Embed Size (px)
Citation preview

Mini-Scleral Design - MSD
• Large RGP• Vaults the cornea, rests on the
sclera.• Creates a fluid filled environment.• Can be used to treat any corneal
condition.• Can be used to treat other anterior
segment conditions.

MSD - Advantages
• Very Stable lens.
• Fluid filled environment.
• Improved comfort.
• Good visual acuity.

Mini-Scleral Design

MSD – Fitting Pearls
Central Feather-
touch.
Intra-limbal
adjustment.
With or without
fenestration or
fenestrations.
Watch edge for
tightening.

Practice Management Issues
• Setting Fees.• Bill for services performed.• Insurances and fee collection.• Appropriate diagnostic and
treatment equipment.– Topography/corneal mapping.– Pachymetry.– Fitting sets.

Refractive Surgery Specific
Moderate – Large Diameter(10.5 mm Standard Diameter, 9.5 mm
to 12.0 mm). Reverse Geometry Transition.
Post Surgical Central BC. Curves
• Paracentral Fitting Curves.
• Asymmetric Corneal Technology (ACT).

A New Option for Keratoconus
Keratoconus Intacs -1 Day PKP -1 Week

Contact Lens Intolerant Keratoconus Steep K ‘s, 45 to 60 Changing refractions, eyes irritated, frequent visits/re-
fits Lenses not providing functional vision
Outright failure Shortened wearing time Inability to achieve 20/40
“keratoconus personality” exacerbated Apprehensive about transplant
Active, younger or risk averse
Objective - Bridge the gap between frustration and (PKP) “the point of no
return”

Reshape the Cornea for CL Success

History
Adjustable Ring
1984

INTACS Design Features• Precision manufactured
to ± 0.01mm: •150° arcs PMMA
•Unique hexagonal cross-section design with 7mm wide optical zone
•Positioning holes for manipulation
• Inserts placement:• In peripheral cornea
•Between stromal layers
Stromal LamellaeStromal Lamellae
6.9 mm
8.1 mm

Stromal LamellaeStromal Lamellae
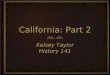
How INTACS Work…
Inserts placed at 75% corneal depth
Inserts separate corneal lamellae
Separation shortens corneal arc length
Central cornea flattens
Increased flattening achieved with thicker segments

Watch the Pre-op and Post-op mire INTACS Normalize Corneal Shape
The INTACS Procedure
Courtesy David Schanzlin, MD Shiley Eye Inst. UCSD

INTACS – PKP ComparisonINTACS – PKP Comparison
+8.00 (.)-2.00 X 180°-0.75
TransplantIntacs

INTACS - PKP ComparisonPKP
Irreversible Procedure Time: 1 Hour Rehab Time: 12-18
Months
Intraocular Procedure Lifetime Follow-up
required Complications
• Cataract• Glaucoma• Endophthalmitis• Rejection• Expulsive hemorrhage• Corneal ulcer• Neovascularization• Induced astigmatism• Disease recurrence• Risk of viral transference
INTACS
Reversible Out-Patient Procedure
Time: 20-30 Minutes Rehab Time: 1-2 Weeks
(Visual Function Immediate) Corneal Lamellar Procedure Periodic Follow-up Complications
• Unsatisfactory ring placement• Segment extrusion(All easily managed with segment removal)

INTACS - PKP Comparison
PKP
Significant loss of endothelial cells
Permanently weakened cornea with risk of additional trauma
Outcomes: unpredictable, often unstable
INTACS
Endothelial cell loss, not clinically significant1
Provides structural integrity, PKP still an option without complication
Outcomes: predictable, case dependent
1Two-Year Endothelial Cell Assessment following INTACS implantation, Azar et al, J Refract Surg. 2001 Sept-Oct

3 lenses for most of the situations
The most common cones : nipple and ovale

Lenses have to follow as close as possible this very prolate cornea in order to :
– respect the cornea– Stabilize properly– Be comfortable
Need to have « very » steep lenses in the center that get flatter « quickly ».

Good center and periphery

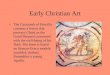
Rose K PrincipleLens changes with the cone
evolution • When a keratoconus is getting more and
more advanced, the apex of the cone is getting steeper but the periphery remains the same.
• For a known apex of the cone, the periphery is often the « same » fom one patient to another : Paul Rose’s Statistic and mathematic models : correlation between BC and slope

Rose K lenses principle
• For each BC that respects the apex of the cone, an unique AEL will be associated to it– Unique Optic Zone– Unique Peripheral curves
World sales indicate that the original AELrepresent 65% of sold lenses

For a 8.70mm diam.

