa
aPrimary host.bSecondary to vaccination; no known natural host.
http://books.nap.edu/html/variola_virus/ch2.html#TopOfPage

SMALLPOX• Genus Orthopoxviruses
Smallpox, monkey pox, cowpox,vaccinia
• DNA Virus• 200 nm brick
shaped
• Smallpox-person to person spread via respiratory secretions/direct contact
• Spread best in low humidity/temperature

CHARACTERISTICS SHARED BYSPECIES OF ORTHOPOXVIRUS :
- - The largest and most complex virusesThe largest and most complex viruses- Virons particles can be seen with a light Virons particles can be seen with a light microscopemicroscope
- They contain a linear genome of a single- They contain a linear genome of a single double-stranded DNA double-stranded DNA - They replicate in the cytoplasm of the They replicate in the cytoplasm of the host cell, host cell, DNA synthetic machineryDNA synthetic machinery (including DNA-dependent RNA (including DNA-dependent RNA polymerasepolymerase
- Serological cross-reactivitySerological cross-reactivity- Produce a hemagglutininin antigen (HA)- Produce a hemagglutininin antigen (HA)

Guarnieri's bodies or Elementary bodies
• Inclusion bodies: type A and type B
• Virions have a brick-like shape and are present in 2 forms, both are infectious

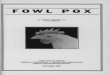
VacciniaVaccinia Virus – Electron micrographsVirus – Electron micrographs
A. Non- enveloped virion (surface of outer membrane with tubular elements)C. Thin section of non-enveloped virion (biconcave core)B. Enveloped virion, found in extracellular mediumD. Viral core, released after treatment of virions with Nonidet
Fenner,F. et al. Smallpox and Its Eradiction. Genevea, Switzerland:WHO. 1998:1460

Variola virus• Brick shaped,cosists
of double layered membrane which surrounds – Biconcave –Nucleoid congaing DNA core
• Either side lens shaped lateral body
300 x 200 x 100 nm


Physical characters
• Remain viable for months at room temperature
• Resists 50% Glycerin and 1 % phenol
• Inactivated by formalin and oxidizing agents

Antigenic structure• Nearly 20 antigen• Heat liable and stable antigens• Cultured on Chorioallontoic membrane of 11
– 13 days old chick embryo• Variola pocks are small shiny, white convex
non necrotic, non hemorrhagic • Variola pocks are larger irregular flat grayish
necrotic lesions some are hemorrhagic• Tissue culture on Monkey kidney, Hela cells

Virus spread by respiratory route

Variola (Smallpox)
Smallpox is an acute exanthematous disease caused by infection with the poxvirus variola.
The significant clinical features include:
Three-day prodromal illness characterized by fever, headache, backache, and vomiting. Generalized centrifugal rash that follows prodrome
Begins centrally then spreads to the extremities and face Rapid succession of papules, vesicles, pustules, umbilication, and crusting over a 14-day period.
Prior vaccination may alter the clinical presentation of smallpox. The following description applies to the classic presentation in unvaccinated individuals.

Variola (Smallpox) View Table
A macular red rash may precede the appearance of the papules, which are deep and firm to palpation. Papules soon vesiculate, forming a circumscribed, elevated lesion that contains clear fluid.
Central umbilication of the pustule is characteristic of smallpox. A second important distinguishing characteristic of smallpox is that all of the lesions at a given time are in the same stage of development. That is, at any one point in time the lesions are all papules or vesicles or pustules. Bacterial infection of the lesions can occur, producing localized abscesses and cellulitis.

Variola (Smallpox) View Table
Chart from the Center for Disease Control and Prevention showing the characteristic distribution of smallpox lesions.


Variola (Smallpox)View Table
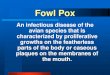
Smallpox on the hand: Notice how these lesions have become confluent.

Variola (Smallpox) View Table
Smallpox in a child: Notice that all lesions are in the same stage of development.


