Embed Size (px)
Citation preview

Master in Medical Physics 2015 to 2016
Practical Report of Interventionism x-ray
Francisco J. Hernandez Flores
International Centre for Theoretical Physics
December 21, 2015
Abstract
This task it is about the quality control in Conventional X-Ray, The aim ofthe present Quality Control (QC) testing is to detect changes that may result ina clinically significant degradation in image quality or a significant increase inradiation exposures to both personnel and patients. of conventional x-ray suchas reproducibility of tube voltage, dose out put, time, and x-ray tube efficiency,Accuracy of kVp, mA, time. Examinations of these factors are studied usingadequate instrumentation for measure different parameter in the hospital Majoreof Trieste Italy. in which were discuses during this practice important concepts as:Automatic Exposure Control (AEC), KAP or DAP, the protection of the staff andpatient, the diagnostic reference levels (DRLs), the Interventional Reference Pointand the regular quality control in interventional radiology.
I. Introduction
Quality control (QC). has been acknowledged as a powerful and effective toolin optimizing radiation protection of the patients in diagnostic and interven-tional radiology (IR). Equipment performance testing is necessary to meet theaims of diagnostic radiology, i.e. to obtain images adequate for the clinicalpurpose with minimum radiation dose to patient.
QC in conventional diagnostic radiology has been well established. However,QC of modern digital radiology systems requires different approaches owingto differences in image receptor, image display devices, image format andequipment configuration. Available QC testing methods should be updated toencompass the developments in the field and to include digital imaging systems.The objective of this report was to evaluate the parameters performance ofPHILIPS fluoroscopy machine used in Angiography procedures by performmonthly quality control tests to check the radiation output consistency.
II. Theory
The x-ray system includes a collimator with motorized blades to adjust to theFOV, and Kerma Air Product (KAP) meter to monitor radiation output for each
1
Master in Medical Physics 2015 to 2016
patient is often available on interventional systems.
Interventional X-ray system re-quires: [3]
• Constant potential generator.
• C-arm system (under table x-raytube)
• High efficiency intensifier or flatpanel imaging system
• Digital image storage and re-trieval
Generally different dose levels influoroscopy are available: Low, Nor-mal and High
I. Quality Controls
The Quality Controls in interventionalradiology comprises (Recommenda-tions of Joint WHO-IRH-CE work-shoop):
• Dosimetrical Controls
• Image quality
• Detector characterisation
• Geometrical controls
• KAP calibration
• CBCT
• DICOM/PACS
II. Constancy tests (monthly)
The basic constancy test are:
• Reference dose, dose rates
• Resolution
• Field diameter
• Collimation
• Contrast resolution
• Tube and generator parameters
• Hard copy devices
III. Useful quantities for patient and staff risk evaluation:
• Dose area product (for stochastic effect). [3]
• Entrance surface dose (for deterministic effect. [3]
• Staff dose per procedure (in more than one location). [3]
The factors affecting the staff doses are: the main source of radiation for the staffin a fluoroscopy room is the patient due to the scattered radiation producedin the interaction of the beam with the patient. The scattered radiation is notuniform around the patient. The dose rate around the patient is a complexfunction of a number of factors. The scattered dose rate at 1 m from the patientcan be higher than 1 mGy/min for some C-arm positions.
2
Master in Medical Physics 2015 to 2016
IV. Diagnostic Reference Levels (DRLs)
"Diagnostic reference levels" means dose levels in medical radiodiagnostic orinterventional radiology practices, or, in the case of radio-pharmaceuticals,levels of activity, for typical examinations for groups of standard-sized patientsor standard phantoms for broadly defined types of equipment. [3]
DRLs are based on dose measurements in various types of hospitals, clinicsand practices. These values represent the 75th percentile KAP values recordedin a survey carried out in different Member of European Community States. [4]This parameter is useful to have a guidance on the level of dose, lower o higherthan the DRL, given to the patient for a specific treatments in a particular clinic.
