Embed Size (px)
Citation preview

Chapter Outline
Temporomandibular Joint Imaging
CHAPTER12
IntroductionAnatomy Common clinical features in TMJ patientsExamination of TMJ
Radiographic imaging of TMJTMJ disordersRadiographic features of TMJ diseasesTMJ ankylosis
INTRODUCTION
Imaging of temporomandibular joint needs proper understanding of joint anatomy and expertise in procedure. It is the only joint which works synchronously at both the ends places anterior to external auditory meatus in glenoid fossa. It can be studied in routine as well as specifi c TMJ radiographic views. Here TMJ imaging along with anatomy discussed in detail.
ANATOMY
Write a short note on radiographic anatomy of TMJ.
Anatomy (Fig. 12.1)
A thorough understanding of radiographic anatomy of TMJ is essential.
Temporomandibular joint constitutes two separate joints anatomically but function as
single unit.A disc composed of fi brocartilage is interposed between condyle and mandibular
fossa. Ligaments and muscles restrict or allow movement of the condyle.
Mainly three structures are important to make up the function, namely condyle,
mandibular fossa, and interarticular disk.Th e condyle is a bony, ellipsoid structure connected to ramus of the mandible by a
narrow neck. Th e extreme aspects of condyle are called medial and lateral poles.A layer of fi brocartilage covers the condyle but is visible radiographically.
Q.
Chapter-12.indd 148Chapter-12.indd 148 7/26/2013 12:35:42 PM7/26/2013 12:35:42 PM

149TEMPOROMANDIBULAR JOINT IMAGING
Th e mandibular and temporal components are calcifi ed by 6 months of age.
Mandibular fossa is located at the inferior aspect of squamous part of temporal bone
and is composed of articular fossa and articular eminence of temporal bone. Th e fossa and articular eminence develop during the fi rst 3 years and young infants lack a defi nite fossa and articular eminence.Interarticular disk composed of fi brous connective tissue is located between the condylar
head and mandibular fossa. Th e disk divides the joint into inferior and superior joint spaces.
Articular surfaces
Th e upper articular surface is formed by articular eminence, anterior part of mandibular fossa and inferior surface is formed by head of mandible.
Articular disc
It is an oval fi brous plate which divides the joint into upper and lower compartments,
the upper compartment permits the gliding movements and lower, rotatory as well as gliding movements. Th e periphery of the disc is attached to fi brous capsule.
Th e ligaments form the supporting system of TMJ.
Fibrous capsule Temporomandibular ligament Sphenomandibular ligament Stylomandibular ligament
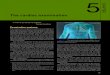
Fig. 12.1. Temporomandibular joint anatomy: (a) Lateral view and (b) coronal view.
1
234
5
6
78
9
10
11
12
1. Articular eminence2. Superior joint space3. Inferior joint space4. Interarticular disk5. Articular tubercle6. Lateral capsular wall7. Lateral collateral ligament8. Medial capsular wall9. Medial collateral ligament10. Mandibular condyle11. Articular surfaces12. Middle cranial fossa
Lateral pterygoid muscle
1. Synovial membrane2. Superior lamina3. Loose areolar connective tissue4. Inferior lamina5. Mandibular condyle6. Synovial membrane7. Inferior belly8. Superior belly9. Articular eminence10. Articular space11. Interarticular disk12. Superior, inferior joint space
Posteriorattachment}
}
67
8
9101112
12
3
4
5
Temporal mandibular joint anatomyLateral view
Temporal mandibular joint anatomyCoronal view
(a) (b)
Chapter-12.indd 149Chapter-12.indd 149 7/26/2013 12:35:43 PM7/26/2013 12:35:43 PM