Small pox• Last case Saiban Bibi Assam 24
may 1977• Patients are source of infection • Close contacts• Single crop centrifugal distribution• Macules – Papules – Vesicles –
Pustules

Pathogenesis of Smallpox
• The portal of entry for smallpox is the respiratory tract or inoculation on the skin
• Excretions from the mouth and nose, rather than scabs, are the most important source of infectious virus
• Studies have shown that primary infection in the nose or mouth do not produce a “primary lesion” that ulcerates and releases virions onto the surface

Clinical Features• Rash stages of development
– All lesions in one region at same stage
– Starts macular, then papular
– Deep, tense vesicles by Day 2 of rash
– Turns to round, tense, deep pustules
– Pustules dry to scabs by Day 9
– Scabs separate

Clinical Features
• Scarring–From separated scabs
–Fibrosis, granulation in sebaceous glands
–Pink, depressed pock marks
–Prominent on face, usually >5 lesions
–Permanent

Clinical Features
• Complications– Sepsis/toxemia
• Usual cause of death• Associated with multiorgan failure• Usually occurs during 2nd week of illness
– Encephalitis• Occasional• Similar to demylination of measles,
Varicella


Clinical Features• Complications
– Secondary bacterial infections uncommon • Staphylococcus aureus cellulitis
– Responds to appropriate antibiotics
• Corneal ulcers– A leading cause of blindness before 20th Century
– Conjunctivitis rare• During 1st week of illness

A disfiguring Disease

Epidemiology
• Infectious Materials–Saliva
–Vesicular fluid–Scabs
–Urine
–Conjunctival fluid
–Possibly blood

Epidemiology
• Infectious Materials– Saliva
– Vesicular fluid
– Scabs
– Urine
– Conjunctival fluid
– Possibly blood

Diagnosis• Clinical diagnosis
– Sufficient in outbreak setting– >90% have classical syndrome
• Prodrome followed by rash
– Rarely, variants can be difficult to recognize• Hemorrhagic – mimics meningococcemia• Malignant – more rapidly fatal• Sine eruptione – prodrome without rash• Partially immune – milder, often atypical

Diagnosis• Traditional confirmatory methods
– Electron microscopy of vesicle fluid• Rapidly confirms if orthopoxvirus
– Culture on chick membrane or cell culture• Slow, specific for variola
• Newer rapid tests– Available only at reference labs (e.g. CDC)– PCR, RFLP

Laboratory Diagnosis of Smallpox
• Culture on Egg chorioallantoic membrane (CA): classical method; poxvirus grow on CA
• Direct examination of vesicle or pustular material: aggregations of virus may be seen in certain cytoplasm upon staining
• Tissue culture: growth in cultured cells• EM: negative staining is used to visualize characteristic large
brick shape of poxvirus– Relatively rapid – Can distinguish orthopox viruses from other viral agents – Cannot differentiate between variola and vaccinia viruses – May not be as sensitive as PCR-Based methods

Laboratory Diagnosis of Smallpox
• PCR Based method: In North America a positive test is considered diagnostic for vaccinia virus unless medical or epidemiologic evidence suggests otherwise
• With slight modifications to the fluorescently labeled probe, this assay can also be used to detect variola virus – Family specific primers are used first, then subgroup-specific
primers are used if the former is not successful in producing PCR product
• DNA Probes: Assays using immobilized oligonucleotides in a microarray have been developed to identify and discriminate among orthopoxviruses
• In situ hybridization of formalin-fixed tissues• Serology: Classical methods such as complement
fixation and gel precipitation commonly were used in the past; experimental enzyme-linked immunoassays are currently being evaluated

Diagnosis
• Differential Diagnosis– Chickenpox (varicella)
• Vesicles shallow, in crops, varied stages
• Centripetal, spares palms/soles
– Other orthopox viruses• Monkeypox – only in Africa, monkey contact• Vaccinia – after exposure to vaccine
• Cowpox – rare, only in UK

Prevention• Vaccination - History
– Introduced by Jenner• Inoculated boy with pustular fluid from cowpox
• 1st immunization using virus of similar disease
• Initially passed arm-to-arm– Also passed syphilis, hepatitis
• Eventually passed calf-to-calf on scarified leg• Immunity not lifelong

Prevention• Vaccine – modern times
– Vaccinia virus• Related to cowpox and variola
• Source – calf lymph
• Now cell culture methods available• Strains
– Lister used by WHO for eradication campaign– New York Board of Health only U.S. strain– Newer more attenuated Japanese strain

Jenner vaccinating

Vaccination for Small Pox

Vaccinating for Smallpox Prevention

Vaccinating for Smallpox



• Program Created by Dr.T.V.Rao MD for benefit of many in the world for
Historical perception on a Dead Disease
• Email• [email protected]