Embed Size (px)
Citation preview
1
Extracorporeal Membrane Oxygenation (ECMO)
15 November 2014
Dr. Esther Wong PhD; MSc; RM; RN President, Hong Kong College of Critical Care Nursing
Adjunct Professor, Girne American University, H.K.
1
10th International Congress of World Federation of Critical Care Nurses (WFCCN)

2
An Overview of ECMO
I. Introduction to Extracorporeal Membrane Oxygenation (ECMO)
II. Trends of ECMO Use WorldwideIII. ECMO Service Development in Hong KongIV. Extracorporeal Life Support (ECLS) ProgramsV. ANP & APN in ECLS ServiceVI. The Way Forward
2
33
What is ECMO? 體外膜 合 氧 (人工肺 /人工心肺 )ECMO = Extracorporeal Membrane Oxygenation • Initially used to describe long-term extracorporeal
support that focused on the function of oxygenation.• Subsequently, in some patients, the emphasis shifted
to removal of carbon dioxide.

ECMO / ECLS• Is not the same as cardiopulmonary bypass .
• It serves as a bridging therapy and it is not a curative therapy. That means ECMO may be used as bridge to recovery (i.e. buying time for patient to recover); bridge to decision (i.e. provide temporary support to patient and allow clinicians to decide on the next step); or bridge to transplant (i.e. provide support to patient while awaiting suitable donor organ).
A New Term – ECLS= Extracorporeal Life Support
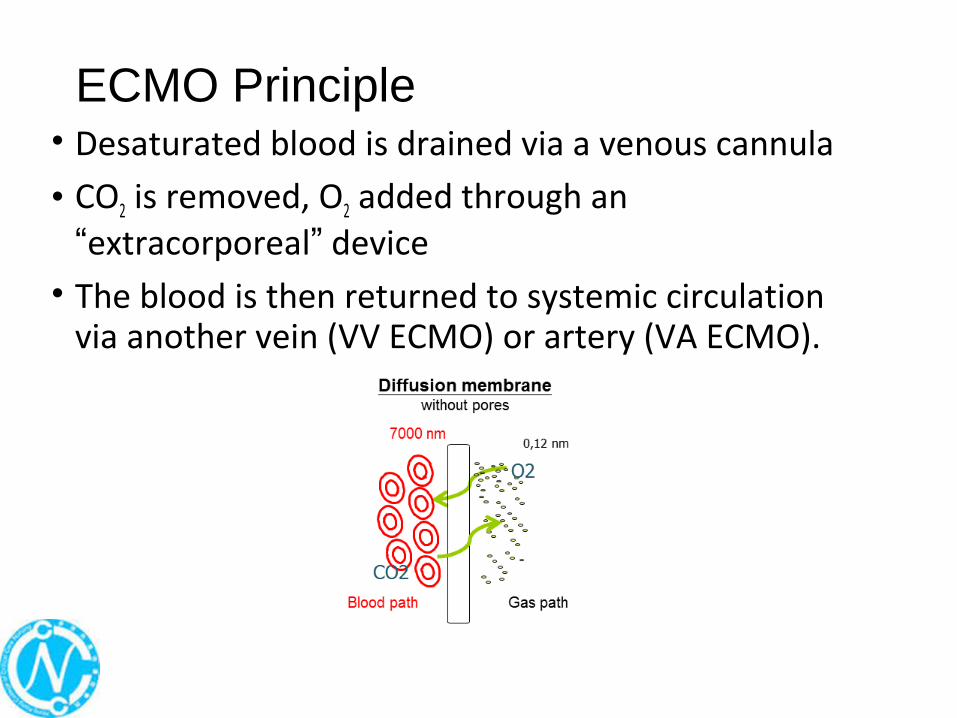
ECMO Principle• Desaturated blood is drained via a venous cannula
• CO2 is removed, O2 added through an “extracorporeal” device
• The blood is then returned to systemic circulation via another vein (VV ECMO) or artery (VA ECMO).

66
Different Configurations in ECMO
Most common configurations:•Veno-venous ECMO (VV-ECMO):
• Used to support patients with severe respiratory failure refractory to conventional therapies
• Blood is drawn from a central vein, pass through an ECMO machine and then returned back via a central vein
•Veno-arterial ECMO (VA-ECMO):• Used to support patients with severe cardiac failure
(with or without respiratory failure) • Blood is drawn from a central vein, pass through an
ECMO machine and then returned back via a central artery

