Embed Size (px)
Citation preview

Kursk State Medical UniversityDepartment of Internal Disease N 1
Sarcoidosis
Student: Gustavo Duarte VianaGroup: 17Course: 6th year 2nd semester

Sarcoidosis (or Bersier Boeck- Schaumann disease)
• Chronic multisystemic inflammatory disorder of unknown etiology that lead to non ceseous granuloma formation, it most commonly affects the lungs, but can also affect other organs mainly the eyes, skin and bones.
• The name sarcoidosis is derived from a misunderstanding, because doctor in the ninth century thought that it was a benign form of extreme aggressive neoplasm.

History of sarcoidosis• In 1899, the pioneering Norwegian
dermatologist Caesar Boeck describe skin nodules characterized by compact, sharply defined foci of "epithelioid cells with large pale nuclei and also a few giant cells .
• Thinking this resembled sarcoma, he called the condition "multiple benign sarcoid of the skin.

EpidemiologyIt is a worldwide disease, but there are some prevalence in Scandinavian countries. But it may affect all ethnic groups. •It has a biphasic peak: Mostly in the ages around 20-40, but it also appears around the 60.•M-F ratio 2:1.•Affects siblings of first- or second- degree relatives in 15% of patients with sarcoidosis.•It is known that US black people have more severe cases of pulmonary and skin sarcoidosis, but Japonese have more cases of eyes sarcoidosis.

Etiology and Pathogenesis• Cause is unknown, although both genetic and environmental factors
suspected.• Theory that disease develops in genetically predetermined hosts who are
exposed to certain environmental agents that trigger an exaggerated inflammatory immune response leading to granuloma formation, specially because the organs most affects (lungs, skin and eyes) are in direct exposure to the triggers.
• The trigger may be some insecticides, fungi, firefighting chemical, wood-burning stoves, tree pollen, heavy metals, some dusts or even bacteria such as Propionibacterium acnes (its DNA was detected by PCR in the granulomas).
• Dust, miners or civil workers are more affected, there was a break out of sarcoidosis in the workers helping in the 11-09-2001 (world trade center)

• Hallmark is non caseaous granulomasn formation, composed of a compact core of macrophages and around it a layer oflymphocytes T CD+4 and lesser quantity lymphocytes B, sometimes the macrophages can even fuse together forming a multinucleated giant cell. There are a surrounding group of macrophages forming the epithelioid histocytes.
• It is made in the porpose to surround and protect the organism of a still unknown trigger.
• If the inflammatory process is persistent, it realease chemiotaxis to fibroblasts which circumscribe the granuloma and lead to formation of fibrotic tissue (scar) of granuloma and surrounding tissue. It may lead to abnormalities in normal architecture of the organ and further dysfunction.

T cells, Macrophages
Chemoattractants Growth Factors
Cellular proliferation Granuloma
Fibrosis
Pathogenesis


Curiosities
In severe cases of AIDS, there is a very low account of T lymphocytes T CD4+, It lead to sarcoidosis “spontaneous remission”, but when patient starts properly the antiretroviral therapy, sarcoidosis return as the level of CD4+ raise up to normal level, it is one of the phenomenon of the IMMUNE RECONSTITUTION SYNDROME.
Kveim Siltzbach test: if positive, it is considered of diagnostic value, for rarely done due to difficulties in the method and standardization of the method itself. It consists of injection a known homogenized sarcoidosis tissue to the subcutaneous tissue of the patient, if after 4-6 weeks appear a papule, it is considered positive. Mechanism is due to the Kveim Siltzbach reaction. It differs from a hypersensitivity reaction because it only occurs after 4-6 weeks.
It is possible to find markers of other disease, which my difficult at first the diagnosis, markers such as Rheumatoid factor, antinuclear antibodies, anti T lymphocyte antibodies.
As long as the disease persists untreated, more likely is to develop secondary organ disfunction.

