Embed Size (px)
Citation preview
Co-Prescribing Opioids and Benzodiazepines: Risks and
RecommendationsPresenters:
• Hooshang Shanehsaz, RPh, Director of Pharmacy, Cardinal Health, and Vice President, Delaware Board of Pharmacy
• R. Corey Waller, MD, MS, Medical Director, Center for Integrative Medicine, Spectrum Health Medical Group
Clinical Track
Moderator: Kelly J. Clark, MD, MBA, FASAM, DFAPA, President-elect, American Society of Addiction Medicine, and Member, Rx and Heroin Summit National Advisory Board
Disclosures
Hooshang Shanehsaz, RPh; R. Corey Waller, MD, MS; and Kelly J. Clark, MD, MBA, FASAM, DFAPA, have disclosed no relevant, real, or apparent personal or professional financial relationships with proprietary entities that produce healthcare goods and services.
Disclosures
• All planners/managers hereby state that they or their spouse/life partner do not have any financial relationships or relationships to products or devices with any commercial interest related to the content of this activity of any amount during the past 12 months.
• The following planners/managers have the following to disclose:– John J. Dreyzehner, MD, MPH, FACOEM – Ownership interest:
Starfish Health (spouse)– Robert DuPont – Employment: Bensinger, DuPont &
Associates-Prescription Drug Research Center
Learning Objectives1. Describe the risks associated with co-prescribing opioids and
benzodiazepines.2. Explain how PDMPs can be used to detect patients who are at
high risk to receive both prescriptions and identify troublesome prescribing patterns.
3. Identify strategies for prescribers to reduce the harmful effects of co-prescribing opioids and benzodiazepines.
4. Identify strategies for prescribers to decrease and/or eliminate utilization of benzodiazepines in high-risk populations.
5. Provide accurate and appropriate counsel as part of the treatment team.
March 30th, 2016Hooshang Shanehsaz, RPh
Co-Prescribing Opioids and Benzodiazepines: Risks and Recommendations
Delaware’s Prescription Drug Monitoring Program
Presenter Information Hooshang Shanehsaz, RPhDirector of Pharmacy, Cardinal Health, Vice President, Delaware Board of PharmacyPrescription Drug Action Committee, Chair, Control Committeehas disclosed no relevant, real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services.”
Original paper written by: Iman Parhami, MD, MPH; Jonathan (Kevin) Massey, BS; Imran Trimzi, MD; Kevin Huckshorn, PhD; Gerard Gallucci, MD, MHS
Learning Objectives:
1. Describe the risks associated with co-prescribing opioids and benzodiazepines.
2. Explain how PDMPs can be used to detect patients who are at high risk to receive both prescriptions and identify troublesome prescribing patterns.

Case Study
• 37-YOF, recently divorced and well-educated, presents to her primary care physician with complaints of daily panic attacks and anxiety.
• History of anxiety problems with panic attacks since her teens.• The daily episodes are unpredictable, elapsing for 15 minutes, and comprising of palpitations,
sweats, shakes, shortness of breaths, and chest pain.• Her medical history is negative other than chronic back pain that started after a work accident and
receives Rx for oxycodone 5mg (every six hours as needed) from her worker’s compensation provider.
• Her medical workup is unremarkable. • She is diagnosed with an anxiety disorder and given a psychiatric referral.• Her PCP provides a prescription of alprazolam 0.5mg (take one tablet every eight hours as needed
for anxiety, dispense 90). Less than two weeks later, the patient is found unarousable in bed. • The medical examiner determined that she died due to an accidental overdose of benzodiazepines
and opioids. Blood revealed high concentrations of alprazolam, oxycodone, alcohol in her blood.
Prescription Opioids and Benzodiazepines Misuse FACTS
Centers for Disease Control and Prevention (CDC) report:1. More than 80 prescriptions per 100 persons in the United States are dispensed
for opioids.2. And 35 prescriptions per 100 people are dispensed for benzodiazepines.(2)3. In addition, many patients are prescribed medications from both classes
together, increasing the risk or adverse events such as respiratory depression and death.