77
VV-ECMO VA-ECMO
88
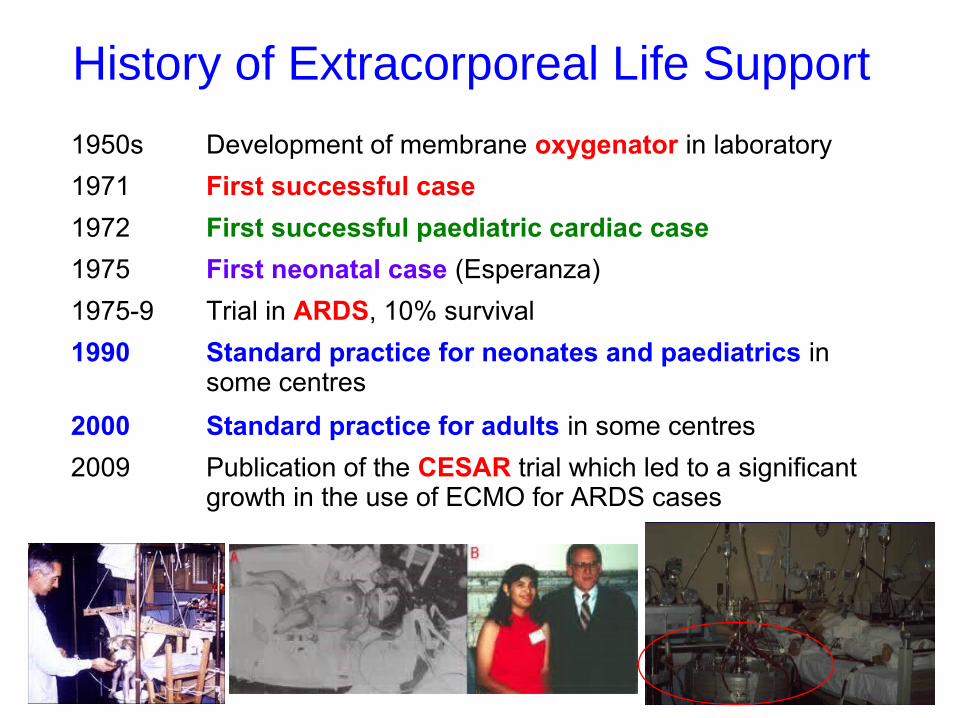
History of Extracorporeal Life Support
1950s Development of membrane oxygenator in laboratory
1971 First successful case
1972 First successful paediatric cardiac case
1975 First neonatal case (Esperanza)
1975-9 Trial in ARDS, 10% survival
1990 Standard practice for neonates and paediatrics in some centres
2000 Standard practice for adults in some centres
2009 Publication of the CESAR trial which led to a significant growth in the use of ECMO for ARDS cases
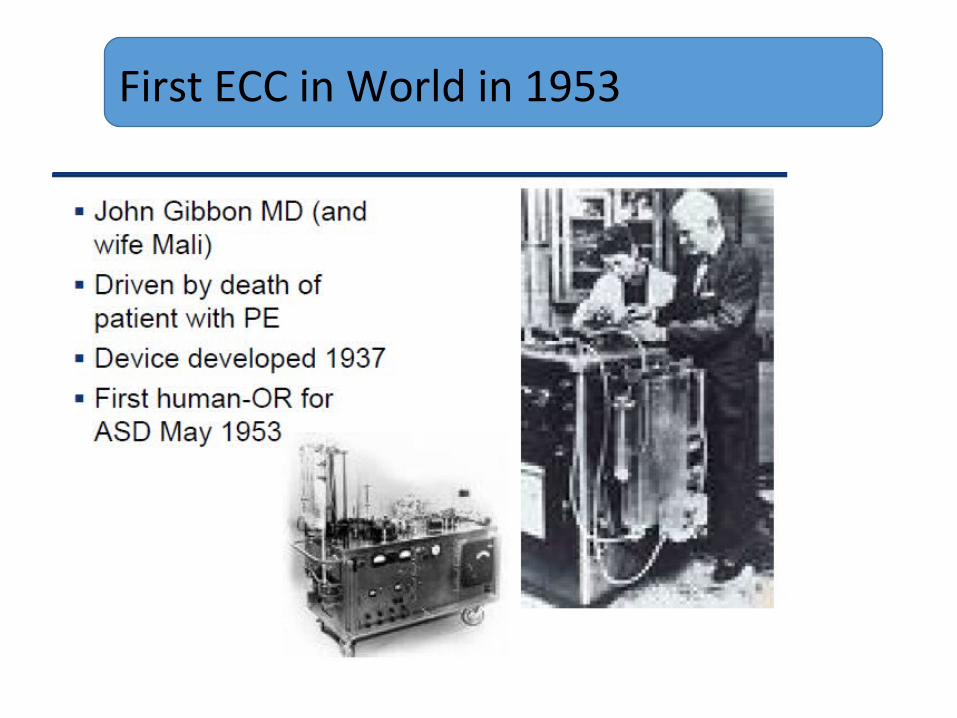
First ECC in World in 1953
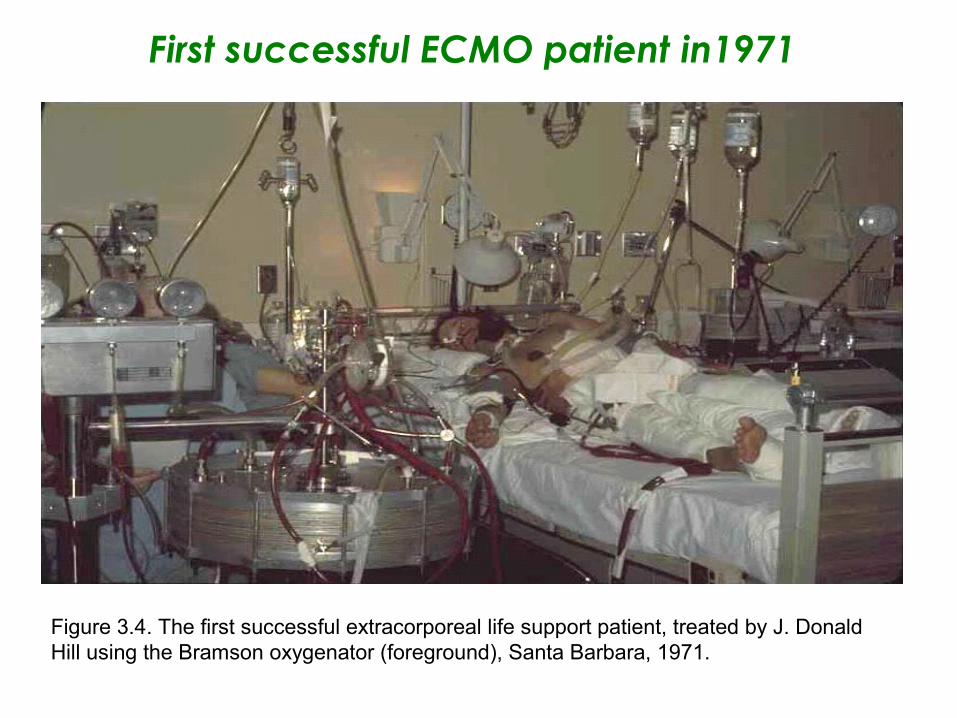
First successful ECMO patient in1971
Figure 3.4. The first successful extracorporeal life support patient, treated by J. Donald Hill using the Bramson oxygenator (foreground), Santa Barbara, 1971.
1111
Indications for Initiation of ECMO1. ELSO’s Criteria
• Acute severe cardiac or pulmonary failure that is potentially reversible and unresponsive to conventional management
2. For VV & VA ECMO
• Veno-venous ECMO provides support for severe respiratory failure without major cardiac dysfunction (Salamonsen, 2007) Examples: Severe pneumonia; ARDS; Status asthmaticus or Pulmonary contusion; and Acute lung (graft) failure following transplant
• Veno-Arterial ECMO provides support for severe cardiac failure (with or without respiratory failure) (Salamonsen, 2007) Examples: Cardiogenic shock ; Cardiomyopathy; Acute Myocarditis; Drug overdose with profound cardiac depression; Sepsis with profound cardiac depression; Post-cardiac surgery (unable to wean from cardiopulmonary bypass) and Primary graft failure (post heart/heart-lung transplant) or as a bridge to cardiac transplantation.
Considerations for Initiation of ECMO
• Less suitable for the lung conditions requiring long time to heal (complication risk > benefits).
• Pre-existing conditions that affect the quality of life (Prior Severe Neurological injury or CNS bleed; Poor Prognosis for Primary Disease such as end stage malignancy, multi-organ failure; risk of systemic bleeding when using anticoagulation).
• Age and size of patients (Too old or small size < 2kg).
• Futility e.g. too sick or on prolonged conventional therapy with a fatal diagnosis.
(Contraindications are relative and Vary widely)

Parameter / Score 0 1 2 3 4
PaO2/FiO2 (On 100%
Oxygen)
≥300mmHg
≥40kPa
225-299
30-40
175-224
23-30
100-174
13-23
<100
<13
CXR normal 1 point per quadrant infiltrated
PEEP(cmH2O) ≤5 6-8 9-11 12-14 ≥15
Compliance (ml/cmH2O)
≥80 60-79 40-59 20-39 ≤19
VV ECMO inclusion criteria - Murray score= average score of all 4 parameters

