Embed Size (px)
Citation preview

Patients and methods
Foam polidocanol sclerotherapy versus liquid
polidocanol sclerotherapy in management of varicose
veins in lower limbs
AbstractBackground: Varicose veins treatment with liquid sclerosing drugs has been performed for almost 100 years.
The first foam sclerosant were described 60 years ago (Goldman et al, 2002). On contact of the sclerosant with the
vein endothelium, the treated veins will be transformed into fibrous cords that cannot recanalize with a functional
result corresponds to the surgical removal of varicose veins (Malouf, 2000).
Patients and methods: One hundred patients complaining of varicose vein lower limbs less than 4mm in
diameter with competent sapheno-femoral and sapheno-popliteal junctions undergone sclerotherapy; 50 patients
were injected by liquid polidocanol And 50 patients were injected by foam polidocanol in the outpatient Clinic of
Suez Canal University Hospital at Ismailia-Egypt. We followed our patients for 6 months in which they were
evaluated for disappearance of varicose veins, side effects and satisfaction with chosen regimen.
Results: Most of the studied patients in both groups were females (56% in foamy POL group and 64% in liquid
POL group). Most of the studied patients were in age group ranging from 30 – 50 years (76% in foamy POL group
and 80% in liquid POL group). Both groups were matched as regarding age and sex. After 4 weeks of
sclerotherapy, total disappearance was more evident among patients treated with the foamy form of POL (84%
versus 52% in liquid POL group). Resolution and fading in pigmentation was significant in both groups, however
it was significantly better with the use of foam group. Post-sclerosis pain was significantly more with the use of
Liquid form of POL with median visual analogue scale 3 versus 1 with the use of Foamy form of POL. There was
no statistically significant difference between both groups regarding the incidence of different side effects.
Discussion and conclusion: Improvement occurred with the use of foamy form of POL was significantly better
than what was recorded with the use of liquid form of POL.
Key words: Foam POL, Liquid POL, Sclerotherapy.
Introduction
Varicose veins treatment with liquid sclerosing drugs has been performed
for almost 100 years. The first foam sclerosant was described 60 years
ago, and was demonstrated that it is hard to tell who has really invented
the technique. However, it remains obvious that two authors –Cabrera in
Spain and Monfreux in France- have boosted its use in the past 10 years
(Goldman et al., 2002).
Page

Patients and methods
The aim of sclerotherapy is the elimination of intracutaneous,
subcutaneous, and/or transfascial varicose veins (perforating veins). The
contact of the sclerosant with the endothelium leads to changes in the
venous wall. In the long term, successfully treated veins will be
transformed into fibrous cords that cannot recanalize. The functional
result corresponds to the surgical removal of varicose veins (Malouf,
2000).
The first advantage of foam is that it does not mix much with blood,
and, therefore, mechanisms of dilution do not happen. Foam sclerosant
also offer the advantage of being an excellent contrast medium for B-
mode echography since ultrasounds are scattered by the multiple
air/liquid interfaces and foam is recognized by its white cloud aspect and
dark shade cone (Guex, 2005).
Many different types of foams have been used and presented, using
different sclerosing agents. The approved technique is a double-syringe
system technique which has been manufactured and standardized but is
still undergoing complete evaluation. The method of this technique is to
mix gas and liquid through either a three-way stopcock or double-syringe
system technique (Guex, 2005).
The ideal sclerosing solution should be painless to inject, free of
adverse effects, and specific for damaged (varicose) veins. The two most
widely used sclerosing solutions worldwide are sodium tetradecyl sulfate
(STS) and polidocanol (POL). These sclerosing agents have a well-
Page

Patients and methods
documented history of safety and efficacy spanning 40 to 50 years (Breu
et al., 2004).
Patients and methods
The study is a clinical comparative study between foam polidocanol
sclerotherapy versus liquid polidocanol sclerotherapy in management of
varicose veins in lower limbs.
It included one hundred patients undergone sclerotherpy; 50 patients were
injected by liquid polidocanol And 50 patients were injected by foam
polidocanol in the outpatient Clinic of Suez Canal University Hospital in
Ismailia-Egypt. We followed our patients for 6 months, in the first 2
months at two weeks interval and after that every month.
In our study, we included:
1. Patient with Varicose veins who were proved by duplex ultrasound to have varicose veins with competent sapheno-femoral and sapheno-popliteal junction.
2. Varicose veins that less than 4 mm in diameter.3. Both sexes4. Age range from 18 to 60 years.
We assessed our patients before the procedure by: Full history taking,
thorough clinical examination, duplex Ultrasound and pelvi-abdominal
ultrasound.
Data collection
A total of 100 patients were enrolled in the study and were randomly allocated to one of two groups: Foamy POL group and liquid POL group. Sample size was taken as all patients with varicose veins in any age, both sexes, varicose vein diameter less than 4 mm without
Page

Patients and methods
incompetence in the sapheno-femoral and sapheno-popliteal junctions in a leg with healthy skin including the sites of injection without any contraindication for sclerotherapy. Fifty Patients were injected in the outpatient clinic by liquid polidocanol sclerotherapy 0.5% and 1% concentration and the other group (50 patients) was injected by foam polidocanol sclerotherapy 0.5% and 1% concentration. The optimal concentration was determined
according to the diameter of vein .
Data management
Gathered data were processed using SPSS version 15 (SPSS Inc.,
Chicago, IL, USA). Quantitative data were expressed as means ± SD
while qualitative data were expressed as numbers and percentages (%).
Chi Square and Fisher's exact tests were used to test significance of
difference for qualitative variables. A probability value (p-value) < 0.05
was considered statistically significant.
Method of injection and preparation of Sclerotherapy :
1. Selection of the concentration and formulation (liquid or Foam) of
Sclerosing agent was based on protocol outlined and presented in
Table (1). The vein diameter was measured by duplex ultrasound,
while the patient is standing. If foam was necessary, it is
formulated from 1 ml of sclerosing solution and 4ml of air mixed
at ratio of 1:4, using The Tessari method which uses a three-way
stopcock and two 5 ml syringe to mix sclerosant. Appropriate post
procedure care was being conducted, and patients will be asked to
keep a record of any adverse events resulting from treatment.
Sclerotherapy will be performed by standard technique on only one leg in
single treatment session. The dose of sclerotherapy is 2ml in each session.
All patients will require elastic stocking compress to the treated leg for 7
days following treatment, and ask the patient to walk directly after
Page