150ORAL RADIOLOGY: EXAM PREPARATORY MANUAL FOR UNDERGRADUATES
Explain briefl y about TMJ bony relationships.
TMJ Bony Relationships
Radiographic joint space is the general term used to describe the radiolucent area
between the condyle and temporal component.Th e condyle is retruded when posterior joint space width is less than the anterior and
protruded when the posterior joint space is wider than the anterior.Widened joint space is seen in cases involving fl uid or blood within joint and decreased
joint space may indicate bone loss, displacement or perforation of intracapsular components.
Write a short note on TMJ soft tissue relationships.
TMJ Soft Tissue Relationships
Laterally parotid gland and temporal branches of facial nerve.
Medially tympanic plate separates the joint from internal carotid artery.
Anteriorly it is related with lateral pterygoid, master nerve, and vessels.
Posteriorly parotid gland separates the joint from external auditory meatus.
Superiorly it is related with middle cranial fossa and middle meningeal vessels.
Inferiorly it is related with maxillary artery and vein.
COMMON CLINICAL FEATURES IN TMJ PATIENTS
What are the common clinical features of TMJ patients?
Clinical Features
Pain in the TMJ or ear or both.
Headache, muscle tenderness, and joint stiff ness.
Clicking or other joint noises.
Reduced range of motion.
Signs include swelling in and around the joint, rise of temperature and redness on
overlying skin.
EXAMINATION OF TMJ
Describe various examinations of temporomandibular joint.
Th e TMJ is located anterior to auditory meatus. Th ey are palpated bilaterally and fi ndings of both sides are compared.
Functional Examination of Masticatory System
Th e masticatory system comprises of three functional units
Th e TMJ.
Masticatory muscles.
Occlusion.
Q.
Q.
Q.
Q.
Chapter-12.indd 150Chapter-12.indd 150 7/26/2013 12:35:43 PM7/26/2013 12:35:43 PM

151TEMPOROMANDIBULAR JOINT IMAGING
Each unit infl uences the other two. Examination of one unit of masticatory system
must include the other two.
Components of Physical Examination of TMJ
Inspection.
Palpation.
Assessment of range of movement of mandible.
Provocation tests.
Intraoral examination.
Assessment of range of movement of mandible
Comfort of opening the mouth to a maximum with assistance (normal is � or �40).Observed for lateral and protrusive movements.
Interincisor separation plus and (or) minus the incisor overlap in central occlusion
provides the measure of mandible movements.
Intraoral examination
Check for lip bite, tongue borders, occlusive tooth wear mobility, and generalized sensitivity.
Occlusion
Functional malocclusion.
Morphological malocclusion.
Occlusal tooth wear and facets.
Enumerate TMJ imaging modalities.
Techniques for radiographic imaging of TMJ:Panoramic radiography.
Specifi c TMJ viewsTranscranial
Transpharyngeal
Transorbital
Conventional skull view
Submentovertex
Reverse Towne’s view
Arthrography.
Computed tomography.
Magnetic resonance imaging.
PANORAMIC RADIOGRAPHY/ RADIOGRAPHIC IMAGING OF TMJ
Write about radiographic imaging of TMJ.
Regular orthopantomograph shows TMJ of both the sides in single image which allows
comparing right side to left side.
Q.
Q.
Chapter-12.indd 151Chapter-12.indd 151 7/26/2013 12:35:43 PM7/26/2013 12:35:43 PM

152ORAL RADIOLOGY: EXAM PREPARATORY MANUAL FOR UNDERGRADUATES
A specifi c TMJ projection allows making image of one side or both sides in open and
closed position, which is optional (Fig. 12.2).
Enlist the specifi c TMJ projections.
Specifi c TMJ views are:Transcranial view.
Transpharyngeal view.
Transorbital view.
Submentovertex view.
Reverse Towne’s view.
Write about transcranial TMJ view.
Transcranial View for TMJ (Fig. 12.3).
Patient positioning: Patient head rotated through 90° so that the TMJ is touching the fi lm and the sagittal plane of head parallel to the fi lm.Cone adjustments: Th e X-ray tube is directed downwards, 25° to the area of interest, and 20° horizontally anterior angulation.Exposure parameters: 70 kVp, 8 mA, and exposure time 1.5 s.
Q.
Q.
Fig. 12.2. TMJ open and closed position of right and left sides.
Fig. 12.3. Transcranial view: (a) Patient positioning, (b) angulation, and (c) radiograph.
(a) The central ray is oriented at a 25-degree positive anglefrom the opposite side (b) and anteriorly 20-degrees, centeredover the TMJ of interest.
20°
(b)(a)
25°
Transcranial projection
(a) (b) (c)
Chapter-12.indd 152Chapter-12.indd 152 7/26/2013 12:35:43 PM7/26/2013 12:35:43 PM