4. Of the 22,767 deaths relating to prescription drug overdose in 2013, 16,235 (71.3%) involved opioid painkillers, and 6,973 (30.6%) involved benzodiazepines.1
5. People who died of drug overdoses often had a combination of benzodiazepines and opioid painkillers in their bodies.1
Prescription Opioids and Benzodiazepines Misuse FACTS
1. Out of one million patients with an opioid prescription, over one-third filled opioid prescriptions by two providers, 14 percent from three providers, and 11 percent from four or more providers.3
2. Nearly two million Americans, aged 12 or older, either abused or were dependent on opioid painkillers in 2013.4
3. Prescription opioid misuse rates have increased in the last few years totaling 4.6 percent nationally per year in the United States. 5,6
4. Approximately 2.1 million people in the United States abused prescription opioid pain relievers in 2012. 7

Prescription Opioids and Benzodiazepines Misuse
Benzodiazepine misuse is also increasing. 8,9 According to a 2010 Substance Abuse and Mental Health Services Administration (SAMHSA) report, 186,000 new individuals misused benzodiazepines in 2010, and the number seeking treatment tripled in the last decade. 10,9,11.

Potential Complications of Opioid and Benzodiazepine Use
1. The most serious complication of benzodiazepine and opioid misuse involves respiratory depression and death.
2. Effects are greater taken together than if taken individually.10
3. According to the CDC, opioid pain relievers were involved in about 17,000 overdose deaths in 2011, and about one-third of these overdose deaths involved benzodiazepines as a contributing cause. 2
4. Higher risks for addiction-related repercussions, intravenous heroin use, blood-born viral infections such as HIV and Hepatitis C, and criminal activity.
5. Strong tolerance and withdrawal properties, individuals filling these prescriptions may seek illegal drugs (sometimes cheaper) such as heroin, to self-medicate their withdrawal symptoms. 10
Prescription Drug Monitoring Program1. PDMP collect, monitor, and analyze electronically transmitted prescribing and dispensing
data.2. Submitted by pharmacies and dispensing physicians including ER.
3. It helps physicians and pharmacies identify potential lethal interactions and abuses.
4. Each state’s laws and rules govern their PDMP.
5. In August 2012, Delaware’s PDMP was launched. It records information on schedule II-V prescriptions that are dispensed in Delaware. Information includes the drug dosage and dispensed quantity, patient age, sex, payor, prescriber and the dispenser.
Opioid and Benzodiazepine Use In Delaware
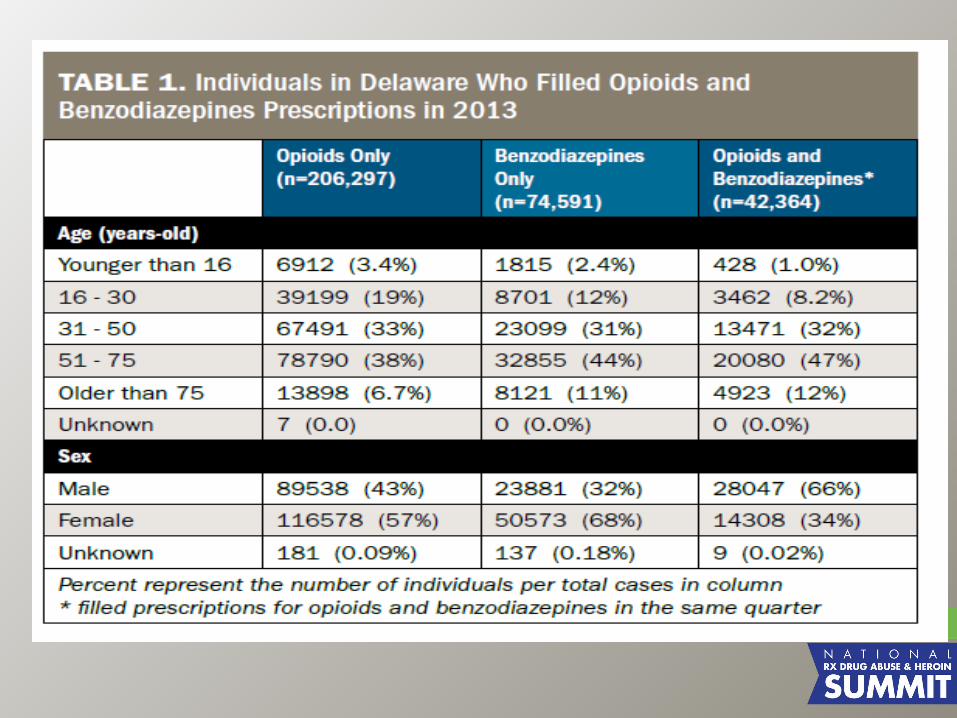
• Based on Delaware’s PDMP, 347,930 individuals filled prescriptions for controlled substances in 2013.
• Approximately 12 percent (n=42,364) filled prescriptions for benzodiazepines and opioids in the same calendar quarter.
• Most of those who filled prescriptions for both opioids and benzodiazepines were aged between 51-75 years old (47 percent), and more than two third were male.
