Prosthetic valve obstruction Prosthetic valve thrombosis Bileaflet mechanical prosthetic valve Cinefluoroscopy Prosthetic valve leaflet motion
- 1. Echo Egypt 2014 Thursday, October 23, 2014
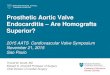
2. Does it have a place in theechocardiography era? 3. Types of
Prosthetic Heart Valves Mechanical Bileaflet (St Jude)(A) Single
tilting disc (Medtronic Hall)(B) Caged-ball (Starr-Edwards) (C)
Biologic StentedCF Leaflet imaging depends on radio-opacity Porcine
xenograft (MedtronicMosaic) (D) Pericardial xenograft
(Carpentier-Edwards Magna) (E) Stentless Porcine xenograft
(MedronicFreestyle) (F) Pericardial xenograft Homograft (
allograft) Percutaneous Expanded over a balloon(Edwards Sapien) (G)
Self expandable(CoreValve) (H) Circulation 2009, 119:1034-1048 4.
Three Types of MechanicalProsthetic Heart ValvesNewer models Older
modelsnBileaflet (St Jude) Single tilting disc (Medtronic Hall)
Caged-ball (Starr-Edwards)Preferred Choice 5. Despite the
recentimprovements in prostheticvalve design and
surgicalprocedures,valve replacement doesnot provide a
definitivecure to the patient;instead it gives rise todevelopment
of a newdiseaseprosthetic valve disease.Native Valve Diseaseis
traded forProsthetic Valve Disease 6. Prosthetic valves
explantedfor severe dysfunction.Pibarot P , and Dumesnil J G
Circulation. 2009;119:1034-1048Outlet strut Inlet
strutLeafletCopyright American Heart Association, Inc. All rights
reserved.ObstructivethrombosisPannusingrowthinteracting withleaflet
openingRupture of theoutlet strutand leafletescape 7. Imaging of
Prosthetic Heart valvesChest X-ray ( CXR )Valve type and position
often easily determined on CXRCinefluoroscopy ( CF )CF optimal for
assessing mechanical valve leafletmotion(radiopaque), unable to see
bioprosthetic leafletsEchocardiography TTE will often best allow
optimal Doppler angles TEE( 2D/RT3D )will often best allow optimal
directvisualizationMulti Detector Computed Tomography ( MDCT
)Allows full evaluation with less artifacts from metalcompositions
as compared to echo. 8. The location of thecardiac valves is
bestdetermined on thelateral radiograph. A line is drawn on
thelateral radiograph fromthe carina to thecardiac apex. The
pulmonic andaortic valves generallysit above this line andthe
tricuspid and mitralvalves sit below this line.Sometimes the aortic
rootcan be inferiorly displacedwhich will shift the aorticvalve
below this line.Chest X-rayAoV & PVMV & TV 9. Chest
X-rayaortic valvemitral valveBjork Shiley valve 10. Bileaflet
Mechanical Prosthetic Heart ValveHingeLeaflets( Occluder
)HousingNormal motion ,Restricted motionSuture RingWell seated
,DehiscedRole of Cine-FluoroscopyIdentify type of valveDetermine
disc mobilityAssess stability of sewing ring 11. Bileaflet
Mechanical Prosthetic Heart ValvesEach model has its own
cinefluoroscopicfeatures which allow its identification 12.
Cinefluoroscopy as the gold standard formechanical valve mobility
13. *Evaluation is considered appropriate when theprosthesis
tilting disk optimal projection isobtained.*This view allows proper
visualization of leafletmotion so that both opening angle (OA)
andclosing angle (CA) can be calculated.C-arm fluoroscopeThe en
faceprojectionThe tilting diskprojectionSide ( Pivot )view 14.