153TEMPOROMANDIBULAR JOINT IMAGING
Explain transpharyngeal TMJ view.
Transpharyngeal View (Fig. 12.4).
Also called ‘ Parma’ view.Patient positioning: Patient holds the cassette against the side of the face over the TMJ area of interest with fi lm and the sagittal plane of the head are parallel and keep the mouth openCone adjustments: Th e X-ray beam is directed superiorly at 5–10° to the sigmoid notch of the opposite side and 10° posteriorly from the sigmoid notch on the side of cone to side of interest/opposite side.Exposure parameters: 70 kVp, 8 mA, and exposure time 0.8 s.
Fig. 12.4. Transpharyngeal view: (a) Patient positioning, (b) angulation, and (c) radiograph.
(a) (b) (c)
(a) The central ray is oriented superiorly 5 to 10 degrees and(b) Posteriorly approximately 10 degrees, centered over theTUJ of interest.
10°
(b)(a)
Transpharyngeal projection
5° to 10°
Describe transorbital TMJ view.
Transorbital View (Fig. 12.5).
Patient positioning: Head is tilted down 10° so that the canthomeatal line is horizontal. Patient holds the cassette behind the ear.Cone adjustments: Th e X-ray beam is directed from the front of the patient through the contralateral orbit.Exposure parameters: 70 kVp, 8 mA, and exposure time 1.0 s.
Q.
Q.
Fig. 12.5. Transorbital view: (a) Patient positioning, (b) angulation, and (c) radiograph.
The central ray is oriented downward approximately 10degrees and laterally approximately 30 degrees though theipsilateral orbit centered over the TMJ of interest
(b)(a)
Transorbital projection
(a) (b) (c)
30°
10°
Chapter-12.indd 153Chapter-12.indd 153 7/26/2013 12:35:43 PM7/26/2013 12:35:43 PM

154ORAL RADIOLOGY: EXAM PREPARATORY MANUAL FOR UNDERGRADUATES
Describe the following conventional skull views for radiographic evaluation of TMJ
Submentovertex view
Reverse Towne’s view.
Submentovertex View (Fig. 12.6).
Procedure of the submentovertex view is described
in the chapter ‘Extraoral Imaging’.Submentovertex view gives a clear picture to identify
laterally displaced fractures of condyle on either side when viewed from submental region.
Reverse Towne’s View (Fig. 12.7)
Procedure of the reverse Town’s view is described
in the chapter ‘Extraoral Imaging’.Reverse Towne’s view gives a clear picture to
identify laterally displaced fractures of condyle on either side when viewed from anterior.
Write a brief note on the following imaging techniques of TMJ.
ArthroscopyMRI
Computed tomography
Arthrography (Fig. 12.8).
A radiographic dye will be injected into the spaces above or below the disc.
And a tomographic image will be taken.
Q.
Q.
Fig. 12.8. (a) Diagram on cadaver section showing injecting site and (b) arthrograph.
(a) (b)
Fig. 12.6. TMJ in submentovertex view.
Fig. 12.7. TMJ in reverse Towne’s view.
Chapter-12.indd 154Chapter-12.indd 154 7/26/2013 12:35:43 PM7/26/2013 12:35:43 PM

155TEMPOROMANDIBULAR JOINT IMAGING
Selecting the site of injection and the technique needs expertise.
Mistake or wrong procedure may perforate the disc.
Computed Tomography (Fig. 12.9).
Computed tomography gives possible sectioned views of TMJ.
Various vertical, cross-sectional and oblique sections of TMJ on either sides can be
taken to study normal anatomy, fractures, tumors and other diseased conditions of TMJ.
Fig. 12.9. Computed tomography of various sections of TMJ.
Magnetic Resonance Imaging (MRI) (Fig. 12.10)
Magnetic resonance image of TMJ can give images of hard tissue as well as soft tissue
components of TMJ which is having better diagnostic quality than CT, as capsule and ligaments also can be seen along with bony components like condyle and glenoid fossa.
Fig. 12.10. MRI image of TMJ in open and closed mouth positions in T1 and T2 images.
Chapter-12.indd 155Chapter-12.indd 155 7/26/2013 12:35:43 PM7/26/2013 12:35:43 PM