Patients and methods
injection. After having first leg treated, subjects returned 1week later for
treatment of contra lateral leg. Patient`s will be seen every 2 weeks
thereafter for follow-up.
Digital photographs were taken prior to treatment and at 4 weeks post-
treatment.
Table (1) Concentrations of polidocanol according to the diameter of
varicose vein and quantities used per injection
___________________________________________________________
Diameter Liquid Foam
___________________________________________________________
1-2mm 1% 0.5%
2.1-3mm 1.25% 0.65%
3.1-4mm 1.5% 0.75%
4.1-5mm 2% 1%
5.1-6mm 2.5% 1.25%
Volume per injection 0.5 ml 2 ml
Quantity (Polidocanol) per injection 0.5 ml 0.5 ml
___________________________________________________________
(Hamel-Desnos et al., 2003).
Ethical consideration
Written consents will be obtained from all patients before getting
them involved in this study.
The steps of the study; the aims , the potential benefits will be
discussed with each individual patient ,
Page

Patients and methods
Patient will be informed about any abnormal results of procedure
and tests performed and will be instructed and treated accordingly.
The patient has the right for withdrawal from the study at any time
with neither jeopardizing the right of the patient to be treated nor
affecting the relationship between the patient and the care provider.
Results
The aim of the present study was to assess the efficacy of polidocanol
(POL) in the foamy and liquid form in sclerotherapy of varicose veins of
the lower limb. A total of 100 patients with varicose veins were enrolled
in the study and were then randomly allocated to one of two treatment
groups; foam POL group (n= 50) and liquid POL group (n = 50). The
patients were evaluated for disappearance of varicose veins, side effects
and satisfaction with each of liquid and foamy form.
Table 1: - Patient characteristics among both groups of the study: -
Foamy POL(n=50)
Liquid POL(n=50)
Total(n=100)
p-value
Age (years)
20 – 8 (16%) 6 (12%) 14 (14%)
0.7 (NS)30 – 22 (44%) 18 (36%) 40 (40%)
40 – 16(32%) 20(40%) 36 (36%)
50 – 55 4 (8%) 6 (12%) 10 (10%)
SexMale 22 (44%) 18 (36%) 40 (40%)
0.8 (NS)Female 28 (56%) 32 (64%) 60 (60%)
NS: no statistically significant difference (p-value > 0.05).
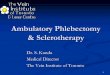
Table (1): Shows that both groups were matched as regarding age and
sex. Most of the studied patients in both groups were females (56% in the
foamy POL group and 64% in the liquid POL group). Most of the studied
Page

44%
36%
66% 64%
0%
10%
20%
30%
40%
50%
60%
70%
% o
f p
atie
nts
Male Female
Foamy POL Liquid POL
16%
12%
44%
36%
32%
40%
8%
12%
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
% o
f p
atie
nts
20 – 30 – 40 – 50 – 55
Foamy POL Liquid POL
Patients and methods
patients were in age group ranging from 30 – 50 years (76% in foamy
POL group and 80% in liquid POL group).
Graph 1: - Age distribution among both groups of the study: -
Graph 2: - Sex distribution among both groups of the study: -
Page

16%
48%
84%
52%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
% o
f p
atie
nts
Partial disappearance Total disappearance
Foamy POL Liquid POL
Patients and methods
Table 2: - Disappearance of varicose veins in both groups of the study: -
DisappearanceFoamy POL
(n=50)Liquid POL
(n=50)Total
(n=100)p-value
Partial disappearance 8 (16%) 24 (48%) 32 (32%)0.03*
Total disappearance 42 (84%) 26 (52%) 68 (68%)
*Statistically significant difference
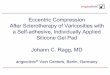
Table (2): Shows that there was statistically significant difference
between both groups as regarding degree of disappearance of varicose
veins after 4 weeks of sclerotherapy. Total disappearance was more
evident among patients treated with the foamy form of POL (84% versus
52% in liquid POL group).
Graph 3: - Disappearance in both groups of the study: -
Page

Patients and methods
Table 3: - Percentage of pigmentation pre and post-sclerosis in both groups of the study: -
% of pigmentationFoamy POL
(n=50)Liquid POL
(n=50)p-value
Pre-sclerosis 75% 78% 0.6 (NS)
Post-sclerosis 14% 47% 0.001*
p-value 0.001* 0.01*
*Statistically significant difference (p-value < 0.05)NS: no statistically significant difference
Table (3): illustrates the change in the percentage of pigmentation
after 4 weeks of sclerotic therapy in both groups. Improvement in the
percentage of pigmentation was significant in both groups, however the
improvement occurred with the use of foamy form of POL was
significantly better than what was recorded with the use of liquid form of
POL.
Page

Patients and methods
Table 4: - Degree of post-sclerosis pain and use of analgesia: -
Post-sclerosis painFoamy POL
(n=50)Liquid POL
(n=50)Total
(n=100)p-value
VAS
No pain 24 (48%) 12(24%) 36 (36%)
0.03*Mild 26 (52%) 28 (56%) 54(54%)
Moderate 0 (0%) 10 (20%) 10(10%)
median (range) 2(0 - 2) 6 (0 – 4) 4 (0 – 4)
Use of analgesia 4 (8%) 8(16%) 12 (12%) 0.7 (NS)
*Statistically significant difference (p-value < 0.05)NS: no statistically significant difference
Table (4): Shows that post-sclerosis pain was significantly more with
the use of Liquid form of POL with median visual analogue scale 3
versus 1 with the use of Foamy form of POL. Use of post-sclerosis
analgesia was higher in Liquid POL group but with no statistically
significant difference.
Page

Patients and methods
Table 5: - Side effects distribution among both groups of the study: -
Side effectsFoamy POL
(n=50)Liquid POL
(n=50)Total
(n=100)p-value
Ecchymosis 21 (42%) 19 (38%) 40 (40%) 0.8 (NS)
Hyper pigmentation 10 (20%) 6 (12%) 16 (16%) 0.7 (NS)
Itching 10 (20%) 8 (16%) 18 (18%) 0.9 (NS)
Telangiectatic matting 4 (8%) 2 (4%) 6 (6%) 0.9 (NS)
Marked swelling 6 (12%) 2(4%) 8 (8%) 0.6 (NS)
Superficial thrombophlebitis
0 (0%) 0 (0%) 0 (0%) 1 (NS)
DVT 0 (0%) 0 (0%) 0 (0%) 1 (NS)
Pulmonary embolism 0 (0%) 0 (0%) 0 (0%) 1 (NS)
Stroke 0 (0%) 0 (0%) 0 (0%) 1 (NS)
Skin necrosis 0 (0%) 0 (0%) 0 (0%) 1 (NS)
Allergic Reaction 0 (0%) 0 (0%) 0 (0%) 1 (NS)
NS: no statistically significant difference
Table (5): Shows the reported side effects among patients in both
groups of the study. Ecchymosis was estimated to be the most common
reported side effect in patients of both groups (42% in foamy POL group
and 38% in liquid POL group). These minor side effects were estimated
to be more common among patients treated with foam POL form but with
no statistically significant difference. Other reported side effects were
hyper pigmentation, Itching, telangiectatic matting and marked swelling.
There was no statistically significant difference between both groups
regarding the incidence of different side effects.
Page