Cinefluoroscopy : Obtaining optimal viewRight anterior
oblique,cranialMitral prosthesisRight anterior oblique,caudalLeft
anterior oblique,cranialAortic prosthesisAortic prosthesisTricuspid
prosthesis 15. Bileaflet Mechanical Prosthetic Heart ValvesThe
opening angle (0), closing angle (C), Theexcursion of each leaflet
(E l, E 2), and the totalleaflet excursion (E total)Opening and
closingangles are defined asthe distance betweenthe 2 leaflets in
the fullyopen and closedposition. 16. Normal values for opening and
closing anglesClosingangle (CA)( cinefluoroscopy )Openingangle
(OA)Bileaflet MechanicalProsthetic Heart ValvesCarbomedics
130Edwards Duromedics 148Sorin Bicarbon 135St.Jude Medical Standard
120Values of OA and CA is obtained by averaging the values over 3
or 5consecutive cardiac cycles, in the presence of sinus rhythm or
atrialfibrillation, respectively.Normal reference values for OA and
CA is obtained from the manufacturer 17. Fluoroscopy of a normally
functioning CarboMedics bileaflet prosthesis in mitral
position.Montorsi P et al. Circulation.
2003;108:II-79-II-84Copyright American Heart Association, Inc. All
rights reserved.Opening angleClosing angle 18. Fluoroscopic
criteria :*Persistent restriction of leaflet(s) motion*Opening
angle greater than the normalreference value(obtained from the
manufacturer)Opening angleNormal Obstruction 19. Example of a
patient with obstructionof a St. Jude prosthetic aortic valve (size
19)Doppler shows aorticprostheticregurgitation & highpressure
gradients70At fluoroscopy, openingangle (OA)reached 70,indicative
of severelyhypomobile leaflets. 20. Stuck Mechanical Tricuspid
Valve ProsthesisThe Valve That Does Not MoveFluoroscopy. A,
Systolic and (B) diastolic frames indicate that both discs ofthe
mechanical tricuspid valve (TV) are stuck in an open position.The
mechanical mitral valve (MV) discs are closed in systole.Fadel B M
et al. Circulation. 2012;126:e335-e336Copyright American Heart
Association, Inc. All rights reserved. 21. St. Jude prosthetic
valve ( mitral ): One of the leaflets was stuck in theclosed
position (Video 1).Normal movement of the valve after streptokinase
(Video 2)N Engl JMed2009;360:e22April
16,2009DOI:10.1056/NEJMicm040909 22. Obstruction by pannus
,thrombus ,or bothCine-FluoroscopyCannot distinguishpannus vs
thrombus 23. T T ET E EC FMDCTImaging modalities 24. That is
theQuestion
inProstheticValveThrombosisThrombolysisorOperationThrombolytic
therapy significantly reduces themean pressure gradient and
improves valve leafletopening angle, so CF can detect the response
to TT 25. Cinefluoroscopy showing leaflet motionBefore thrombolytic
therapy After thrombolytic therapyThe views of the open valveThe
views of the closed valveOne leaflet is seen to be
immobilized(arrow). The measured opening angleis 59(normal, 111),
and the closingangle is 110 (normal, 1202).Leaflet motion is seen
to havereturned almost entirely to normal.The opening angle is now
14 andthe closing angle 124.5911014124 26. If lytic infusion is
stopped at this time,the remaining thrombus could be the triggerCF
: Guide duration for a late rethrombotic process.of lytic therapyAn
abnormal OA value(greater than the normal)OA improvedbut
notnormalizedOA completelynormalizedMontorsi P et al.