ECMO UseWorldwide Trend

1515
Trends of ECMO Use
• Since 2009, ECMO practice has evolved significantly due to:
Better patient outcomes supported by clinical evidence Wider acceptance by clinicians Improved technology with more user-friendly
equipment, enhanced portability and better cannulas and circuitry
• This results in a growth in ECMO centres and ECMO use
CESAR StudyConventional ventilation or ECMO for Severe Adult Respiratory failureLancet 2009, 374:1351-63
Single ECMO centre at Glenfield Hospital, UK
• ECMO: 57 in 90 patients (63%)• Conventional ventilation: 41 in 87 patients (47%)
• Relative risk reduction in favour of ECMO0.69 (0.05–0.97; P = 0.03)
Significant Study and Result
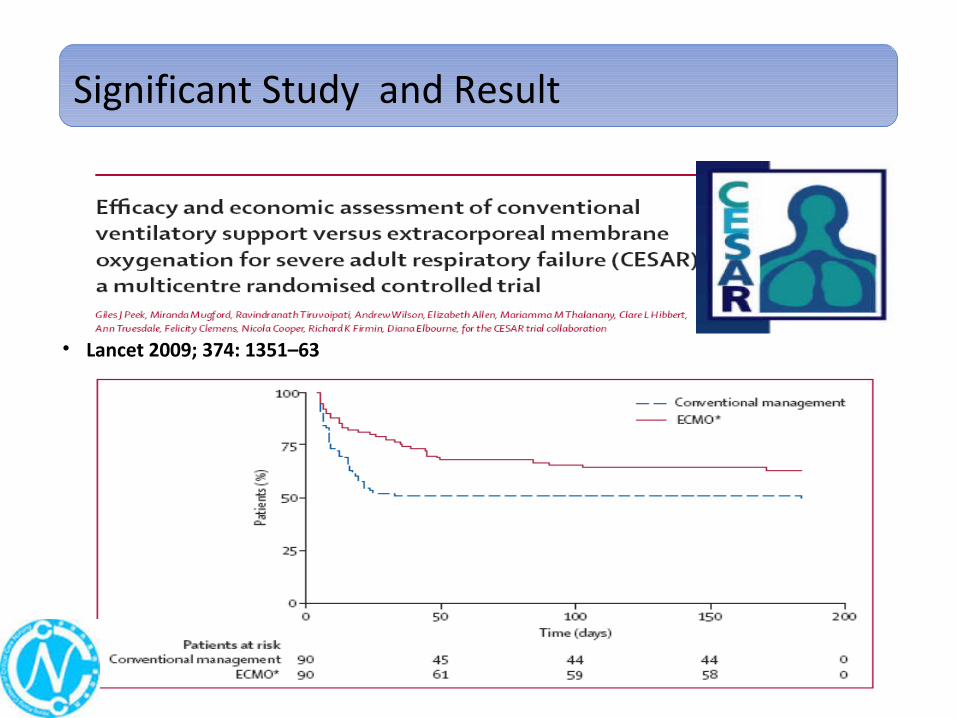
• Lancet 2009; 374: 1351–63
Significant Study and Result

ECMO for 2009 Influenza A(H1N1)Acute Respiratory Distress SyndromeThe Australia and New Zealand Extracorporeal Membrane Oxygenation (ANZ ECMO) Influenza InvestigatorsJAMA. 2009;302(17):1888-1895. Published online October 12, 2009(doi:10.1001/jama.2009.1535)
• During winter 2009 (1 June 2009 to 31 August 2009), Australia & New Zealand ICUs
• Out of 133 patients with IPPV 68 patients required ECMO
• For patients given ECMO• 48/68 (71%) survived ICU
• 32/68 (47%) survived hospital• 16/68 (24%) still in hospital
• 6/68 (9%) still in ICU• 14/68 (21%) died
Significant Study and Result

1919
Trends in ECLS (ELSO, 2014)

2020
ECLS Registry Report
January 2014
2121
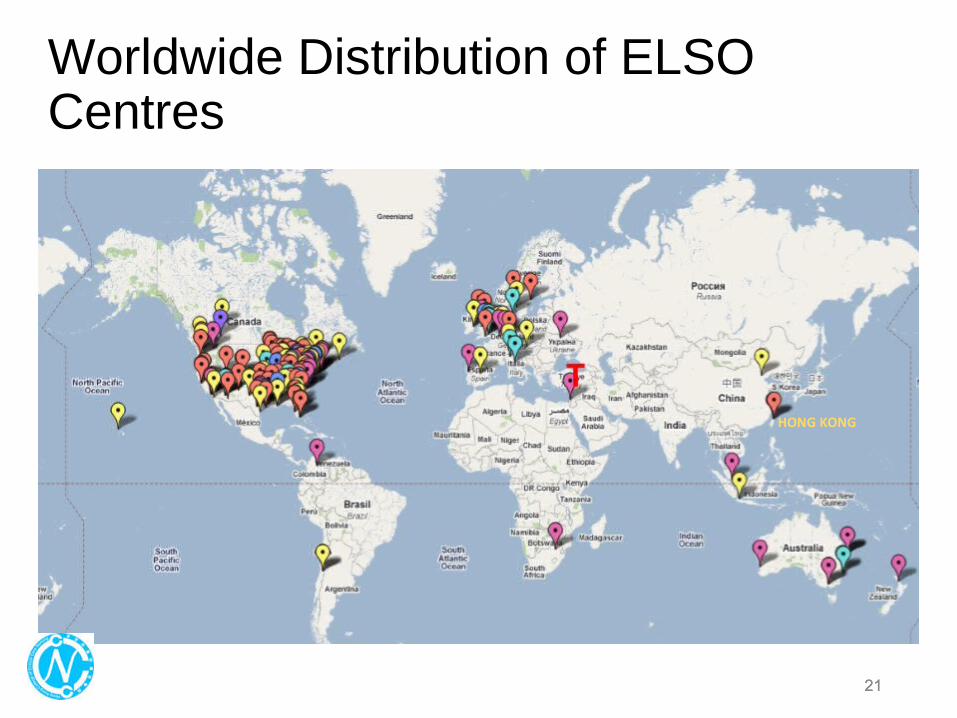
Worldwide Distribution of ELSO Centres
HONG KONG

22
ECMO Service Development in Hong Kong
22

Milestones for ECMO Use in HK
Pioneered by The University of Hong Kong• 1964 – First Open Heart Surgery.• 1968 – First CPB.• 1992 – First Heart Transplant.• 2000 – ECMO for paediatric service.