Patients and methods
Graph 4: - Side effects distribution among both groups of the study: -
Page

92%
80%
8%
20%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
% o
f p
atie
nts
Satisfied Unsatisfied
Foamy POL Liquid POL
Patients and methods
Table 6: - Patients' satisfaction among both groups of the study: -
Foamy POL(n50)
Liquid POL(n=50)
Total(n=100)
p-value
Satisfied 46 (92%) 43 (86%) 89 (89%)
0.5 (NS)Unsatisfied 4 (8%) 7 (14%) 11 (11%)
Total 50 50 100(100%)
NS: no statistically significant difference
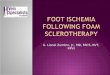
As regarding, the patient satisfaction with the form used in the
treatment, there was no significant difference between both groups. Only
11 patients were unsatisfied by the treatment; four patients in the foam
group and 7 in the liquid groups.
Graph 5: - Patients' satisfaction among both groups of the study: -
Page

Patients and methods
Discussion
The present study was aiming to assess the efficacy of polidocanol
(POL) in the foamy form and the liquid form in sclerotherapy of varicose
veins of the lower limb. A total of 50 patients with varicose veins were
enrolled in the study and were then randomly allocated to one of two
treatment groups; foam POL group (n= 25) and liquid POL group (n =
25). The patients were evaluated for clearance of varicose veins, side
effects and satisfaction with each of liquid and foamy form.
Polidocanol was reported by Goldman et al., (1987), Sadick (1994),
Weiss (1994) and Noel (2004) as an effective safe sclerosing solution
with distinct advantages of being forgiving with extravasation and having
extremely low risk of allergic reaction. The incidence of post sclerosis
pigmentation and telangiectatic matting in different sclerosing solutions
including polidocanol with different concentration was conducted in a
study done by Weiss and Weiss (1990). They stated that these
complications were related to both vessel size and to sclerosing
concentration.
Polidocanol at concentrations of 0.25%, 0.5% and 1% was injected in
the dorsal rabbit ear model by Goldman et al., (1987). They reported that
POL at concentration of 0.5% and 1% produced histologic and clinical
vein disappearance, whereas POL at 0.25% concentration didn't produce
clinical vein resolution. In addition, they noted recanalization at the low
concentration of 0.25%. In the present study we used both 0.5% and 1%
concentrations
Page

Patients and methods
Numerous studies were performed to compare the effect of different
sclerosing agents in the management of telangiectasia and reticular veins.
They used polidocanol in different concentration in their comparison. In
1987 Carlin and Ratz used polidocanol 0.25% in liquid form on 20
patients. The patients were injected every 4 weeks until all vessels had
disappeared or for a maximum of six visits. They reported that 13 patients
had good to excellent disappearance of veins and two had poor results.
They stated that the level of overall improvement was good. However,
they believed that the concentration of polidocanol that they used may
have been too low, resulting in slower disappearance of the vessels.
Another study used polidocanol 0.25% was presented by Kern et al.,
(2004). They used POL in both forms either as liquid or foam. A single
sclerosing session was performed in each patient. They proved that
polidocanol concentration of 0.25% had a lower efficacy in clearing the
telangiectatic and reticular veins in either forms.
Polidocanol at a concentration of 0.5% was used by Sadick (1994) to
treat reticular veins of 2 – 3 mm in diameter in 20 patients. A single
sclerosing session was performed in each patient. He stated that
polidocanol at this concentration was successful in the treatment of
reticular vessels. In 2005, another study was presented by Rao et al.,
using polidocanol in both forms, foamed and liquid. Their study was
carried on twenty patients. They emphasized that POL in both forms was
found to be effective in causing the disappearance of veins in all size
categories. Ecchymosis and reversible hyperpigmentation being the most
common adverse events occurred. Of note, no skin necrosis, no
recanalization was observed in any patient treated either form. All
Page

Patients and methods
subjects tolerated POL very well and were pleased with their treatments.
Their study confirms that POL, in both liquid and foamy forms have
similar efficacy, tolerability and patient satisfaction.
The results of this study show that for the same concentration of
polidocanol, the efficacy of sclerotherapy with foam is greater than with
liquid, although risks of minor adverse effects such as pain,
inflammation, and skin pigmentation are also more frequent. Other
authors have published similar results when using duplex-guided
sclerotherapy (Hamel-Desnos et al., 2003; Yamaki et al., 2004).
The specific characteristics of foam sclerosants may explain their
greater capacity and irritant nature. Foam sclerosants are compact
solutions that displace the blood column rather than dissolving in the
circulating blood. Foam adheres better to the walls of the vein, a feature
that, together with the capacity to provoke spasm, allows greater contact
with the endothelium, conferring greater efficacy at lower concentrations
and lower total quantity of sclerosant (Frullini et al., 2002).
The durability of the foam sclerosant combined with a greater capacity
to penetrate collaterals results in sclerosis over a larger region. The foam
is highly echogenic which facilitates ultrasound guided sclerotherapy,
increasing the safety of sclerosis of saphenous axes (Cavezzi and
Frullini, 1999; Frullini et al., 2000).
The greater efficacy seen in the foam group confirms the advantages
of this type of sclerosis and confirmation of efficacy by Duplex
ultrasound added value to the study. From the practical point of view,
Page

Patients and methods
foam sclerosis involves cheap, readily available, and easy to use products
in daily practice, not unduly lengthening the medical process and
probably reducing the number of sessions needed to treat each patient
(Alos et al., 2006).
Regarding the safety of the treatment, Harkins and Harmon in 1934
and Richardson in 1937 demonstrated the safety of injecting animals
with small doses of endovenous air for short periods. Based on these
experiments, Henriet (1997) analyzed the passage of this air to the
circulation system under several conditions of extracorporeal circulation
or during echocardiograms using air, confirming the safety of the
procedure. These results are consistent with several later clinical studies
using foam produced by various techniques (Garcia, 2001; Cavezzi et
al., 2002) proving that small doses of air injected intravenously do not
produce major systemic changes and are well tolerated by patients. The
presentation of major complications (deep vein thrombosis or lung
thromboembolism) is unusual with this technique and is probably related
to the dose used and the sclerosis region, occurring considerably more
often with truncal saphenous sclerosis, incompetent perforator veins, and
when large doses of foam are used (Varcoe, 2001). None of these
complications occurred in our study or in similar studies, mainly due to
the type of veins treated (reticular and postoperative) and the low doses
and concentrations used.
The minor complications recorded (local inflammation and
hyperpigmentation), which in our study were very similar to the study
published by Benigni and Sadoun (1999), present widely divergent
percentages in the literature, attributable to several possible factors: the
Page