Clinical Presentation• One third have non-specific symptoms of fever, fatigue, weight
loss and malaise.• It may be very difficult to diagnose sarcoidosis due to lack of
specific symptoms, in average it takes 1 year to diagnosis if disease affects mostly the lungs and 6 months if affects mostly the skin.
Forms: asymptomatic Acute Chronic

Asymptomatic: 30-50% of patients and are diagnosed on routine CXR, usually with the classical SYMMETRICAL BILATERAL HILAR ADENOPATHY with or without infiltrate.
Acute: with evolution within few weeks with generalized symptoms as fever, severe asthenia and anorexia and symptoms of pulmonary affection as dyspnea, cough and chest discomfort.
there are two acute syndromes distinguished separately in acute sarcoidosis
Loefgren syndrome, it is mostly frequent in Scandinavian women, from inland and Puerto Rico.
1- Uveitis
2- Erythema Nodosum
3- X-ray finding of symmetrical bilateral hilar adenopathy or parabrachial.
4- acute peripheral arthritis or poliarthralgia.
Heerfordt Walderstrom syndrome or AKA eveoparotid fever
1- Fever
2- parotid enlargement
3- anterior uveitis
4- facial paralysis. Chronic: insidious form lasting for months, strongly linked with respiratory symptoms and in lesser stand with
generalized symptoms, it lead to permanent irreversible organ changes, in specially lungs.



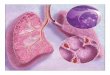
Specific organ involvement✕ Lungs: more than 90% of patients with sarcoidosis will evolve to abnormalities shown in the X-ray, in very early stages
where interstitial pneumonia is present before formation of the granulomas. The infiltrate is usually in the upper lobes (in contrary to other non infectious pneumopathy).
One third of the patients shows restrictive pneumopathy in pulmonary function test and one third of the patients show criteria of obstructive pneumopathy.
There is the classical symmetrical bilateral hilar adenopathy which is very suggestive, but not pathognomonic because it may be also present in fungic infections and neoplasia like bronchogenic carcinoma.
The main symptoms are dyspnea, dry cough and retrosternal dysconfort, others symptoms are seldom seen as pleural involvement, pleural infusion, hemoptesis.
✕ Upper air ways: 20% of patients has involvement of the nasal mucosa leading to nasal obstruction, but all naso-oral mucosa may be involved leading to high dyspnea, wheezing and hoarseness (Laryngeal sarcoidosis).
✕ Lymph-nodes: intrathoracic are enlarged in more than 90% of the patients with the classic symmetrical bilateral hilar adenopathy, other lymph- nodes may be also involved as cervical chain, axillary and inguinal and they are painless, mobile and non ulcerative and usually not perceived by the patient.

✕ Skin: about one third of patients which
• Erythema nodosum: they are erythematous painful nodules in the anterior surface of the legs, they represent a subcutaneous vasculitis.
• Maculopapulous eruptions: they are due to granulomas itself and may be up to 3cm with a plateau surface and of wax appearance, they may be found all over the body.
• Dischromias: usually painless and of a violate tin. • Subcutanous nodules: in trunk and extrimities• Lupus pernio: it forms complex of shining cyanotic harden lessions around the nose, libs, checks and
ears, it may erode to bones and cartilages around.
• It may develop over surgical scars and tattoo.



✕ Eyes: 25% of patients
Anterior uveitis: photophobia, epiphora and blurred vision.
Sicca keroconjutivitis
Blindness
✕ Bone marrow: 40% of patients, but lead only to a mild lymphopenia, very rare hematological alterations.
✕ Spleen: 10%, but rarely lead to hiper-splenism syndrome.
✕ Liver: 50% reveals granulomas during autopsy, but rarely lead to hepatogram abnormalities, usually only alkaline phosphatase is increased.
✕ Pancreas and intestine are rare affects, only granulomas at autopsy.
✕ Kidney: rare formation of granuloma, but sarcoidosis indirectly may lead to renal morbidity due to increasing of active D vitamin (Granuloma has 25-hydroxivitamin D), which leads to hyperkalemia and therefor nephrocalcinosis and repeated nephrolithiasis. All patients with sarcoidosis must routinely check urine level of calcium and in blood analysis.
✕ Central and peripheral nervous system or neurosarcoidosis: A) cranial nerve paralysis B) migraines C) ataxia D) cognitive dysfunction E) Asthenia F) seizures G) mononeuropathy or even polyneuropathies of peripheral nerves leading to sensorial loss or paresthesy H) Incidious lymphocytic meningitis (sarcoidosis meningitis) I) Diabetes insipidus due to granulomatous lesion to hypothalamus.
✕ Endocrine glands: 10% involving the parotid gland (Heerfordt syndrome) and rarely suprarenal cortex insufficiency.