24
Overall situation in Hong Kong
• Catchment population: 7.1 million• ECMO service is available in both public and private hospital• Conducts more than a total of 100 VV- and VA-ECMO cases
per year• Average ECMO Days in ICU: 5 – 7 days• Survival rate: similar to international benchmarks
• Over 250 doctors and nurses have received ECMO trainings
24

25
Milestones of ECMO use for adult intensive care in Hong Kong• ECMO was first used in cardiothoracic surgical centres and
cardiac centres Intensive care of Hospital Authority introduced ECLS program in 2010
• Kicked off by introducing a co-joint training program from The Alfred ICU, Australia.
• Initially 4 centres provided limited VV-ECMO service• Now has 5 ECMO centres in the public hospitals to provide 24 x
7 coverage for both VV- and VA-ECMO service to critically ill adult patients
• 2 Private Hospitals (HK Adventist & HKS&H) also provide service to cardiac patients.
25

26
ECMO Centres in Public Hospitals• The 5 ECMO centres under intensive care of Public
Hospitals in Hong Kong:1- Queen Elizabeth Hospital2 - Queen Mary Hospital3 - Pamela Youde Nethersole Eastern Hospital4 - Prince of Wales Hospital
5 - Princess Margaret Hospital
26
AB C
D
E
SARS in 2003
• 1755 victims, 386 healthcare workers• 299 death, 8 healthcare workers• Option of ECMO actively explored
Considered “unavailable”
“Partial bypass” as backup in Cath Lab

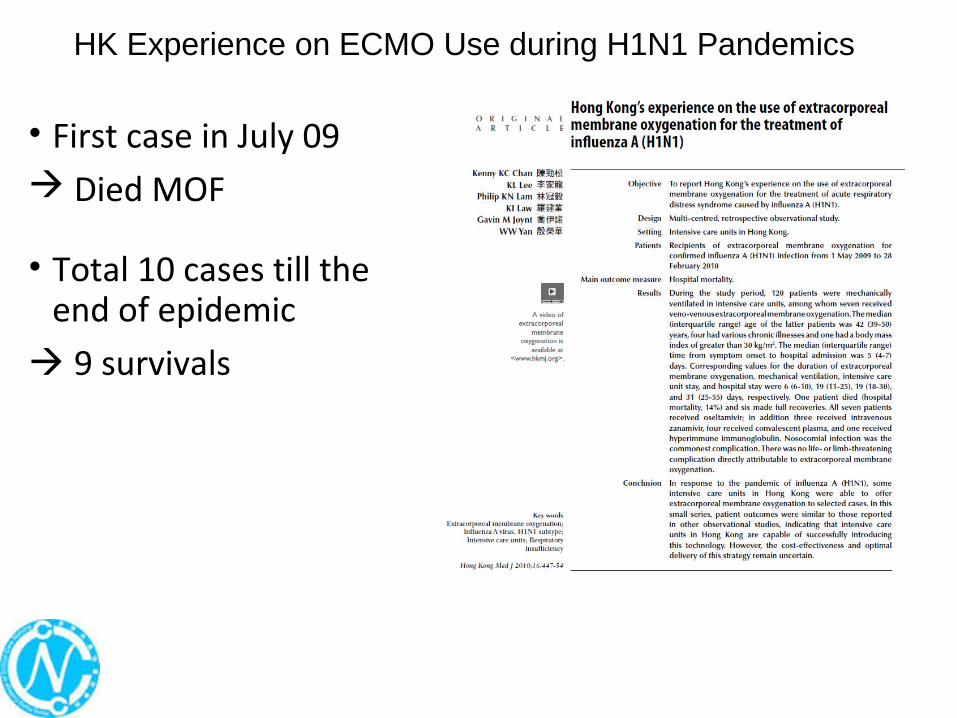
HK Experience on ECMO Use during H1N1 Pandemics
• First case in July 09 Died MOF
• Total 10 cases till theend of epidemic
9 survivals
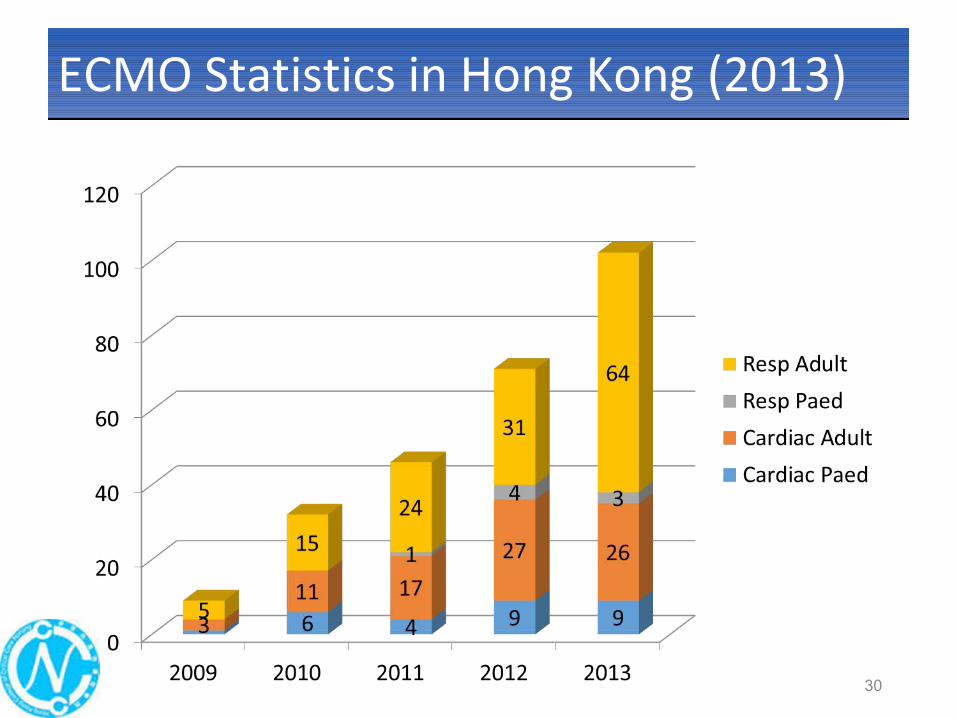
ECMO Statistics in Hong Kong (2013)ECMO Statistics in Hong Kong (2013)
30
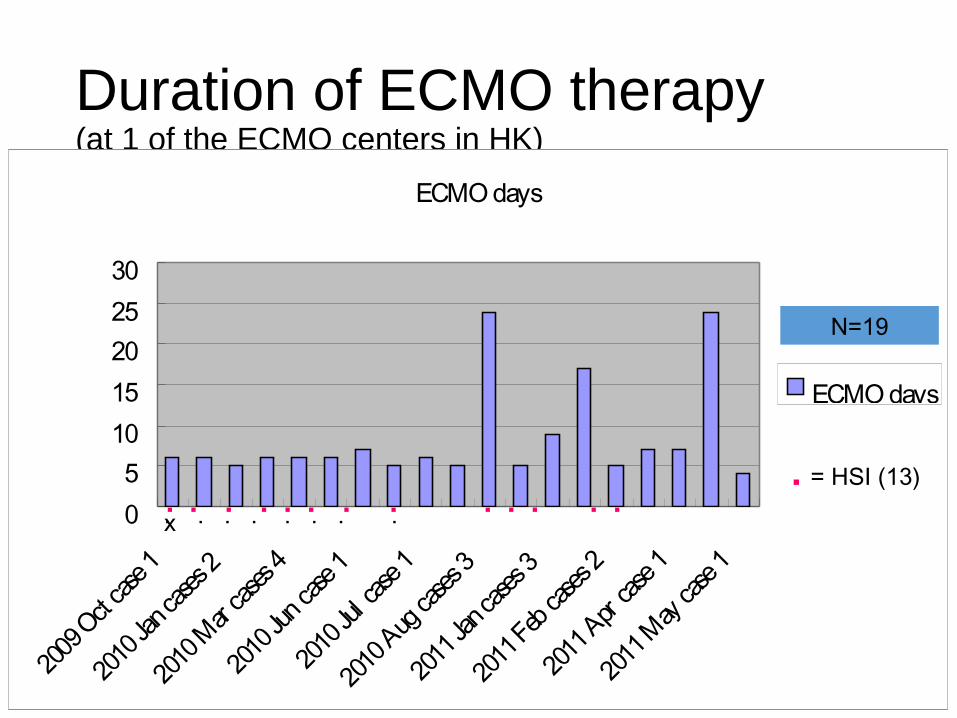
Duration of ECMO therapy (at 1 of the ECMO centers in HK)
ECMO days
05
1015202530
2009 O
ct case
1
2010 J
an cas
es 2
2010 M
ar case
s 4
2010 J
un cas
e 1
2010 J
ul cas
e 1
2010 A
ug cas
es 3
2011 J
an cas
es 3
2011 F
eb cas
es 2
2011 A
pr cas
e 1
2011 M
ay cas
e 1
ECMO days
. . . . . . . . . . . . . . . . . . . . .x
. = HSI (13)
N=19
Echo before ECMOExclude contraindications -Aortic dissection / atherosclerosis
Exclude new reversible pathology - Tamponade- Valve disease - LV dysfunction
Specific nursing careSpecific nursing care
Monitor patientMonitor patient’’s conditions condition
• PPatientatient’’s s vital signs, vital signs, SaO2SaO2• ABG: pH, ABG: pH, pCO2, pO2 pCO2, pO2 • Extracorporeal blood flow Extracorporeal blood flow • ECMO circuit inspectionECMO circuit inspection• Observe for potential complicationsObserve for potential complications especially especially
bleeding bleeding • Plasma free Hb (Haemolysis)Plasma free Hb (Haemolysis)• Body temperatureBody temperature