Patients and methods
method of foam production, as non-industrial methods do not produce a
completely standardized microfoam; and the relatively low
concentrations and quantities used in each session (higher concentrations
of sclerosant produce smaller size bubbles). The larger bubble size could
be directly related to the appearance of inflammation beyond the
endothelium, involving the whole venous wall and the perivenous tissue
with the consequent clinical signs and anti-aesthetic secondary effects
such as skin pigmentation (Breu and Guggenbichler, 2004).
However, there is a clear tendency towards the reduction of foam
concentrations in order to achieve better results and avoid the secondary
effects characteristic of this technique. The use of postsclerosis, elastic
compression for only 48 h could have been another possible influential
factor as longer term compression has been shown to be effective in
reducing inflammation and its consequences (Vin and Benigni, 2003).
Skin pigmentation can also be reduced by performing drainage micro-
thrombectomy on the thrombosis of the treated vein (Scultetus et al.,
2003).
Other minor complications that have been described in the literature
(dizziness and blurred vision) derive from the passing of air from the
foam to the circulation system, are related to the total quantity of injected
foam, and are prevented by the patient gradually sitting up and previous
elevation of the treated limb (Frullini et al., 2002).
No incident of this kind was recorded in our study due probably to the
low doses administrated to all patients. There was a significant relation
between presentation of pigmentation and the concentration of sclerosant
Page

Patients and methods
used. but the sample size was small and statistical power limited, so care
must be used in the interpretation of this result.
An important feature of the design of this study and one which made
the two groups more homogeneous and easier to compare, was use of the
two techniques simultaneously on the same patient, each of whom acted
as his/her own control. Assessment of the differences between the
procedures was thus, more valid and precise with regard to both efficacy
and complications as any possible confounding factors that depended on
the patients were automatically corrected and variability was greatly
reduced. Likewise, the use of the duplex ultrasound allowed for greater
accuracy and objectivity in determining the percentages of sclerosant for
each venous caliber and enabled accurate measurement of partial and
complete efficacy.
In conclusion, the results of this study demonstrate that foam
polidocanol has greater sclerosant efficacy compared to liquid
polidocanol in the treatment of telangiectatic varices not involving the
saphenofemoral junction. A larger percentage of total sclerosis as well as
the extent of the obliterated region was observed. Despite this, foam
sclerosant also showed a greater tendency to provoke inflammation and
consequently mild adverse effects including pain, signs of inflammation
and skin pigmentation.
References
Page

Patients and methods
1. Ahmad I, Ahmad W, Dingui M. Prevention or reversal of deep
venous insufficiency by aggressive treatment of superficial
venous disease. Am J Surg. Jan;191(1):33-8. 2006
2. Angle N, Freischlag JA. Venous disease. In: Townsend CM Jr.,
Beauchamp RD, Evers BM, Mattox KL, editors. Sabiston
textbook of surgery. 17 ed. Philadelphia, PA: W.B. Saunders
Co.; th2004. Ch 67. Copyright © 2004 Elsevier is ease. Am J
Surg. Jan; 191(1):33-8. 2006
3. Amro mohamed, et al. Evaluation of new trends and materials
in Sclerotherapy of the lower limbs varicose veins. Summary;
Cairo University - Theses.2001
4. Alos J, Carreno P, Lopez JA, Estadella B, Serra-Prat M,
Marinel-lo J. Efficacy and Safety of Sclerotherapy Using
Polidocanol Foam: A Controlled Clinical Trial. Eur J
VascEndovascSurg.; 31: 101 – 107. 2006
5. Ballard JL, Bergan JJ, eds. Springer-Verlag, Chronic Venous
Insufficiency: Diagnosis and Treatment. London Berlin
Heidelberg. 2000.
6. Benigni JP, Sadoun S, Thirion V, Sica M, Demagny A,
Chaim M. Te´langiectasies et varices re´ticulaires. Traitement
par la mousse d’Aetoxiscle´rol a 0,25%. Pre´sentation d’une e
´tude pilote. Phle´bologie ;52:283–290.1999
Page

Patients and methods
7. Belcaro, G, Cesarone, MR, Di Renzo, A, et al. Foam-
sclerotherapy, surgery, sclerotherapy, and combined treatment
for varicose veins: a 10-year, prospective, randomized,
controlled, trial (VEDICO trial). Angiology ; 54:307.2003
8. Bergan JJ. Surgical procedures for varicose veins. In: Bergan
JJ, Yao JST, eds. venous disorders. Philadelphia: W.B.
Saunders Company ; 201–216.1991
9. Bergan JJ, Eklof B, Kistner RL, Moneta GL, Nicolaides AN,
and the International ad hoc committee of the American
Venous Forum. Classification and grading of chronic venous
disease in the lower limbs. A consensus statement, Vasc. Surg. .
30: 5–11. 1996
10.Bergan JJ. Ambulatory surgery of varicose veins. In: Goldman
MP, Bergan JJ, eds. Ambulatory treatment of venous disease..
St. Louis: Mosby. 149–154. 1996
11.Bergan JJ, Weiss RA, Goldman MP. Extensive tissue necrosis
following high-concentration sclerotherapy for varicose veins,
Derm Surg.. 26: 535–542. 2000
12.Bergan JJ, Rattner Z. Endovenous therapy—2005,
ActaChirBel.. 105(1): 12–15. 2005
13.Biegeleisen K, Neilsen RD, O’Shaughnessy A: Inadvertent
intraarterial injection complicating ordinary and ultrasound-
guided sclerotherapy. J DermatolSurgOncol 19:953-958, 1993
Page