156ORAL RADIOLOGY: EXAM PREPARATORY MANUAL FOR UNDERGRADUATES
T1 and T2 images in open and closed mouth positions will help to compare both sides
in diff erent contrast images of TMJ.
TMJ DISEASES
Enlist the classifi cation of TMJ diseases.
Developmental
Condylar agenesis
Condylar hypoplasia
Condylar hyperplasia
Bifi d condyle
Juvenile arthrosis
Coronoid hyperplasia
Infl ammatory
Arthritis (septic, rheumatoid, gout, psoriasis)
Synovitis/capsulitis/ retrodiscitis
Polyarthritis
Degenerative
Osteoarthrosis
Osteoarthritis
Juvenile idiopathic arthritis
Functional
Subluxation
Luxation
Ankylosis
Abnormality within the joint
Internal derangement with or without reduction
Disc perforation
Adhesion
Eff usion
Myogenous
Myositis
Myospasm
MPDS
Contracture
Hypertrophy
Fibromyalgia
Neoplasms aff ecting the joint
Benign: Osteoma, osteochondroma, Langerhans histiocytosis and osteoblastoma.Malignant: Osteogenic sarcoma, chondrosarcoma, synovial sarcoma, and fi brosar-coma of the capsule.
Q.
Chapter-12.indd 156Chapter-12.indd 156 7/26/2013 12:35:43 PM7/26/2013 12:35:43 PM

157TEMPOROMANDIBULAR JOINT IMAGING
RADIOGRAPHIC FEATURES OF TMJ DISEASES
Developmental disorders occur either due to genetic or environmental factors.
Describe radiographic features of absence of condyle.
Condylar Aplasia/Agenesis
Refers to absence of condyle, which is extremely rare when not associated with
syndrome.It may be unilateral or bilateral and is usually associated with hemifacial microstomia,
Treacher-Collins syndrome, and Goldenhar syndrome, proteus syndrome, Morquio syndrome and auriculo-condylar syndrome.Cause: Disturbance in the development of TMJ before 10th week of fetal stage.Clinically: Facial asymmetry, deviation of the midline and mandible towards aff ected side on opening the mouth, and malocclusion.Radiographically: Complete absence of the condyle, facial asymmetry and deviation of the midline can be appreciated well in computed tomography and CBCT.
Describe radiographic features of condylar hypoplasia.
Condylar Hypoplasia
Refers to undergrowth or failure to attain normal size of the condyle.
It may be congenital or acquired.
It may be inherited or appear spontaneously.
It may be unilateral or bilateral.
Cause: For acquired hypoplasia includes trauma to TMJ, forceps delivery, irradiation or infection during growth and development, and endocrinal disturbances, etc.Clinically: Facial asymmetry, deviation of the mandible to the aff ected side on opening the mouth, and crowding of the teeth are noted.Radiographically
Aff ected condyle is smaller, however morphology is normal.
Proportionately mandibular fossa, ramus, and body of the mandible are also small.
Posterior border of the ramus and condylar neck may have posterior (dorsal)
inclination.Antegonial notch is prominent.
Treatment: Surgical correction of the joint using graft, orthognathic surgery, and orthodontic correction to maintain the function.
Explain the radiographic features of condylar hyperplasia.
Condylar Hyperplasia
Refers to overgrowth or enlargement of the condyle.
It is usually unilateral accompanied by hyperplasia of the same side.
Q.
Q.
Q.
Chapter-12.indd 157Chapter-12.indd 157 7/26/2013 12:35:43 PM7/26/2013 12:35:43 PM