Observe patient’s parameter
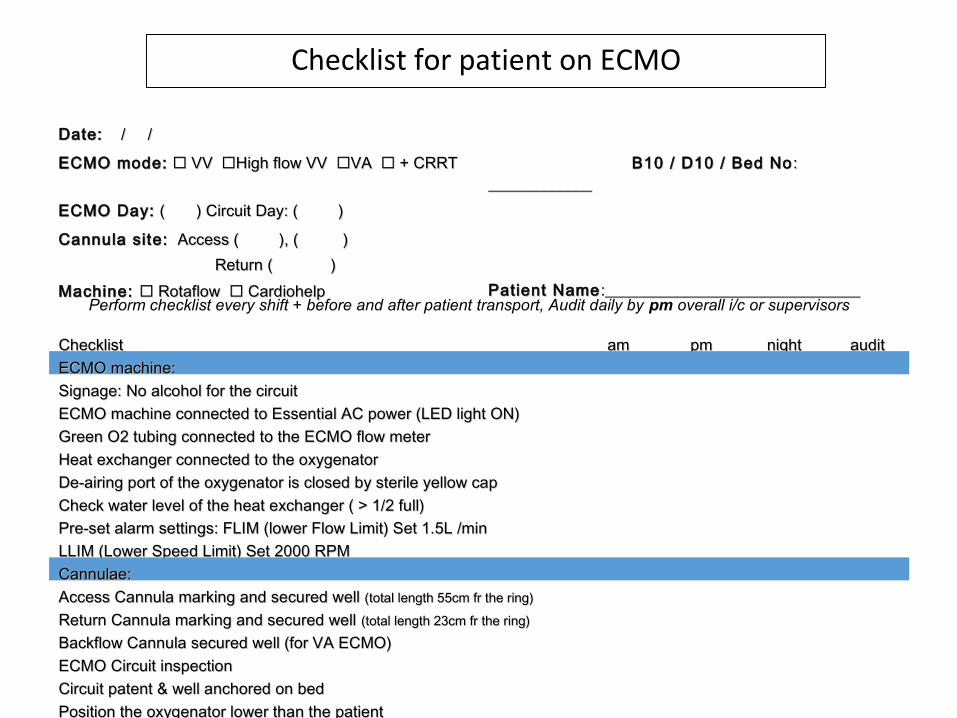
ChecklistChecklist amam pmpm nightnight auditauditECMO machine:ECMO machine: Signage: No alcohol for the circuitSignage: No alcohol for the circuit ECMO machine connected to Essential AC power (LED light ON)ECMO machine connected to Essential AC power (LED light ON) Green O2 tubing connected to the ECMO flow meterGreen O2 tubing connected to the ECMO flow meter Heat exchanger connected to the oxygenatorHeat exchanger connected to the oxygenator De-airing port of the oxygenator is closed by sterile yellow capDe-airing port of the oxygenator is closed by sterile yellow cap Check water level of the heat exchanger ( > 1/2 full)Check water level of the heat exchanger ( > 1/2 full) Pre-set alarm settings: FLIM (lower Flow Limit) Set 1.5L /minPre-set alarm settings: FLIM (lower Flow Limit) Set 1.5L /min LLIM (Lower Speed Limit) Set 2000 RPMLLIM (Lower Speed Limit) Set 2000 RPMCannulae:Cannulae:Access Cannula marking and secured well Access Cannula marking and secured well (total length 55cm fr the ring)(total length 55cm fr the ring) Return Cannula marking and secured well Return Cannula marking and secured well (total length 23cm fr the ring)(total length 23cm fr the ring) Backflow Cannula secured well (for VA ECMO)Backflow Cannula secured well (for VA ECMO) ECMO Circuit inspectionECMO Circuit inspection Circuit patent & well anchored on bedCircuit patent & well anchored on bed Position the oxygenator lower than the patientPosition the oxygenator lower than the patient
Checklist for patient on ECMO
Date:Date: / / / /
ECMO mode:ECMO mode: VV VV High flow VV High flow VV VA VA + CRRT + CRRT B10 / D10 / Bed NoB10 / D10 / Bed No : : __________________________
ECMO Day:ECMO Day: ( ) Circuit Day: ( ) ( ) Circuit Day: ( )
Cannula site:Cannula site: Access ( ), ( ) Access ( ), ( ) Return ( )Return ( )
Patient NamePatient Name :________________________________:________________________________ Machine: Machine: Rotaflow Rotaflow Cardiohelp Cardiohelp Perform checklist every shift + before and after patient transport, Audit daily by pm overall i/c or supervisors