Patients and methods
14.Blalock A. Oxygen content of blood in patients with varicose
veins, Arch Surg.. 19: 898–904. 1929
15.Blenkinsopp WK , Hamel-Desnos C, Desnos P, Wollmann
JC, Ouvry P, Mako S, Allaert FA. Comparison of tetradecyl
sulfate of sodium: Evaluation of the efficacy of polidocanol in
the form of foam compared with liquid form in sclerotherapy of
the greater saphenous vein: initial results, Dermatol. Surg.. (29):
1170 1175. 2003
16.Blalock A. Oxygen content of blood in patients with varicose
veins, Arch Surg. 1929. 19: 898–904. The cause of venous
ulceration, Lancet.. 1998-ii: 243–245. 1982
17.Bountouroglou DG, Azzam M, Kakkos SK, Pathmarajah M,
Young P, Geroulakos G. Ultrasound-guided foam sclerotherapy
combined with sapheno-femoral ligation compared to surgical
treatment of varicose veins: early results of a randomised
controlled trial. Eur J Vasc Endovasc Surg;31:93–100, 2006
18.Breu FX, Guggenbichler S. European consensus meeting on
foam sclerotherapy. DermatolSurg; 30(5):709–717. 2004
19.Bush RG, Hammond KA. Tumescent anesthetic technique for
long saphenous stripping, J Am Coll Surg.. 189: 626–628. 1999
20.Cabrera J, Cabrera Garcia-Olmedo JR. Nuevo metodo de
esclerosis en lasvaricaslares, PatolVasc.. 4: 55–73. 1995
Page

Patients and methods
21.Cabrera Garrido JR, Cabrera Garcia–Olmedo JR, Garcia–
Olmedo Dominguez MA:Elargissement des limites de la schle´
rothe´ rapie: noveauxproduitsscle´ rosantsPhle´ bologie 50:181-
188, 1997.
22.Cabrera J Jr., Garcia–Olmedo MA: Treatment of varicose
long saphenous veins with sclerosant in microfoam form: long
term outcomes. Phlebology 15:19-23, 2000.
23.Caggiati A, Bergan JJ, Gloviczki P, Jantet G, Wendell-Smith
CP, Partsch H. International Interdisciplinary Consensus
Committee on Venous Anatomical Terminology. Nomenclature
of the veins of the lower limbs: An international interdisciplinary
consensus statement, J Vasc Surg.. 36: 416–422. 2002
24.Cavezzi A, Frullini A. The role of sclerosing foam in ultrasound
guided sclerotherapy of the saphenous veins and of recurrent
varicose veins. Aust NZ J Phlebol;3:49–50,1999.
25.Cavezzi A, Frullini A, Ricci S, Tessari L. Treatment of
varicose veins by foam sclerotherapy: two clinical series.
Phlebology; 17:13–18. 2002
26.Cheatle T. The long saphenous vein: To strip or not to strip?
SeminVasc Surg.. 18(1): 10–14. 2005
27.Cohn MS, Seiger E, Goldman S. Ambulatory phlebectomy
using the tumescent technique for local anesthesia, Dermatol
Surg.. 21(4): 315–318. 1995
Page

Patients and methods
28.Coleridge Smith PD. Microcirculation disorders in venous leg
ulcer. Microcirculation in CVI, Microcirculation. 2001. pp. 1–
10. 2001
29.Cooper WM. Clinical evaluation of sotradecol, a sodium alkyl
sulfate solution, in the injection therapy of varicose veins,
SurgGynecol Obstet. MacGowen WAL et al. The local effects of
intra-arterial injections of sodium tetradecyl sulfate (STD) 3%:
An experimental study, Br J Surg.. 59: 101–104. 1972
30.Corbett CR, Runcie JJ, Lea TM, Jamieson CW. Reasons to
strip the long saphenous vein, Phlebologie.. 41: 766–769. 1988
31.Darke SG. Recurrent varicose veins. In: Goldman MP, Bergan
JJ, eds. Ambulatory treatment of venous disease. 1996. St.
Louis: Mosby. Bergan JJ. Saphenous vein stripping by inversion:
Current technique, Surgical Rounds.. 118–124. 2000
32.Dastain JY.Sclerotherapy of varices when the patient is on
anticoagulants, with reference to 2 patients on anticoagulants,
Phlebologie.. 34: 73. 1981
33.Davis LT, Duffy DM: Determination of incidence and risk
factors for postsclerotherapy Telangiectatic matting of the lower
extremity: a retrospective analysis. J DermatolSurgOncol 16:327
330, 1990.
Page

Patients and methods
34.Dawson TA, Black RJ, Strang WC, et al. Delayed and
immediate hypersensitivity to carbitols, Contact Dermatitis.. 21:
52. 1989
35.Eklöf B, Rutherford RB, Bergan JJ, Carpentier P, Gloviczki
P, Kistner RL et al., for the American Venous Forum
International Ad Hoc Committee for Revision of the CEAP
classification. Revision of the CEAP classification for chronic
venous disorders: Consensus statement, J. Vasc. Surg.. 40:
1248–1252. 2004
36.Escribano JM, Juan J, Bofill R, Maeso J, Rodriguez-Mori A,
Matas M. Durability of reflux-elimination by a minimal
invasive CHIVA procedure on patients with varicose veins. A 3-
year prospective case study, Eur J VascEndovasc Surg.. 25(2):
159–163. 2003
37.Fegan WG. Continuous compression technique of injecting
varicose veins, Lancet.. 2: 109. 1963
38.Fegan WG. Varicose veins: Compression sclerotherapy. 1967.
London: Heinemann. Hanschell HM. Treatment of varicose
veins, Br Med J.. 2: 630. 1947
39.Fronek HR. Noninvasive examination of thevenous system in
the leg: presclerotherapy evaluation.J DermatolSurgOncol ;15 :
170–173. 1989
Page

Patients and methods
40.Frullini A: New technique in producing sclerosing foam in a
disposable syringe. DermSurg 26:705-706, 2000.
41.Frullini A, Cavezzi A. Echoescle´rose par mousse de te
´tradecylsulfate de sodium et de polidecanol. Deuxanne
´esd’expe´rience. Phle´bologie 2000;53–4:431–435.
42.Frullini A. Sclerosing foam in the treatment of recurrent
varicose veins. In: Henriet J, ed. Foam sclerotherapy: state of the
art. Paris: Editions Phle´bologiquesFranc¸aises,:73–78. 2002
43.Frullini A, Cavezzi A. Sclerosing foam in the treatment of
varicose veins and telangiectases: history and analysis of safety
and complications. DermatolSurg;28(1):11–15. 2002
44.Garcia Mingo J.Tratamiento de la insuficienciavenosacro´nica
con esclerosantes en espuma: me´todo F.M.S (Foam Medical
System). Anales de Cirugı´aCardı´aca y Vascular;7(4):300–324.
2001
45.Georgiev M: Postsclerotherapy hyperpigmentation: a one-year
follow- up. J Dermatol Surg Oncol; 16:608-610. 1990
46.GeorgievM: Post sclerotherapy hyper pigmentations . J Dermato
lSurg Oncol; 19 : 649–652, 1993
47.Gerard J.Tortora. Principles of human anatomy, anatomy of
Blood vessels, ninth edition,. 254-269. 2002
Page