According to a 2012 CDC report, prescribing rates of opioids and benzodiazepines were higher than average in Delaware compared to other states:
• 90.8 opioid prescriptions per 100 persons (ranked 17th highest in the US)
• 21.7 prescriptions per 100 persons for long-acting/ extended-release opioid pain relievers (ranked 2nd highest)
• 8.8 per 100 persons for high-dose opioid pain relievers (ranked highest); and 41.5 prescriptions per 100 persons for benzodiazepines.2
Opioid and Benzodiazepine Use In Delaware

Potential Benefits From Delaware ’s Prescription Drug Monitoring Program
Delaware’s PDMP can have multiple clinical and public health benefits.• First, prescribers can access the data in real-time and obtain reports of a
patient’s prior prescriptions to determine whether patients are receiving benzodiazepines or opioids from other prescribers.
• Second, pharmacies can detect conflicting prescriptions from multiple providers.
• Third, health care organizations can determine whether certain physicians commonly prescribe these two classes of medications together.
• Fourth, researchers can use the data to understand whether certain medications or certain patient demographics correlate with an increased risk of filling prescriptions for both benzodiazepines and opioids. This data can influence and evaluate new programs aimed at reducing misuse and poor prescribing patterns.
Detecting and Managing Pill Misuse
Regular assessments for misuse, urine toxicology screens, and PDMP reviews may help curb pill misuse. The World Health Organization (WHO) has developed a brief, reliable, and valid screening instrument used to detect hazardous and harmful drug use in the primary care setting. 12 This screener, WHO-ASSIST (Alcohol, Smoking, and Substance Involvement Screening Test) is freely available online (http://whqlibdoc.who.int/ publications/2010/9789241599382_eng. pdf?ua=1).
ConclusionThe potential effects of opioid and benzodiazepine misuse are detrimental. Unfortunately, a significant part of this problem arises from physician prescriptions. Prescribers can help reduce the harmful effects by being more mindful of potential misuse, utilizing the PDMP, and providing brief addiction related treatments or referrals. In addition, the PDMP is a valuable tool that can help better detect patients who are at high risk to receive both prescriptions, and prescribers who are more likely to exhibit troublesome patterns.
Importantly, the scope of this report is limited to prescription opioid and benzodiazepine misuse and fails to mention the interaction with alcohol and these medications. In 2010 alcohol was involved in 18.5 percent of opioid pain relievers and 27.2 percent of benzodiazepine drug-abuse related emergency department visits and 22 percent of opioid pain relievers and 21 percent of benzodiazepine related deaths in 13 states. 13 Alcohol combined with opioids or benzodiazepines increases the risk for more serious emergency department visits. 14 Therefore, it is important to assess alcohol use when prescribing opioids and benzodiazepines.
References:1.Centers for Disease Control and Prevention. National Vital Statistics System mortality data. (2015) Available from URL: http://www.cdc.gov/nchs/deaths.htm.2. Paulozzi LJ, Hockenberry JM. Vital signs: Variation among states in prescribing of opioid pain relievers and benzodiazepines, 2012. Available at: www.cdc.gov/ mmwr/preview/mmwrhtml/mm6326a2.htm. Accessed Dec 17 2014.3. Jena AB, Goldman D, Weaver L, Karaca-Mandic P. Opioid prescribing by multiple providers in Medicare: Retrospective observational study of insurance claims. BMJ. 2014;348:g13934. Substance Abuse and Mental Health Services Administration, Results from the 2012 National Survey on Drug Use and Health: Summary of National Findings, NSDUH Series H-46, HHS Publication No. (SMA) 13-4795. Rockville, MD: Substance Abuse and Mental Health Services Administration, 2013.5. Jones CM. Frequency of prescription pain reliever nonmedical use: 2002-2003 and 2009-2010. Arch Intern Med. 2012;172:1265-1267.6. SAMSA. State estimates of nonmedical use of prescription pain relievers. The NSDUH Report: State Estimates of Nonmedical Use of Prescription Pain Relievers. Published Jan 8 2013. Available at: archive.samhsa.gov/data/2k12/NSDUH115/sr115-nonmedical-use-pain-relievers.htm. Accessed Dec 15 2014.7. SAMSA. Results from the 2012 National Survey on Drug Use and Health: Summary of national findings. Center for Behavioral Health Statistics and Quality. Available at: archive.samhsa.gov/data/NSDUH/2012summnatfinddettables/National findings/nsduhresults2012.htm. Accessed Dec 17 2014.8. Lader M. Benzodiazepines revisited—will we ever learn? Addiction.2011;106:2086-2109.9. Pradel V, Delga C, Rouby F, et al. Assessment of abuse potential of benzodiazepines from a prescription database using ‘doctor shopping’ as an indicator. CNS drugs. 2010;24:611-620.10. Jones JD, Mogali S, Comer SD. Polydrug abuse: A review of opioid and benzodiazepine combination use. Drug Alcohol Depend. 2012;125:8-18.11. SAMSA. Results from the 2009 national survey on drug use and health. Office of Applied Studies, NSDUH Series H-38A, HHS Publication No. SMA.10-4586. Rockville, MD.12. WHO-ASSIST Working Group. The alcohol, smoking and substance involvement screening test (ASSIST): development, reliability and feasibility. Addiction. 2002;97:1183-1194.