✕ Heart: 25% reveal granulomas in cardiac tissue, but only 5% will have symptoms, except Japoneses where one forth of them will have heart sarcoidosis affection.
it may lead to: cardiac blocks, arrhythmias, angina, aneurisms, pericardial effusion, chronic cardiac insufficiency. Cor pumonale is rare, but has association to pulmonary fibrosis in advanced sarcoidosis.
✕ Bones: affects mostly the phalanges, metacarpus and metatarsus leading to deformities in fingers and nails. May lead to osteoporosis and cist formation
✕ Joints: arthritis or polyarthritis of big joints as ankles, knees, wrists and elbow. Patients with gout may have worsening of the clinical picture because the granuloma itself produces purines.
✕ Muscles: acute myositis and chronic myopathy.
✕ Breats✕ Tests ✕ Ovaries ✕ Stomach✕ Others




Common Clinical Features

Erythema Nodosum

Lupus Pernio


X-ray manifestations✕Nodules on X-ray may be isolated or multiples which may suggest
tumor, or they may be even miliar suggesting TB.✕Hilar or mediastinal lymph-nodes may have the EGG SHELL
appearance of calcifications suggesting as differential diagnosis silicosis.
✕May have bullae formation or true cavities with mycetoma inside.✕Lobar atelectasia by endobronchic granulomas✕Pleural infusion

4 Stages of Pulmonary Sarcoidosis
I Bilateral hilar lymphadenopathy and paratracheal adenopathy
55-90% remissio
nII Mediastinal adenopathy with
pulmonary parenchymal involvements
40-70%
III Pulmonary parenchymal without adenopathy
10-20%
IV Pulmonary fibrosis with honeycombing
0-5%

Stages

Laboratory StudiesRoutine lab evaluation often is unrevealing.Blood and biochemical blood analysis
Increased erythrocyte sedimentation rate (except in Loefgren syndrome)LymphopeniaHyperglobulinemiaHypercalcemia or hypercalciuria. Hypercalcemia is seen in about 10-13% of patients, whereas hypercalciuria is 3 times more common.Elevated alkaline phosphatase level suggests hepatic involvement. Angiotensin converting enzyme may be elevated.
Lumbar PunctureLiqueur may have pleocytosis due to lymphocytes, elevated protein and normal glucose (aseptic lymphocytic meningitis)

Biopsy specimen • A biopsy specimen should be obtained from the
involved organ that is most easily accessed, such as the skin, peripheral LN. (not in erythema nodosum)
• Eyes, lacrimal glands and gums only if they are affected.
• If diagnosis requires pulmonary tissue, trans-bronchial biopsy by means of bronchoscopy has a diagnostic yield of at least 85% when multiple lung segments are sampled. It may also be obtained by mediastinoscopy or thoracothomy.

The central histologic finding is the presence of NCGs with special stains negative for fungus and
mycobacteria.

Diagnosis
Consists of 3 main points •Clinical manifestations •Chest X-ray showing typical picture • biopsy showing non caseating granuloma
Differential diagnosis •TB•Fungal infections•Lymphoma•Epithelioid tumors of the breast•Lung cancer

Treatment60% has remission spontaneously 10-20% has remission by corticosteroidsThe main goal is to prevent fibrosis (ocular and pulmonary)•Observation•Initiating corticosteroid therapy when appropriate•Monitoring response to therapy•Discontinuing corticosteroids when clinically or physiologically indicated.