Axial Ege Lift (AEL) Edge Lift (EL)
• Rather than talking about AEL in mm which is difficult to evaluate for the fitter, Paul Rose simplified and reduced this notion to a simple number without unit : Edge Lift (EL)• EL = 0 = standard corresponds to the AEL
associated to the curve• EL > 0 correspond to lenses that are flatter in
periphery than standard• EL < 0 correspond to lenses that are steeper in
periphery than standard

available EL+3.00 à -1.3 / 0.1
•EL Standard “0” 65%
•EL “quick” +1.0 20%
•EL “slow” -0.5 10%
•Others 5 to 10%
The majority of Rose K are done with 3 EL

Trial Box
• Std EL for all lenses (but AEL unique for each BC)
• Powers increase in steep curves : the more advanced is the cone, the more myopia there is important for assessing precisely centration and mobility .
• Diameter decreases when the cone is getting advanced (difficult for large lenses to follow the very flat periphery)


Fitting steps
1. Keratometry from a keratometer or a topograph
7,00 mm 12⁰
6,60 mm 102⁰
Km. 6.80
Cyl. 3,00

2. In the trial box, choose the lens according to the rule :BC = av.K -0.10
3. Assess the contact at the apex of the cone• If too much contact (Flat) decrease BC• If not enough contact (Steep) increase BC
STEEP FLATOPTIMALE

Remarques
• Wait 1 minute before evaluation
• Analyze fluo pattern, lens centered

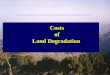
4. After finding the best BC– If too thin periphery (< 0.6 mm) EL
« quick » +1.0– If too wide periphery (> 0.8mm) EL
« slow » -0.5Too thin Optimal Too wide

5. Centration and mobility
Up riding.steep the lens.and/or reduce diameter .and/or reduce EL
Low riding.Flatten the lens.and/or increase diameter .and/or increase ELOptimal

6. Find the best sphere giving the best

Spherical Aberrations
• Peripheral rays are more refracted than central rays.
Ex : -7.00 in the center, -7.75 in periphery

• Those aberrations induced by the lens are higher when : – Pupil is large– Power of the lens is high
More benefits for high myopic patients

Rose K2 Advantages
• Easy to fit– Only 1 trial box : one lens name– Lens changes with the cone (AEL changes with BC)– Std EL works in main cases– 2 other EL slow and quick cover most of the
modifications– 6 steps fitting
• Maximum physiological respect– Material Z– Special Geometry for the best compromise
physiology/vision
• Vision– Control of the spherical aberrations


Indications
• Pellucid Marginal Degeneration - PMD• Keratoglobus• Post lasik ectasy, Post Graft
PMDDMP Globus Lasik

• reversed design for BC > 7.20• flatter the BC is, more reversed the design is• Larger optical zone • OZ decreases with BC• EL steeper than Rose K•Total diameter larger than graft diameter• Also used on post lasik ectasy


5 Edge Lift
+0.6 /+1.2 / -0.5 / -1.0

1st lens: BC = K’ +0.30 mm
Fitting: 1. Keratometry 2. BC
3. central Fitting 4. peripheral fitting 5. Centration/Mobility (=>Diameter)
6.Power
Ex. 6.80/5.50 5.50 +0.30 = 5.80

BC
plat
OK / serré
serré

EL
périphérie très serrée EL Lent (-)
périphérie serrée EL standard
Périphérie ok EL rapide (+)

Mobility
Look for enough mobility to insure enough tear flow
Mobility ++ Mobility --
increase diameter Decrease diameter decrease BC Flatten BC0
decrease l’Edge Lift increase l’Edge Lift

1st lens = Km - 0.30 mm
Fitting : 1. Keratometry 2. BC 3. central fitting 4. peropheral fitting 5. Centration / mobility
6. Power
Ex. 6.80/5.50 6.15 - 0.30 = 5.85

ROSE K2 Post Graft: Rose K2 PG
• the hardest fitting• irregular cornea shape• High astigmatism, often irregular sensitives eyes

• Optimal