158ORAL RADIOLOGY: EXAM PREPARATORY MANUAL FOR UNDERGRADUATES
Cause: Presence of overreactive cartilage or persistent cartilaginous rests in the condylar head, increasing the thickness of entire cartilaginous and precartilagenous layers provoked by trauma or endocrinal disturbance.Clinically: Progressive facial asymmetry, enlargement of the condyle, deviation of the mandible to the unaff ected side on opening the mouth, open bite, and limited joint movement are noted.Radiographically: Orthopantomograph shows the aff ected condyle longer than the unaff ected side.Treatment: Orthognathic surgery along with orthodontic correction for correction of the defect.
Write about bifi d condyle, juvenile arthrosis, and coronoid hyperplasia.
Bifi d Condyle/trifi d Condyle
Refers to division of the condylar head into two or three parts by deep notches or
depressions in the frontal or sagittal planes.It may be unilateral or bilateral.
Cause: Persistence of fi brous septa between the condylar cartilage, rupture of septal vessels secondary to trauma, exposure to teratogenic substances, irradiation, and nutritional defi ciencies during growth and development.Clinically: Patients are asymptomatic.Radiographically
It is an incidental fi nding during radiographic investigation. a deep notch dividing
the condylar head is seen on the superior surface of the condyle.Glenoid fossa may be one or separate to accommodate each part of the condylar head.
Computed tomography and three-dimensional reconstruction delineate the
morphology better.Treatment: As it is asymptomatic, no treatment is required.
Juvenile Arthrosis ( Boering Arthrosis)
It refers to hypoplasia of the condyle due to growth disturbance.
It aff ects children and adolescents.
It may be unilateral or bilateral.
Clinically: Facial asymmetry with signs and symptoms of dysfunction.Radiographically: Marked fl attening and elongation of the articular surface gives the condyle a toad stool appearance, even the temporal surface is fl attened, neck of the condyle is short or absent, ramus is short with prominent antegonial notch.Treatment: Orthognathic surgery along with orthodontic treatment for correction of asymmetry and to prevent the further destruction of the condyle.
Coronoid hyperplasiaRefers to elongation of the coronoid process (more than or equal to 1 cm) beyond the
medial surface of the zygomatic arch.It can be unilateral or bilateral and it can be genetic or acquired.
Q.
Chapter-12.indd 158Chapter-12.indd 158 7/26/2013 12:35:43 PM7/26/2013 12:35:43 PM

159TEMPOROMANDIBULAR JOINT IMAGING
Cause: For acquired hyperplasia includes trauma, increased temporalis muscle activity, and endocrinal disturbances.Clinically: Progressive limitation in the mouth opening.Radiographically: Waters’ view, orthopantamograph and axial computed tomography in open mouth position demonstrate the ‘drumstick appearance’ of hyperplastic coronoid.Treatment: Surgical correction of coronoid process.
Describe radiographic features of arthritis aff ecting TMJ.
Rheumatoid Arthritis
It refers to chronic infl ammation of the synovial lining of the joint leading to proliferation
of synovial granulomatous (pannus) into the articular surface causing destruction of articular surface and fi brous ankylosis.
It aff ects multiple joints, usually beginning in interphalangeal and wrist joint.
Involvement of TMJ may be unilateral or bilateral.
Clinically: Periods of exacerbation and remissions in the symptoms like pain, joint stiff ness, limited mouth opening and joint sounds.Radiographically:
Early changes include osteopenia and reduced density of the bone.
As the disease progresses erosion of the articular surface with anterosuperior
positioning of condyle occurs giving it a ‘sharpened pencil’ appearance.In severe cases condyle may be completely destroyed.
Treatment: Palliative measures for relief of pain and restoration of function.Intra-articular injection of steroids.
In severe cases, joint replacement therapy may be considered.
Write about osteoarthritis.
Osteoarthritis
It refers to degeneration of articular soft tissue and remodeling of the underlying
bone usually resulting from ageing (primary osteoarthritis) or parafunctional habits (secondary osteoarthritis).During early stages deterioration of the soft tissue occur followed by erosive changes
involving bot the temporal and condylar bones leading to sclerosis, subcondylar cysts ( cysts of Elyes) and peripheral osteophyte formation.Clinically: Limited mouth opening, pain and tenderness over the TMJ, and deviation of the mandible towards aff ected side on opening the mouth are noted.Radiographically: In early stages, bony changes may not be evident. Later narrowing of the joint space, fl attening of the articular surface, sclerosis, subcondylar cysts, and osteophyte formation lying freely in the joint space (joint mice) are noted.Treatment: correctional of parafunctional habits along with symptomatic measures for pain relief like analgesics, soft diet, restricted mouth opening, and hot fomentation over joint are indicated. In severe cases, surgical treatment is performed.
Q.
Q.
Chapter-12.indd 159Chapter-12.indd 159 7/26/2013 12:35:43 PM7/26/2013 12:35:43 PM