Air/O2 blender
Centrifugal pump
Warmer
Oxygenator
System console
Access cannulaAccess cannula
Return cannulaReturn cannula
ECMO related parts & equipment

Cardiohelp ECMO oxygenator
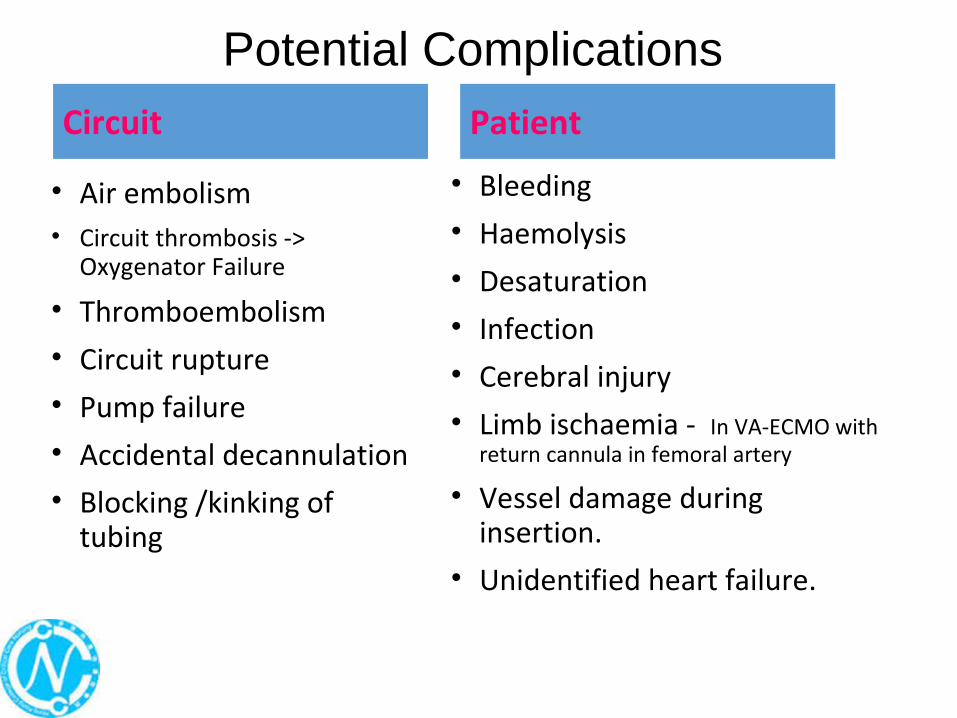
Potential Complications
• Air embolism• Circuit thrombosis ->
Oxygenator Failure
• Thromboembolism
• Circuit rupture
• Pump failure
• Accidental decannulation
• Blocking /kinking of tubing
• Bleeding
• Haemolysis
• Desaturation
• Infection
• Cerebral injury
• Limb ischaemia - In VA-ECMO with return cannula in femoral artery
• Vessel damage during insertion.
• Unidentified heart failure.
Circuit Patient

Elevate the bed in whole piece to avoid kinking of cannulae
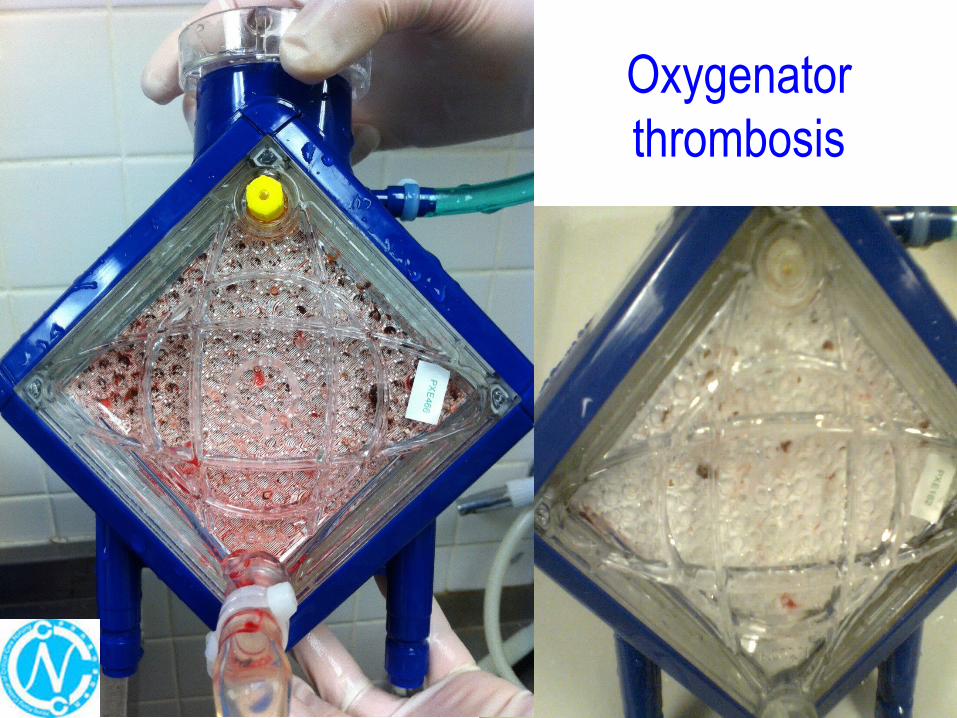
Oxygenatorthrombosis
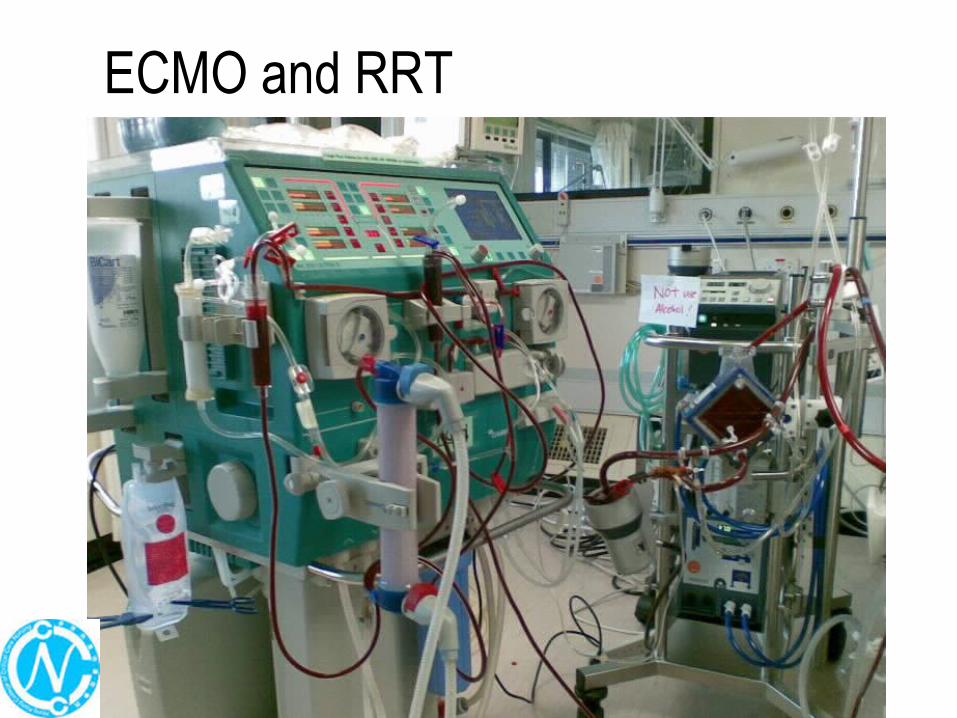
ECMO and RRT
Monitor effect and side effect of concurrent treatment• Titrate sedation according to the sedation target• Monitor clotting profile (APTT) adjust heparin infusion
accordingly
• the ventilator should be adjusted to a low setting to allow lung rest• Continue protocol for DVT prophylaxis (use sequential
mechanical compression device)
• Maintain nutrition (enteral feeding preferred).
44
ECLS Programs
44