Treatment by X-stages •Stage 1 – only observation, if worsening of clinical picture we should start steroids.•Stage 2 – Asymptomatic – observation for 6 months, if no improvement we should treat. Treatment only if symptomatic or Asymptomatic with elevated blood ACE, alteration in relation CD4+\CD8+ or enhanced absorption of gallium 67.•Stage 3 – Treat•Stage 4 – treat if there is still absorption of Gallium 67, if there is not absorption that means that the fibrosis is already formed and disease is not active anymore, so corticosteroids would be useless If there is still absorption of Gallium 67, administer corticoids
Other organs sarcoidosis or extrapulmonaryWe should always treat with corticoisteroid:Vital organs as eyes, nervous system, heart, liver, kidney, spleen.Affection of upper air ways, parotidis, thyroid, cutaneous, specially lupus pernio.Severe forms of articular, bone or muscular sarcoidosisBiochemical alterations such as hyperkalemia, elevated ACE.

Neurosarcoidosis: pulse metilprednisolone IV 500 mg every second day or 1g every week for 4-6 weeks.Ocular sarcoidosis: eyes drops for conjuctivitis or uveitis, but if it is posterior uveitis systemic corticosteroids should be administered.Pulmonary sarcoidosis: inhaled Upper air way sarcoidosis: inhaledCutaneous: with ointments, creams or local injections of corticosteroids.

Treatment
• Topical therapy for cutaneous or ophthalmic disease (eye drops).
• Systemic corticosteroids for patients with unresponsive ophthalmic manifestations, cardiac, neurologic and progressive pulmonary involvement.
• Systemic therapy for patients with hypercalcemia.

Treatment• Prednisone, 20 to 60 mg/d in divided doses or
alternate-day dosing is used for organ involvement that is not life threatening gradually diminishing the dose until the matainence dose of 5 – 10 mg daily or 10-20 alternate day.
• Higher dosage is used off-label for potentially life threatening disease.
• High-dose inhaled corticosteroids may be useful in patients with symptomatic pulmonary disease.

Treatment• Clinical improvement should be assessed after 3
months of corticosteroids. • If no improvement is found, further treatment is
unlikely to be beneficial.• Long term adverse affects of therapy include
weight gain, mood swings, cataracts, GERD, osteoporosis

Other drugsthey are not so useful as corticosteroids, but may help in association to it.NSAIDS: if present erythema nodosum, polyarthritis or acute uveitis.Hydroxichlorquine: chronic fibrotic lesions in lung or skin, 200mg in alternate days for 9 months to avoid ocular toxicity and should be followed by a ophthalmologist.Metothrexate: Lupus pernio or chronic skin lesions, 10mg once per week for 3 months.Azathioprine (50mg 3x daily for 3 months), cyclophosphamide (50mg 1x daily for 3 months) or chlorambucil (5mg 1x daily for 3 months) may be also used to try to diminish corticosteroids intake.Organ transplantation is a choice for whom have lost organs function (pulmonary, liver or kidney), interesting fact is that after transplantation there are formation of non caseating granuloma in the transplanted organ, even in patients in immunosuppressive therapy.

PrognosisMany patients do not require therapy, and their
conditions will spontaneously improve.
Markers for a poor prognosis include :• Advanced CXR stage.• Extrapulmonary disease (predominantly cardiac and neurologic) • Evidence of pulmonary hypertension.• Multiple studies have demonstrated that the most
important marker for prognosis is the initial CXR stage.

Remission• 2/3 of patients with sarcoidosis generally have a
remission within a decade after diagnosis, with few or no consequences; remission occurs for more than half of patients within 3 years.
• Unfortunately, up to 1/3 of patients have progressive disease, leading to clinically significant organ impairment.
• A recurrence after 1 or more years of remission is uncommon (affecting <5% of patients), but recurrent disease may develop at any age and in any organ.

Death
• Less than 5% of patients die from sarcoidosis.
• death is usually the result of pulmonary fibrosis with respiratory failure or of cardiac or neurologic involvement.