References:
13. Jones CM, Paulozzi LJ, Mack KA. Alcohol involvement in opioid pain reliever andbenzodiazepine drug abuse-related emergency department visits and drug related death – US, 2010. Centers for Disease Control and Prevention. Available at: http://www.cdc.gov/MMWr/preview/mmwrhtml/mm6340a1.htm. Published Oct 10 2014. Accessed Dec 20 201414. SAMSA. Benzodiazepines in Combination with Opioid Pain Relievers or Alcohol: Greater Risk of More Serious ED Visit Outcomes. Available at:www.samhsa.gov/data/sites/default/files/DAW N-SR192-BenzoCombos-2014/ DAW N-SR192-BenzoCombos-2014.pdf. Accessed Dec 22 2014.
THANK YOU
Benzodiazepines
R. Corey Waller MD, MS, FACEP, DFASAMPresident, Michigan Society of Addiction MedicineMedical Staff Chief, Pain MedicineSUD Medical Director, PIHP Region 3

Abuse Stats
• The number of benzodiazepine admissions nearly tripled between 1998 and 2008, while overall treatment admissions increased only 11 percent
• The majority of benzodiazepine admissions were male, between the ages of 18 and 34, or non-Hispanic White
• Almost all benzodiazepine admissions (95 percent) reported abuse of another substance in addition to abuse of benzodiazepines: – 82.1 percent reported primary abuse of another
substance with secondary abuse of benzodiazepines, and
– 12.9 percent reported primary abuse of benzodiazepines with secondary abuse of another substance
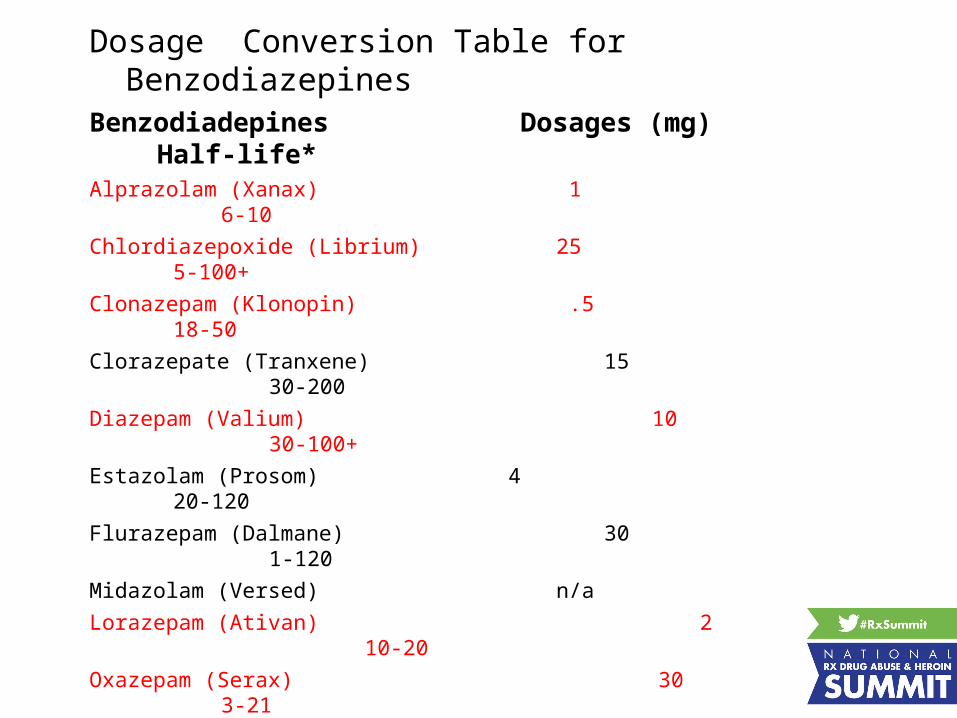
Dosage Conversion Table for Benzodiazepines
Benzodiadepines Dosages (mg) Half-life*
Alprazolam (Xanax) 1 6-10
Chlordiazepoxide (Librium) 25 5-100+
Clonazepam (Klonopin) .5 18-50
Clorazepate (Tranxene) 15 30-200
Diazepam (Valium) 10 30-100+
Estazolam (Prosom) 4 20-120
Flurazepam (Dalmane) 30 1-120
Midazolam (Versed) n/a Lorazepam (Ativan) 2
10-20 Oxazepam (Serax) 30
3-21Quazepam (Doral) 30
20-120Temazepam (Restoril) 30
10-12Triazolam (Halcion) 1
2-3Zolpidem (Ambien) 20
2.5Zaleplon (Sonata) 20
1Adapted from Giannini AJ. Drugs of abuse. 2d ed. Los Angeles: Practice Management
Information Corp., 1997:121-5.*Includes metabolites - in hours
Benzos: Patterns of Use
• 45% of Use <30 days• 80% of Use <4 months• 15% of Use >12 months (7-18% Europe)
• Women, twice the rate as men• <40% of Anxiety Diagnosis Treated with Benzo• >40% of Panic Disorder Treated with Benzo
BZD: Adverse Effects
• BZD vs other psychotropics have few SE • Sedation, CNS Depression– Worse if combined with EtOH or opioids
• Behavioral Disinhibition– Irritability, excitement, aggression (<1%), rage
• Psychomotor & Cognitive Impairment– coordination, attention (driving)– poor visual-spatial ability (not aware of it)– Ataxia, confusion
BZD: Adverse Effects
• Overdose: Rare fatalities if BZD alone• Severe CNS & Respiratory Depression if
combined with:– alcohol– barbiturates– narcotics– tricyclic antidepressants