4545
4646
An early day ECMO training hosted by Pamela Youde Nethersole Eastern Hospital (PYNEH)

4747
The first comprehensive course in VV ECMO jointly organized by Pamela Youde Nethersole Eastern Hospital and Hong Kong College of Critical Care Nursing

4848
Local ECMO Training Programs Organized by Queen Mary Hospital

4949
The first International ECMO Course
conducted in Hong Kong

5050
Picture taken in an International training program “ECMO simulation train the trainer course”
in Delaware USA in early October 2014

51
Retrieval service in ECLS program
51

Preparation • To obtain information on: - patient’s condition, - body weight, and - existing vascular access and type
• Involve the referring hospital on: - equipment preparation (Checklist), and - consent from relatives to be obtained.
Cannulation• Clear role assignment with doctors, nurses and auxiliary staff• Cannulation and stabilization before patient transfer• Patient should be escorted back to ECMO center asap for
further management
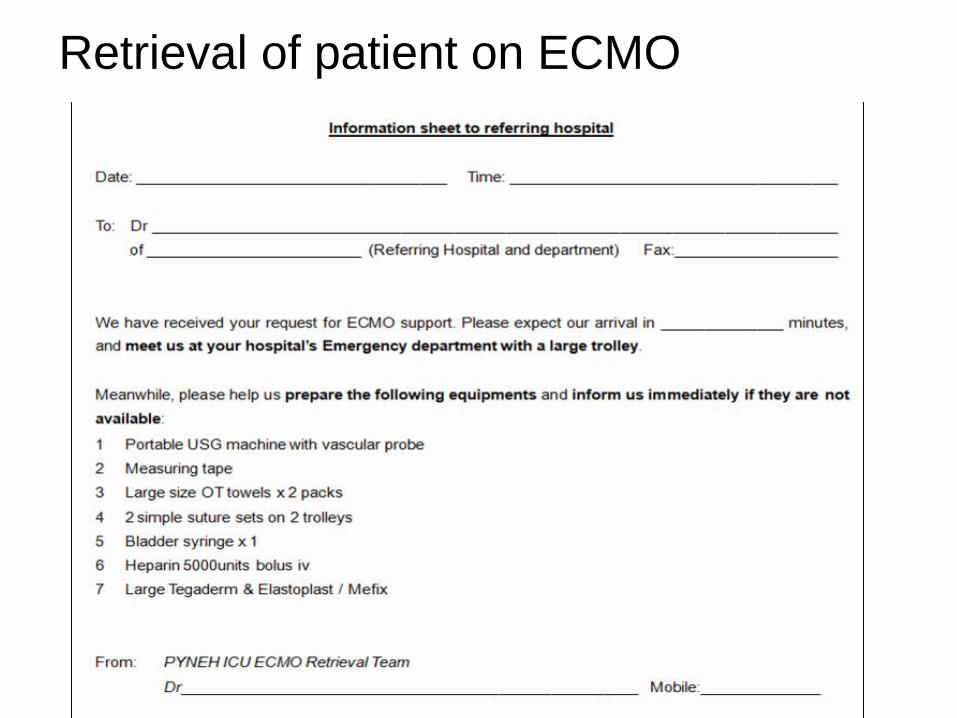
Retrieval of patient on ECMO
Patient escort
• Patients’ haemodynamics including: arterial line BP, ECG, SpO2 , pulse, and blood colour in
and out of the ECMO machine should be continuously monitored during transfer
• Escort personnel should be very skillful and avoid any unexpected hazards during transportation:
e.g. profound hypotension; oxygen hose dislodgement; or accidental decannulation.
55
Advanced nursing practice- ANP in ECLS service
55

56
ELSO guidelines for ECMO Centres on ECMO Specialist
• ECMO specialist should have a strong intensive care background
• ECMO specialist can be a doctor, a nurse or a perfusionist
• There should be an ECMO specialist to provide specialist: patient ratio of 1:1 to 1:2 care throughout the course of ECMO
56

57
Requirements of an advanced practice nurse (APN) in ECLS program• Requires a unique skill set• Strong foundation of ICU nursing• Function independently and as a member of the team• Excellent time management and organisational skills• Problem solving• Ability to make rapid critical decisions• Excellent communications skills
57

58
Credentialing for the advanced practice
• Recommended components in an ECLS course:• Didactic lecture (24-36 Hrs)• Wet-labs/ Water drills (hands-on workshop)• Simulation-based training
• Supervised practice (Bedside 16-32 Hrs)• Completion of competency assessment• In addition, the specialist should have adequate
volume of practice hour per year (request at least 8 hours in 8 weeks), otherwise, retraining is required
58
59
Roles of an APN in ECLS program1. The primary role is to ensure safety
2. Provide direct care to patient on ECMO:• Commence ECMO (including patient retrieval)• Stabilize patient on ECMO• Patient care planning throughout patient journey• Manage ECMO circuit• Handle clinical emergencies
3. Be proactive, and able to anticipate and recognize early ECMO-related complications, and provide prompt actions to them is mandatory!
4. Advanced practice nurse in ECLS program also serves as patient advocate:• Link between medical team and family • Support family during crisis moments• Looking out for patient’s and family’s wellbeing
59

60
Roles of an APN in ECLS program
5. Other roles:• Organize ECLS training program• Perform audit on ECLS program• Conduct ECLS researches• Support ECLS development in local and international level.
Work is hard but rewarding!
60