Patients and methods
48.Green D. Compression sclerotherapy techniques, Dermatol
Clin..7:137. 1989
49.Green D.Sclerotherapy for permanent eradicationof varicose
veins: theoretical and practical considerations. J Am Acad
Dermatol;38: 461–475. 1998
50.Goldman MP.Sclerosing agents in the treatment of
telangiectasia: Comparison of the clinical and histologic effects
of intravascular polidocanol, sodium tetradecyl sulfate, and
hypertonic saline in the dorsal rabbit ear vein model, Arch
Dermatol.. 123: 1196. 1987
51.Goldman MP. And Bennet R.: Treatment of telangiectasia: A
review. J Am Acad Dermatol; 17:167- 8. 1987
52.Goldman MP. A comparison of sclerosing agents: Clinical and
histologic effects of intravascular sodium morrhuate,
ethanolamine oleate, hypertonic saline (11.7%), and sclerodex in
the dorsal rabbit ear vein, J Dermatol Surg Oncol.. 17: 354. 1991
53.Goldman MP. Sclerotherapy: Treatment of varicose and
telangiectatic leg veins. Mosby, St. Louis, p 56, 1991.
54.Goldman MP, Weiss R, BergenJ: Diagnosis and treatment of
varicose veins: a review. J Am AcadDermatol;31 : 393–413,
1994
Page

Patients and methods
55.Goldman MP, Duffy DM, Sadick MD, Weiss RA:Guidelines
of care for sclerotherapy treatment of varicose and telangiectatic
leg veins. J Am AcadDermatol; 34 : 523–528, 1996
56.Goldman MP. Treatment of varicose and telangiectatic leg
veins: Double blind prospective comparative trial between
aethoxysklerol and sotradecol, Dermatol Surg.. 28: 52–55. 2002
57.Goldman MP. Sodium tetradecyl sulfate for sclerotherapy
treatment of veins: Is compounding pharmacy solution safe?
Dermatol Surg.. 30: 1454–1456. 2004
58.Guex JJ MD. Indications for the sclerosing agent Polidocanol®,
J DermatolSurgOncol.. 19: 959–961. 1993
59.Guex JJ MD, Isaacs, MN. Comparison of surgery and
ultrasound guided sclerotherapy for treatment of saphenous
varicose veins: Must the criteria for assessment be the same?
IntAngiol.. 19(4): 299– 302. 2000
60.Guex JJ MD, Allaert FA, Gillet JL, Chleir F. Immediate and
mid-term complications of sclerotherapy. Report of a
prospective Multi-center registry of 12,173 sclerotherapy
sessions, Dermatol Surg.. 31: 123. 2005
61.Guex JJ MD. Foam sclerotherapy: An overview of use for
primary venous insufficiency. Semin Vasc Surg.. 18: 25–29.
2005
Page

Patients and methods
62.Guex JJ MD: contraindication of sclerotherapy , update, J Mal
Vasc 30:144-149,2005
63.Hamel-Desnos C, Desnos P, Wollmann JC, Ouvry P, Mako
S, Allaert FA. Evaluation of the efficacy of polidocanol in the
form of foam compared with liquid form in sclerotherapy of the
greater saphenous vein: initial results. DermatolSurg; 29(12):
1170–1175. 2003
64.Harkins HN, Harmon PN. Embolism by air and oxygen:
comparative studies. ProcSocExpBiol Med;32:178. 1934
65.Hamel-Desnos C, Allaert FA, Benigni JP, Boitelle G, Chleir
F, Ouvry P, et al. Etude 3/1. Mousse de Polidocanol 3% versus
1% dans la grandeveinesaphène. Premiersrésultats, Phlébologie..
58(2): 165–173. 2005
66.Hayes, Inc. Hayes Report: Sclerotherapy for Symptomatic
Varicose Veins. December 2004. Search last updated January,.
Lansdale, PA. 2006
67.Henriet JP. Un ann de ptatiquequotidienne de la scle´rothe
´rapie (veinesreticulaires et te´langiectasies) par mousse de
polidocanol. Faisabilite´, Re´sultats, Complications. Phle
´bologie;50:355–360. 1997
68.Henriet JP: Expe´rienceduranttroisanne´es de la mousse de
polidocanoldans le traitement des varices re´ ticulaires et des
varicosite´ s. Phlebologie 52:277-282, 1999.
Page

Patients and methods
69.Holme JB, Holme K, Sorensen LS. The anatomic relationship
between the long saphenous vein and the saphenous nerve.
Relevance for radical varicose vein surgery, Acta Chir Scand..
154(11–12): 631–633. 1988
70.Hoshino S, Satokawa H, Ono T, Igari T. Surgical treatment for
varicose veins of the legs using intraoperative angioscopy. In:
Raymond Martimbeau P, Prescott R, Zummo M, eds.
Phlebologie 92. Paris: John LibbeyEurotext.. pp. 1083–1085.
1992
71.Hollinshead WH. The back and limbs. In: Hollinshead WH, ed.
Anatomy for surgeons. New York: Harper & Row Publishers..
617–631, 754–758, 803–807. 1969
72.Homans J. The operative treatment of varicose veins and ulcers
based on a classification of these lesions, SurgGynecObst.. 22:
143– 158. 1916
73.Imhoff E, Stemmer R. Classification and mechanism of action
of sclerosing agents, Soc Fran Phlebol.. 22: 143. 1969
74.Jones L, Braithwaite BD, Selwyn D, Cooke S, Earnshaw
JJ.Neovascularisation is the principal cause of varicose vein
recurrence: Results of a randomized trial of stripping the long
saphenous vein, Eur J VascEndovasc Surg.. 12(4): 442–445.
1996.
Page