Tolerance• Time-dependent decrease in effect.• Neurochemical basis unclear
• Varying rates for different behavioral effects:• sedative and psychomotor effects • diminish first (e.g. few weeks)
• memory and anxiety effects persist despite chronic use.
• Varying rates with different benzos.• If no history of addiction, rarely see dose
escalation or overuse• Cross-tolerance with ETOH and other sed-hyp
Dependence• Negative reinforcement of withdrawal - major deterrent to
discontinuing use.• Difficult to distinguish between WD & rebound anxiety upon
discontinuing drug.• Withdrawal-time-limited (not part of original anxiety state)• Relapse-reemergence of original anxiety• Rebound - increased anxiety > baseline
• Also see insomnia, fatigue, • headache, • muscle twitching, tremor, • sweating, dizziness, • tinnitus, difficulty concentrating, • nausea, depression, • abnormal perception of movement, • irritability
Dependence/Withdrawal, cont.
• Rarely -seizures, delirium, confusion, psychosis.
• triggering of depression, mania, OCD.
• 90% of long-term users (>8mo-1yr) experience significant withdrawal
• insignificant wd if used less than 2 weeks• mild-moderate if used >8 weeks
• Slow taper (>30days) with +/- carbamazepine, valproic acid, trazodone, imipramine.
• CBT effective in dc-ing benzos and controlling panic/anxiety.
Predictors of severe withdrawal
• High-potency-quickly eliminated• (e.g. alprazolam, lorazepam, triazolam)
• higher daily dose• more rapid rate of taper (esp last 50%)• diagnosis of panic disorder (not GAD)• high pre-taper levels of anxiety and depression• ETOH or other substance dependence/abuse• personality pathology -e.g. neurotic or dependent• Not motivated to discontinue use

Practical Points regarding Benzodiazepines.
• Lowest effective dose for the shortest possible time.– Minimizes dependence and withdrawal.
• Discontinuance withdrawal is most common with short-acting benzodiazepines.– Cessation of long-acting drugs produces a tapering effect due to long
elimination half-life.– Patients on short-acting benzodiazepines need weeks to months to be
weaned.– Do this at 20% per month– You can flip to longer acting BDZ and wean from there
Behavioral Health
• Focused on reason for starting BDZ• Mindfulness• CBT• Watch for increase in MJ or Tobacco• Slow and steady through the stages of change
Co-Prescribing Opioids and Benzodiazepines: Risks and
RecommendationsPresenters:
• Hooshang Shanehsaz, RPh, Director of Pharmacy, Cardinal Health, and Vice President, Delaware Board of Pharmacy
• R. Corey Waller, MD, MS, Medical Director, Center for Integrative Medicine, Spectrum Health Medical Group
Clinical Track
Moderator: Kelly J. Clark, MD, MBA, FASAM, DFAPA, President-elect, American Society of Addiction Medicine, and Member, Rx and Heroin Summit National Advisory Board