Circulation.2003;108:II-79-II-84 Normal Doppler study
despitesignificant restriction in leaflet(s) motion at CF(so called
Doppler silent PVT). 27. Tricuspid mechanical prosthesisCF showing
both of theleaflets fixed in a semiopenpositionAfter 25 mg tPA
infusion, CFrevealed mild movement ofboth leafletsAfter heparin
Infusion&a second TTsession with 25 mg tPA, restriction
ofleaflets was completely resolvedTrk Kardiyol Dern Ar - Arch Turk
Soc Cardiol 2014;42(5):478-481doi: 10.5543/tkda.2014.09804 28. On
admission, CF of tricuspidmechanical prosthesis showingbileaflets
fixed in a semiopenposition (A)Minor alteration in leaflet
positionsduring systole and diastoleafter 25 mg tPA infusion
wasadministered (B)After 50 mg tPA infusion, restriction ofleaflets
had completely resolved (C).Trk Kardiyol Dern Ar - Arch Turk Soc
Cardiol2014;42(5):478-481 doi: 10.5543/tkda.2014.09804 29.
Prosthetic Valve ThrombosisCLASS IIa : Fluoroscopy or CT is
reasonable in patientswith suspected valve thrombosis to assess
valve motion.(Level of Evidence: C)*Fluoroscopy and CT are
alternative imaging techniques for evaluation ofmechanical valve
leaflet motion, particularly in patients with prostheticaortic
valves, which are difficult to image by either TTE or TEE.*CT is
best suited for measurement of valve opening angles.*CT imaging may
also allow visualization of pannus or thrombus in patientswith
mechanical or bioprosthetic valves. 30. Pseudo prosthetic
valveobstructionProsthetic valve gradientsIt is an important lesson
to learn ,raised prosthetic gradient is notequal to thrombusPlease
remember flow acrossprosthetic valve is governedby delicate local
hemodynamicrules 31. The Am J Cardiol. 2000. Jan 1. Vol
85CinefluoroscopyDopplerechocardiographyTransesophagealechocardiographyNormal
opening angles High gradientsAbsence ofthrombus and pannus 32.
L'HUILLIER I et al. Heart 2001;85:513Bileaflet prosthesis( Only one
leaflet at the mitral position )Acute mitral valve
dysfunctionCopyright BMJ Publishing Group Ltd & British
Cardiovascular Society. All rights reserved. 33. Ultrasound shows
the escaped leaflet(arrows) as a linear hyperechogenicobject in the
lumen of terminal portionof the abdominal aorta.The surgically
removedmechanical valve 34. Dehiscedaortic valve(Rocking
)Normalmitral valveMitral and aortic valves (Medtronic Hall and ATS
Medical, respectively 35. A Few Words AboutMulti Detector
ComputedTomography 36. St. Jude medical valves (bileaflet
mechanical valves)The geometric orifice area ( GOA), length,
andopening/closing angles determined by MDCT. 37. St. Jude
bileaflet prosthetic AVRA, obstructive acute thrombusvisualized as
low-attenuation mass.Chan J et al. Circulation.
2009;120:1933-1934B, After thrombolysis with resolutionof
thrombus.Copyright American Heart Association, Inc. All rights
reserved. 38. AppropriateUseScore (19)Prosthetic Heart
Valves*Characterization of prosthetic cardiac valves A
(8)*Suspected clinically significant valvulardysfunction*Inadequate
images from other noninvasivemethodsScore 7 to 9 ( A ) Appropriate
IndicationsAppropriate test for specific indication (test is
generally acceptable andis a reasonable approach for the
indication). 39. Fluoroscopy is the most widely used
methodfordiagnosing stuck valves.It is readily available inmost
centers and can be performed rapidly,particularlyin unstable
patients. 40. Fluoroscopy is not usefulin distinguishing pannus
fromthrombus since neitherpannus nor thrombus can beidentified
fluoroscopically.In the case of bileaflet valves, the diskscan be
directly visualized, and opening andclosing angles can be measured
using aside (pivot) view.pannusThrombus10 OA 120 CAMoreover,
fluoroscopy may be particularlyutilized as an easily repeatable
modality tofollow stable patients for evaluation ofvalve motions
during TT. ThrombolyticTherapy 41. One should consider that
bothechocardiography and CF providedifferent kinds of information
onprosthesis function, and thereforethey should still be considered
ascomplementary and not alternative.