160ORAL RADIOLOGY: EXAM PREPARATORY MANUAL FOR UNDERGRADUATES
Explain the features of juvenile chronic arthritis.
Juvenile Chronic Arthritis ( Still’s Disease/ Juvenile Idiopathic Arthritis)
It refers to chronic, intermittent infl ammation of the synovial membrane leading to
synovial hypertrophy, joint eff usion, and degenerative changes in the articular surface.It occurs before sixteen years of age.
It can involve one or more joints (polyarthrits).
It may be unilateral or bilateral.
In 40% of cases involvement of TMJ is seen.
Clinically: Facial asymmetry, pain, and tenderness in the joint and restricted mouth opening noted, other fi ndings include micrognathia and anterior open bite.Radiographically: Degenerative changes like sclerosis, erosion of articular surface with anterosuperior positioning of the condyle, osteophyte formation may occur. In severe cases condyle may be completely destroyed.
Describe radiographic features of subluxation of TMJ?
Subluxation (Hypermobility, Partial Dislocation)
It refers to positioning of the condyle anterior to the articular eminence and which can
be reduced by the patient.Cause: Joint laxity as seen in Ehlers–Danlos syndrome, change in fossa and eminence architecture, and iatrogenic during prolonged mouth opening (endodontic procedures, third molar extraction, endotracheal intubation).It may be unilateral or bilateral.
Clinically: Locking of the jaw on opening the mouth wide and on manipulation of the jaw for closure result in joint sound (due to movement of condyle over articular eminence) and it may be associated with pain in chronic conditions.Radiographically: Excessive translation of the condyle is noted.Treatment: Includes injecting sclerosing agent and in severe cases surgical treatment is required.
Describe radiographic features of TMJ dislocation?
Dislocation ( Open Lock)It refers to positioning of the condyle anterior to the articular eminence and that cannot
be reduced by the patient.It is usually bilateral and occurs due to trauma.
Clinically: Patient presents with open mouth position associated with pain and muscle spasm. If unilateral dislocation occurs deviation of the mandible to the unaff ected side is noted. Radiographically: Condyle is located anterior and superior to the articular eminence.Treatment: Guiding the condyle into the glenoid fossa by manipulation of the mandible followed by immobilization of the jaw with strap bandages around the head and restricting the wide opening of mouth for 2 weeks.
Q.
Q.
Q.
Chapter-12.indd 160Chapter-12.indd 160 7/26/2013 12:35:43 PM7/26/2013 12:35:43 PM