61
The Way Forward
NOW - 3 Types of ECMO
61
Respiratory ECMO
• Cardiac ECMO• “Rescue” ECMO
6262
The Way Forward for ECMO in Hong Kong
• With increasing ECMO experience and the potential improved outcomes, some experts have begun to suggest early implementation of ECMO as a lung-protective strategy.
• As ventilator-induced lung injury (VILI) continues to be recognized
as an important element of morbidity and mortality of patients with acute respiratory failure, early initiation of ECMO represents an intriguing option to potentially improve outcomes and protect the lungs of these critically ill patients
Respiratory ECMO

6363
The Way Forward for ECMO in Hong Kong
Keeping patient awake and mobilized during ECMO to improve their quality of life
ECMO as a bridge to lung recovery or lung transplantation
6464
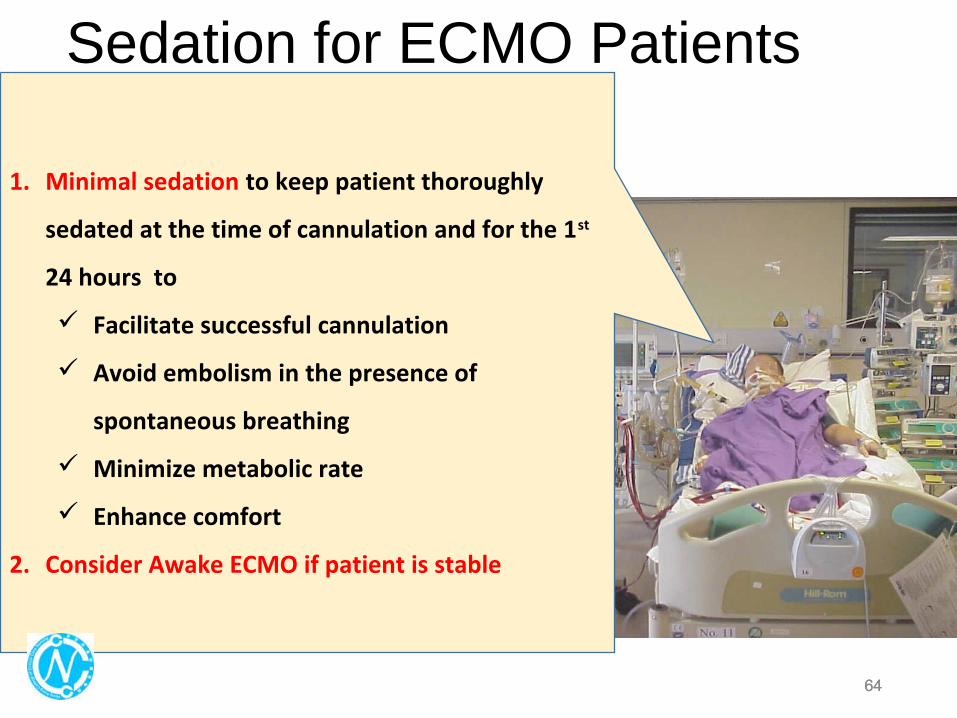
Sedation for ECMO Patients
1. Minimal sedation to keep patient thoroughly
sedated at the time of cannulation and for the 1st
24 hours to
Facilitate successful cannulation
Avoid embolism in the presence of
spontaneous breathing
Minimize metabolic rate
Enhance comfort
2. Consider Awake ECMO if patient is stable
6565
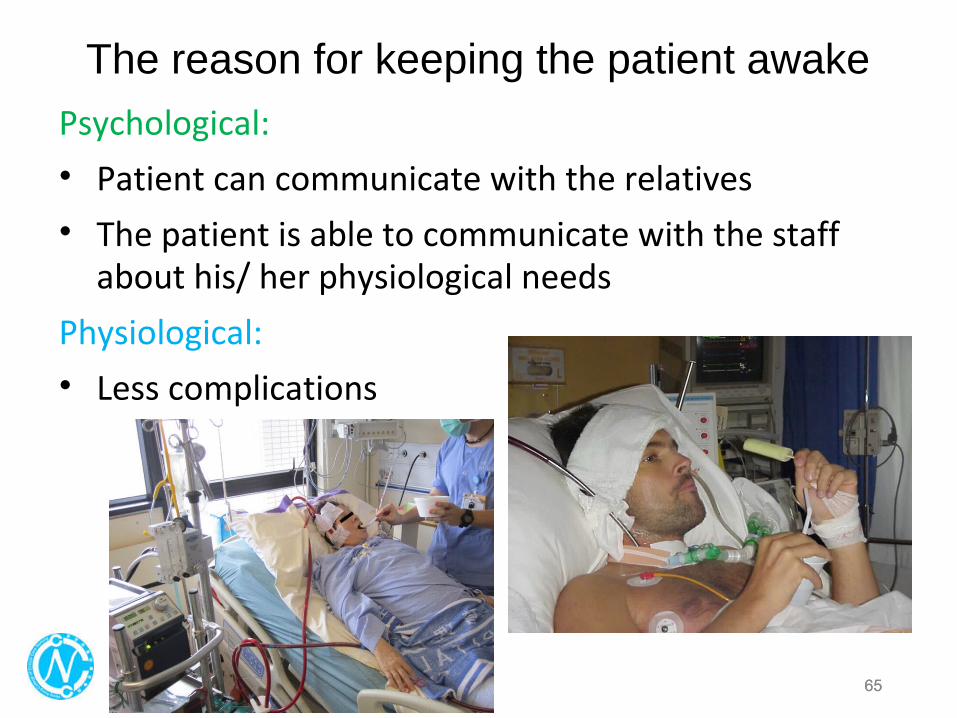
The reason for keeping the patient awake
Psychological:
• Patient can communicate with the relatives
• The patient is able to communicate with the staff about his/ her physiological needs
Physiological:
• Less complications

6666
Prone Position
• Multicenter, prospective RCT in patients with ARDS• 237 patients (prone) versus 229 patients (supine)• Outcome: early application of prolonged prone- position
significantly mortality at 28-day (p<0.001) and 90-day (p< 0.001)
• This results in practice change with more pronation therapy before ECMO and some even practice pronation therapy during ECMO

6767
Another trend in the hemodynamic market is the use of small, lightweight ECMO systems when high levels of support are needed in extremely sick or high-risk patients.
The Way Forward for ECMO in Hong Kong
Increasing the trend on having more VA-ECMO or mix type of VV & VA-ECMOprovided biventricular support for respiratory and cardiac failure (e.g. cardiomyopathy/ myocarditis)
Cardiac ECMO

68
“Rescue” ECMO
68
• Increased utilization for ECPR• ECMO to CPR can increase survival rates to 40 percent
• Can you go on ECMO without a heartbeat? – YES!• ECPR: better than conventional CPR• “ECMO - the resuscitating technique of the future”!
Said Robert Barlett, the “Father of ECMO”
Food for thought:• Having additional position of ECMO Specialist• Establish rapid response ECMO Algorithm (e.g.<30
minutes) for E-CPR.• Unify Guidelines and protocols to facilitate ECMO
Service.• More research on the topic.

7070
Acknowledgement:NC & APN of the 5 ECMO Centres in Hong Kong