V. Interventional Reference Point
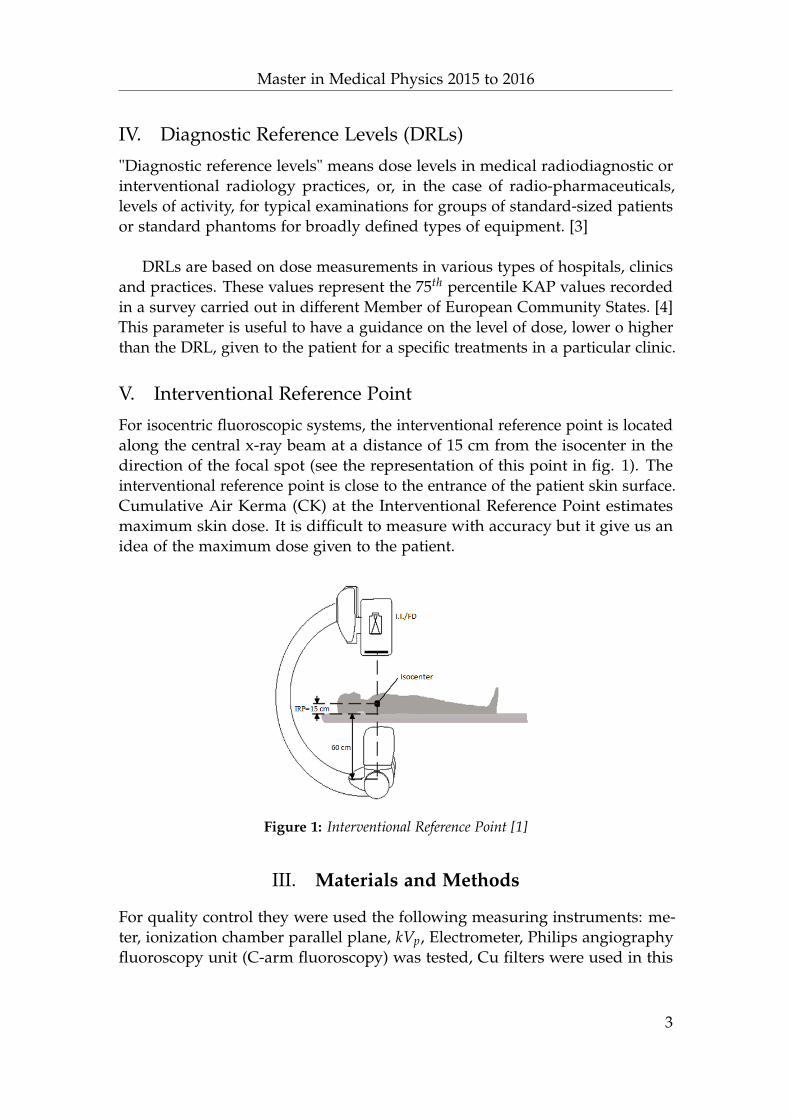
For isocentric fluoroscopic systems, the interventional reference point is locatedalong the central x-ray beam at a distance of 15 cm from the isocenter in thedirection of the focal spot (see the representation of this point in fig. 1). Theinterventional reference point is close to the entrance of the patient skin surface.Cumulative Air Kerma (CK) at the Interventional Reference Point estimatesmaximum skin dose. It is difficult to measure with accuracy but it give us anidea of the maximum dose given to the patient.
Figure 1: Interventional Reference Point [1]
III. Materials and Methods
For quality control they were used the following measuring instruments: me-ter, ionization chamber parallel plane, kVp, Electrometer, Philips angiographyfluoroscopy unit (C-arm fluoroscopy) was tested, Cu filters were used in this
3
Master in Medical Physics 2015 to 2016
experiment to check the exposure consistency.
This practice was made following the local protocol frequently used in qual-ity control in the Catinara Hospital, The chamber of ionization was positionedat 100 cm of distance at focal spot, connected at the electrometer for evaluatedthe Ka. then measurements began varying the kV with the same mAs at samedistance focal spot surface with different field sizes were measured (31, 25, 20and 17 cm) in different flouroscopy modes (low, normal and high) were usedto stimulate the automatic exposure control (AEC) to check the kVp and mAappeared in control panel of the system.
The value of kVp and mA were registered from the control panel and com-pared with the reference values of acceptation test for the machine.
The Quality Control (QC) in radiography is a central part of QA programme,which deals with equipment maintenance and monitoring. QA in diagnosticradiology is a mean of maintaining standards in imaging and working towardsminimizing patient and staff doses. To accomplish these objectives, a numberof physical parameters that affect the performance of X-ray imaging system areto be measured.
The equipment taking in to account for Radiation protection were leadaprons and thyroid shields also were visually checked.