Patients and methods
75.Kanter AH. Complications of sotradecolsclerotherapy with and
without heparin. In: Raymond-Martimbeau P, Prescott R,
Zummo M, eds. Phlebologie ’92, Paris,. John Libbey Eurotext.
1992
76.Kanter A: Clinical determinants of ultrasound-guided
sclerotherapy outcome. Part I: The effects of age, gender, and
vein size. DermatolSurg 24:131-135, 1998.
77.Kern P et al. Single-blind randomized studycomparing
chromated glycerin, polidocanol solution and polidocanol foam
for treatment of telangiectatic leg veins. DermatolSurg; 30 :
367–372, 2004
78.Kostas T, Ioannou CV, Touloupakis E, Daskalaki E,
Giannoukas AD, Tsetis D, Katsamouris AN. Recurrent
varicose veins after surgery: A new appraisal of a common and
complex problem in vascular surgery, Eur J VascEndovasc
Surg.. 27(3): 275–282. 2004
79.Labas, P, Ohradka, B, Cambal, M. Long term results of
compression sclerotherapy. Bratisl Lek Listy; 104:78. 2003
80.Labropoulos N, Volteas N, Leon M, et al: The role of venous
outflow obstruction in patients with chronic venous dysfunction.
Arch Surg 1329:46-51, 1997.
Page

Patients and methods
81.Labropoulos N, Kang SS, Mansour MA, et al: Primary
superficial vein reflux with competent saphenous trunk. Eur J
EndovascSurg 18:201-206, 1999.
82.Lane RJ, Graiche JA, Coroneos JC, Cuzzilla ML. Long-term
comparison of external valvular stenting and stripping of
varicose veins, ANZ J Surg.. 73(8): 605–609. 2003
83.Lerond L, Bergan JJ, Schmid-Schönbein GW. Venous
hypertension, inflammation and valve remodeling, Eur J
VascEndovasc Surg.. 28: 484–493. 2004
84.MacKenzie RK, Paisley A, Lee AJ, Ruckley CV, Bradbury
AW. The effect of long saphenous vein stripping on quality of
life, JVS.. 35(2): 1197–1203. 2002
85.MacKenzie RK, Allan PL, Ruckley CV, Bradbury AW. The
effect of long saphenous vein stripping on deep venous reflux,
Eur J VascEndovasc Surg.. 28(1): 104–107. 2004
86.Martin DE, Goldman MP. A comparison of sclerosing agents:
Clinical and histologic effects of intravascular sodium tetradecyl
sulfate and chromatedglycerine in the dorsal rabbit ear vein, J
DermatolSurgOncol.. 16: 18. 1990.
87.Mendoza E. To the topographic anatomy of the Vena saphena
magna: A duplex sonographische study regarding by surgery
relevant aspects, Phlebologie.. 30: 140–144, 2001.
Page

Patients and methods
88.Mendes RR, Marston WA, Farber MA, Keagy BA. Treatment
of superficial and perforator venous incompetence without deep
venous insufficiency: Is routine perforator ligation necessary? J
Vasc Surg.. 38(5): 891–895. 2004
89.McMullin GM, Coleridge Smith PD, Scurr JH. Objective
assessment of ligation without stripping the long saphenous vein,
Br J Surg..78: 1139–1142. 1991
90.Min RJ, Navarro L:Transcatheter duplex ultrasound-guided
sclerotherapy for treatment of greater saphenous vein reflux:
preliminary report. DermatolSurg 26:410-414, 2000.
91.Monfreux A: Traitement sclerosant des troncssaphe` nies et
leurscollate´ rales de groscalibre par le me´ thode mus. Phle´
bologie 50:351- 353, 1997.
92.Neglen P. Treatment of varicosities of saphenous origin:
Comparison of ligation, selective excision, and sclerotherapy. In:
Bergan JJ, Goldman MP, eds. varicose veins and telangiectasias:
Diagnosis and treatment.. St. Louis: Quality Medical Publishing:
148–165. 1993
93.Negus D. The blood vessels of lower limb: Applied anatomy. In:
NegusD, ed. Leg ulcers: A practical approach to management.
2e. London: Butterworth-Heinemann 1992.
Page

Patients and methods
94.Nyamekye I, Shephard NA, Davies B, Heather BP, Earnshaw
JJ. Clinicopathological evidence that neovascularization is a
cause of recurrent varicose veins, Eur J VascEndovasc Surg.. 15:
412–415. 1998
95.Orbach EJ:Sclerotherapy of varicose veins: utilization of an
intravenous air-block. Am J Surg 66:362-366; 1944.
96.Panetta TF, Marin ML, Veith FJ, Goldsmith J, and Gordon
RE, Jones AM et al. Unsuspected preexisting saphenous vein
disease: An unrecognized cause of vein bypasses failure, J Vasc
Surg.. 15(1): 102– 110. 1992
97.Pappas PJ, DeFouw DO, Venezio LM, Gorti R, Padberg FT,
Jr., Silva MB, Jr., et al. Morphometric assessment of the
dermal microcirculation in patients with chronic venous
insufficiency, J Vasc Surg.. 26: 784–795. 1997
98.Pascarella L, Lerond L, Bergan JJ, Schmid-Schönbein GW.
Venous hypertension, inflammation and valve remodeling, Eur J
Vasc and Endovasc Surg.. 28: 484–493. 2004
99.Pereira F, Pereira C, Lacerda MH. Contact dermatitis due to a
cream containing chitin and a carbitol. Contact Dermatitis.. 38:
290–291. 1998
Page

Patients and methods
100. Perrin M, Guidicelli H, Rastel D. Surgical techniques used
for the treatment of varicose veins: Survey of practice in France,
J Mal Vasc.. 28(5): 277–286. 2003
101. Piulachs P, Vidal Baraquer F. Pathogenic study of
varicose veins, Angiology.. 4: 59–100. 1953
102. Porter JM, Moneta GL, an International Consensus
Committee on Chronic Venous Disease. Reporting standards in
venous disease: An update, J. Vasc. Surg.. 21: 635–645. 1995
103. Rabe E, Pannier Fischer F, Gerlach H: Guidelines
for sclerotherapy of varicose veins. Dermatol Surg ; 30: 686–
693. 2004
104. Ramelet AA, Monti M: Phlebology: The Guide. Elsevier,
Amsterdam, 1999
105. Redrawn from Mózes G, Gloviczki P, Kádár A,
Carmichael SW. Chapter 2, Anatomy of the Perforating Veins
in Gloviczki, P, and Bergan, JJ, eds. Atlas of Endoscopic
Perforating Vein Surgery. Springer, London. 1998.
106. Richardson HF, Coles BC, Hall GE. Experimental gas
embolism: intravenous air embolism. Toronto Can Med Assoc
J;36:584–588. 1937
107. Rutherford RB, Padberg FT, Comerota AJ, Kistner RL,
Meissner MH, Moneta GL. Venous severity scoring: An adjunct
to venous outcome assessment, J. Vasc. Surg.. 31: 1307–1312.
2000.
Page