161TEMPOROMANDIBULAR JOINT IMAGING
TMJ ANKYLOSIS
Discuss about TMJ ankylosis.
TMJ Ankylosis (Fig. 12.11).
Ankylosis or joining of two counterparts of the joint.
It can be congenital, traumatic, or unknown in origin.
Congenital may be due to forceps delivery and childhood traumas may lead to
ankylosis.It can be fi brous or bony or pseudotype of ankylosis.
It can be unilateral or bilateral involvement.
It will be manifested as limited or restricted mouth opening or deviations.
In case of early occurrence in life, it may lead to underdevelopment of the jaw on one
side or both the sides.It refers to fusion or adhesion between the condyle and the glenoid fossa.
It is a Greek word meaning ‘stiff joint’.It may be
True/False or pseudoankylosis.
Fibrous/bone/fi bro-osseous ankylosis.
Unilateral/bilateral ankylosis
Partial/complete ankylosis.
True ankylosis (intra-articular): Refers to bony or fi brous adhesion between the articular surfaces of the TMJ. True ankylosis may be partial/incomplete. Ankylosis refers to incomplete union between articulating surfaces.
Complete ankylosis refers to complete union between articulating surfaces.
Fibrous ankylosis: Refers to fi brous union between articulating surfaces. False ankylosis (extra-articular): Refers to restricted mandibular movement secondary to conditions like muscle spasm, myositis ossifi cans, and coronoid hyperplasia.Cause: trauma during forceps delivery, spread of middle ear infection, parotid abscess, mastoiditis, infratemporal, submassetric or parapharyngeal infections into TMJ,
Q.
Fig. 12.11. Radiographic image of ankylosed TMJ.
Chapter-12.indd 161Chapter-12.indd 161 7/26/2013 12:35:43 PM7/26/2013 12:35:43 PM

162ORAL RADIOLOGY: EXAM PREPARATORY MANUAL FOR UNDERGRADUATES
prolonged immobilization of jaws or muscle splinting, comminuted condylar fracture especially in children, arthritis, infl ammatory conditions, and neoplasms.Clinically
In case of unilateral ankylosis: Unilateral vertical defi ciency, fullness, and deviation of mandible towards the aff ected side, mouth opening is restricted, deviation of the midline towards the aff ected side and cross bit on the unaff ected side are noted.In case of bilateral ankylosis: Convex profi le, retrognathic mandible, short ramus, small body, small chin giving ‘Bird-face’ or ‘Andy Gump’ appearance. Other fi ndings include incompetent lips, open bite, severe crowding, and poor oral hygiene maintenance.
Radiographically
In fi brous ankylosis, joint space appears narrow with irregularities in the articular
surface.In bony ankylosis, joint space may be partly or completely obliterated by irregular
bone mass. Secondary degenerative changes may be seen.Treatment: Includes surgical correction of the deformity and restore the mandibular function.
Write about internal derangement.
Internal Derangement
It refers to abnormality in the articular disc position and morphology relative to
condyle.Displacement of the disc is often in anterior direction; however, it may be displaced
anteromedially or anterolaterally.Lateral and posterior displacement is rare.
Cause: Parafunctional habits (bruxism and clenching).In normal TMJ, during mouth opening the condyle translates and the biconcave disc gets stretched and lies between the condylar head and the articular eminence. During closure as the condyle moves backward, the disc recoils to its normal position.In anterior disc displacement with reduction: Th e disc lies displaced with its posterior band lying anteriorly. During opening as the condyle translates the disc snaps back to its normal location producing a click (opening click).
While closing disc returns to its displaced position producing a click ( reciprocal click).Clinically: Patients may or may not be symptomatic. Restricted movement of the jaw, deviation of the mandible towards aff ected side, clicking sound both on opening and closing the jaw are noted.
In anterior disc displacement without reduction: Th e anteriorly displaced disc remains static both on opening and closing the mouth.
Locking of the disc ( gum ball eff ect) results in restricted condylar translation.Clinically: Pain and severe limitation in mouth opening, limited lateral and protrusive movement, mandible is deviated towards same side, joint crepitus is
Q.
Chapter-12.indd 162Chapter-12.indd 162 7/26/2013 12:35:43 PM7/26/2013 12:35:43 PM

163TEMPOROMANDIBULAR JOINT IMAGING
heard on opening and closing the mouth. Episodes of open and closed locking of the jaw are noted.Radiographically: MRI and arthrography demonstrates the disc morphology and position.Treatment: Analgesics for symptomatic relief of pain along with anterior repositioning splints and physiotherapy are indicated.
FAQs
1. Enumerate the radiographic views in which TMJ can be evaluated.
2. Explain the specifi c TMJ views.
3. What is Parma view?
4. Describe the transcranial, transpharyngeal, and transorbital TMJ imaging.
Chapter-12.indd 163Chapter-12.indd 163 7/26/2013 12:35:44 PM7/26/2013 12:35:44 PM