IV. Results and discussion
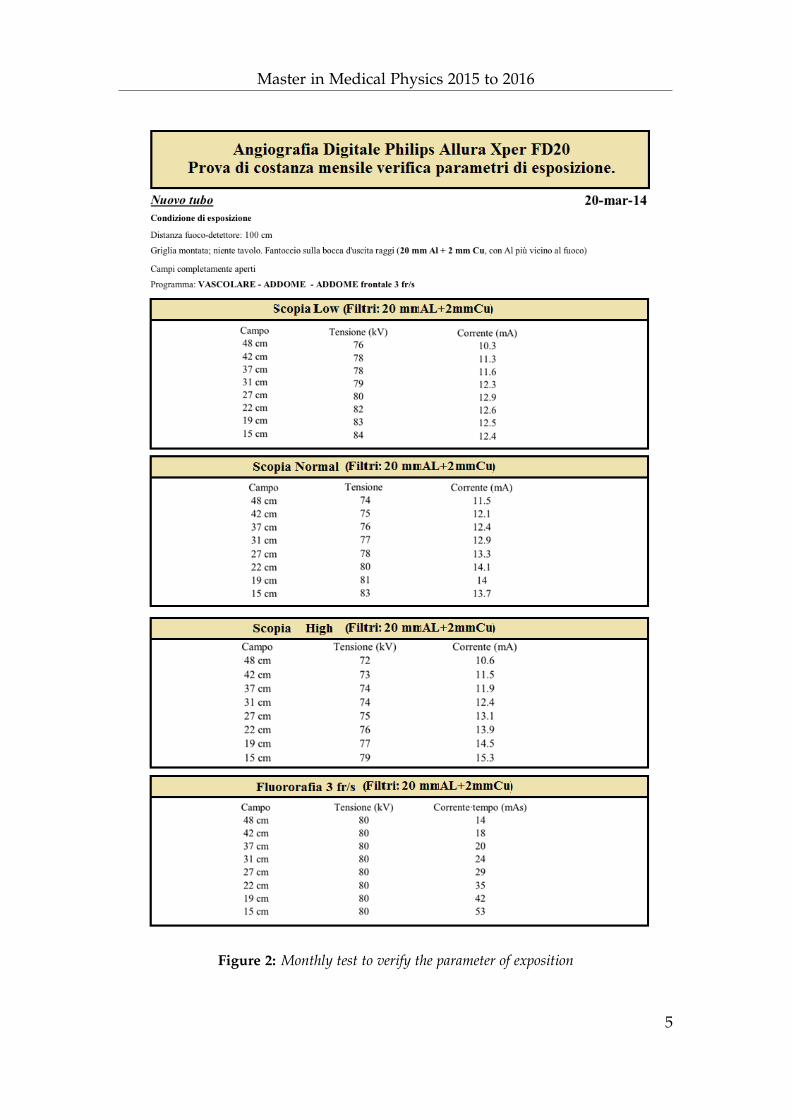
During the practice the monthly test regarding the constancy of the parameterof exposition was measured to compare with the reference base state. The dataobtained were similar to the data showed in the Fig. 2. This test is important tocontrol the well functionality of the Automatic Exposure Control (AEC).
The AEC controls the Incident Air Kerma to the image detector prevent fluc-tuation in image brightness and SNR that would make diagnosis or navigationof instruments difficult [2].
Fluoroscopic AEC may use the signal from a sensor to determine necessaryadjustments of fluoroscopic technique factors such as tube voltage and tubecurrent which depends of the Field of View (FOV) and the dose level (Low,Normal and High) like as showed in the fig. 2.
4
Master in Medical Physics 2015 to 2016
Figure 2: Monthly test to verify the parameter of exposition
5
Master in Medical Physics 2015 to 2016
V. Conclusion
• One of the most important part of quality control in interventional radiol-ogy is to measure the output of the Automatic Exposure Control in orderto avoid high unnecessary dose to the patient.
• Other important aspect in radiology obtained the best quality image usefulfor the radiologist using the ALARA concept in radiation protection for toreduce the dose of staff and damage in the skin of the patient due to thehigh dose.
• Due to the receive high dose or low dose produce effect they can tobe deterministic or probabilistic even the absorbed dose in this pointis very useful that the staff use the adequate protection like: aprons,lead eyeglasses, thyroid shield and radiation shields in order to reducesignificant this effects
• The reference point air kerma is the most approximate quantity to cal-culate the skin dose to the patient but it is not accurate and usuallyunderestimates or overestimates the real dose.
References
[1] Annalisa Trianni, Lecture 10 Skin dose calculation of Information Technologyin Medicine, ICTP Trieste Italy, 3rd trimester 2015.
[2] Dance, et.al. Diagnostic Radiology Physics. IAEA, Vienna, 2014.
[3] Paola Bregant , Lecture Physics of Diagnostic with x-ray 2, ICTP Trieste Italy,2015
[4] R.Padovani et al Reference Levels at European Level for Cardiac InterventionalProcedures, Vol:129;105-107, 2008.
6