Patients and methods
108. Sadick NS. Treatment of varicose and telangiectatic leg
veins with hypertonic saline: A comparative study of heparin
and saline, J DermatolSurgOncol. Bodian EL. Sclerotherapy,
SeminDermatol.. 6: 238. 1987
109. Sadick NS. Treatment of varicose and telangiectaticleg
veins with hypertonic saline: a comparative study of heparin and
saline. J DermatolSurgOncol; 16 : 24–28, 1990
110. Sadick NS, Farber B. A microbiologic study of diluted
sclerotherapy solutions, J DermatolSurgOncol.; 19: 450. 1993
111. Sadick NS. Hyperosmolar versus detergentsclerosing agents
in sclerotherapy. J DermatolSurgOncol; 20 : 313–316. 1994
112. Sadick NS, Wasser S. Combined endovascular laser plus
ambulatory phlebectomy for the treatment of superficial venous
incompetence: a 4-year perspective. J Cosmet Laser Ther.
Mar;9(1):9-13. 2007
113. Sarin S, Scurr JH, Coleridge Smith PD. Stripping of the
long saphenous vein in the treatment of primary varicose veins,
Br J Surg.. 81(10): 1455–1458., 1994
114. Schmid-Schönbein GW, Bergan JJ. Leukocyte activation
in patients with venous insufficiency, J Vasc Surg.. 30: 148–156.
1999
Page

Patients and methods
115. Schmid-Schönbein GW, Takase S, Bergan JJ. New
advances in the understanding of the pathophysiology of chronic
venous insufficiency, Angiology.. 52: Suppl 1: S27–34. 2001
116. Schmier AA. Clinical comparison of sclerosing solutions in
injection treatment of varicose veins, Am J Surg.. 36: 389. 1937
117. Scott HJ, Smith PDC, Scurr JH. Histological study of
white blood cells and their association with lipodermatosclerosis
and venous ulceration, Br J Surg. 78: 210–211. 1991
118. Scultetus AH, Villavicencio JL, Kao TC, Gillespie DL,
Ketron GD, Iafrati MD.Microthrombectomy reduces
postsclerotherapy pigmentation: multicenter randomized trial. J
Vasc Surg;38:896–903, 2003
119. Somjen GM. Anatomy of the superficial venous system,
Dermatol Surg.. 21: 35–45. 1995
120. Stuart WP, Adam DJ, Allan PL, Ruckley CV, Bradbury
AW. Saphenous surgery does not correct perforator
incompetence in the presence of deep venous reflux, J Vasc
Surg.. 28(5): 834–838. 1998
121. Tarek Hamada, Mohmed Abd El Hamid. Foam treatment
for varicose veins; efficacy and safety, Sci. Med. J. ESCME,
Vol. 18, No. 1, January 2006
Page

Patients and methods
122. Takase S, Lerond L, Bergan JJ, Schmid-Schönbein GW.
The inflammatory reaction during venous hypertension in the
rat, Microcirculation.. 7: 41–52, 2000
123. Tessari L, Cavezzi A, Frullini A: Preliminary experience
with new sclerosing foam in the treatment of varicose veins.
DermatolSurg 27:58-60, 2001.
124. Tezelaar DJ, Neumann HAM, De Roos KP. Long cotton
wool rolls as compression enhancers in macrosclerotherapy for
varicose veins. DermatolSurg; 25: 38–40, 1999
125. Thibault PK, Wlodarczyk: Correlation of serum ferritin
levels and postsclerotherapy pigmentation- a prospective study. J
DermatolSurgOncol 20:684-686, 1994
126. Thomas PR, Nash GB,Dormandy JA. White cell
accumulation in dependent legs of patients with venous
hypertension: A possible mechanism for trophic changes in the
skin, Br Med J (Clin Res Ed).. 18; 296(6638): 1693–520, 1988
127. van Rij AM, Jones GT, Hill GB, Jiang P.
Neovascularization and recurrent varicose veins: More histologic
and ultrasound evidence, J Vasc Surg.. 40(2): 296–302. 2004
128. Varcoe P. Complications of duplex guided sclerotherapy.
IntAngiol ;20(Suppl 1):25. 2001
129. VIN F, Allert FA, Levardon M: Influence of estrogens and
progesterone on the venous system of the lower limbs in women.
J DermatolSurgOncol 18:888-892, 1992.
Page

Patients and methods
130. Vin F, Benigni JP.Confe´rence international de consensus
sur la compression. Compresionapre`sd’escle´rothe´rapie. Phle
´bologie;56:349–351. 2003
131. Weiss RA, Sadick NS, Goldman MP, Weiss MA. Post
sclerotherapy compression: controlled comparative study of
duration of compression and its effect of clinical outcome.
DermatolSurg: 105–108. 2005
132. Weiss RA, Weiss MA. Controlled radiofrequency
endovenous occlusion using a unique radiofrequency catheter
under duplex guidance to eliminate saphenous varicose vein
reflux: A 2-year follow-up, Dermatol Surg.. 28: 38–42. 2002.
133. Winterborn RJ, Foy C, Earnshaw JJ. Causes of varicose
vein recurrence:Late results of a randomized controlled trial of
stripping the long saphenous vein, J Vasc Surg.. 40(4): 634–639.
2004
134. Wollmann JC. Schaum—zwischenVergangenheit und
Zukunft. 8. Bonner Venentage 15–16. Feb. Vasomed.. 16(1):
34–35. 2002
135. Wollmann JC. The history of sclerosing foams, Dermatol
Surg.. 30: 694–703. 2004
Page

Patients and methods
136. Yamaki T, Nozaki M, Iwasaka S. Comparative study of
duplexguided foam sclerotherapy and duplex-guided liquid
sclerotherapy for the treatment of superficial venous
insufficiency. DermatolSurg; 30(5):718–722. 2004
137. Zamboni P, Cisno C, Marchetti F, Quaglio D, Mazza P,
Liboni A. Reflux elimination without any ablation or
disconnection of the saphenous vein. A haemodynamic model
for venous surgery, Eur J VascEndovasc Surg.. 21(4): 361–369.
2001
138. Zimmet S: The prevention of cutaneous necrosis following
extravasation of hypertonic saline and sodium tetradecyl sulfate.
J. Dermatol Surg Oncol 19:641-646, 1993.
139. Zimmet S: Hyaluronidase in the prevention of sclerotherapy
induced extravasation necrosis: a dose-response study. Derm;
Surg22:73- 77, 1996.
Page