Embed Size (px)
Citation preview
2
ARF Immunologically mediated inflammatory
responseDelayed sequel to GABH Strept. throat
infectionGenetically susceptible individuals
Developed world - dramatic decline in incidence
Developing world – still a major problem – 20 million new cases/year
Introduction
3
ARF - Aetiopathogenesis Definite aetiology ??
Antigenic mimicry between streptococcal M-protein epitopes & human tissues (heart valves, myosin, synovium & basal ganglia)
Autoimmunity in genetically susceptible individualsConstant association with HLA class II antigens (HLA
B5)
Age – 5 -18 yrs Incidence:
Developed world - 0.05/1000 populationDeveloping world - 24/ 1000 population
4
Making the diagnosis of streptococcal pharyngitis
Streptococcal pharyngitis (Group A beta-hemolytic pharyngitis)Only 10-15% incidence in adults with
pharyngitisBut a 40% incidence in children with
pharyngitis
5
Making the diagnosis of streptococcal pharyngitis
Scoring system for risk of strep pharyngitis:1. Temperature > 37.8 degrees C2. Tonsillar exudate3. Anterior cervical lymphadenopathy
Three factors present = 40-50% risk of strep pharyngitis
Only two factors present = 15% risk Consider increased risk for known exposure or
community outbreak
6
Making the diagnosis of streptococcal pharyngitis
Clinical diagnosisFever and sore throat are always presentRarely seen are rhinitis, conjunctivitis,
bronchitis, laryngitis or diarrheaMust have pharyngeal edema or exudateMust have cervical lymphadenopathy
7
Diagnosis of ARF
No “gold standard”No specific clinical/lab. test to establish
diagnosisDiagnosis based on revised (updated)
Jones criteria1944 T. Duckett JonesFinal revision 1992 – by committee on
Rheumatic Fever, Endocarditis, Kawasaki Disease of the AHA
8
Updated Jones Criteria: (need 2 major or 1 major and 2 minor criteria AND
evidence of infection):
Major manifestations Carditis Erythema marginatum Polyarthritis Subcutaneous nodules Chorea
Minor manifestations Clinical findings: arthalgia and fever Lab findings: ↑ESR, ↑C-reactive protein, ↑acute-phase
reactants, prolonged PR interval Supporting evidence of antecedent streptococcal infection
Positive throat culture or rapid streptococcal antigen test Elevated or rising streptococcal antibody titers
Exception : Chorea Indolent carditis
9
10
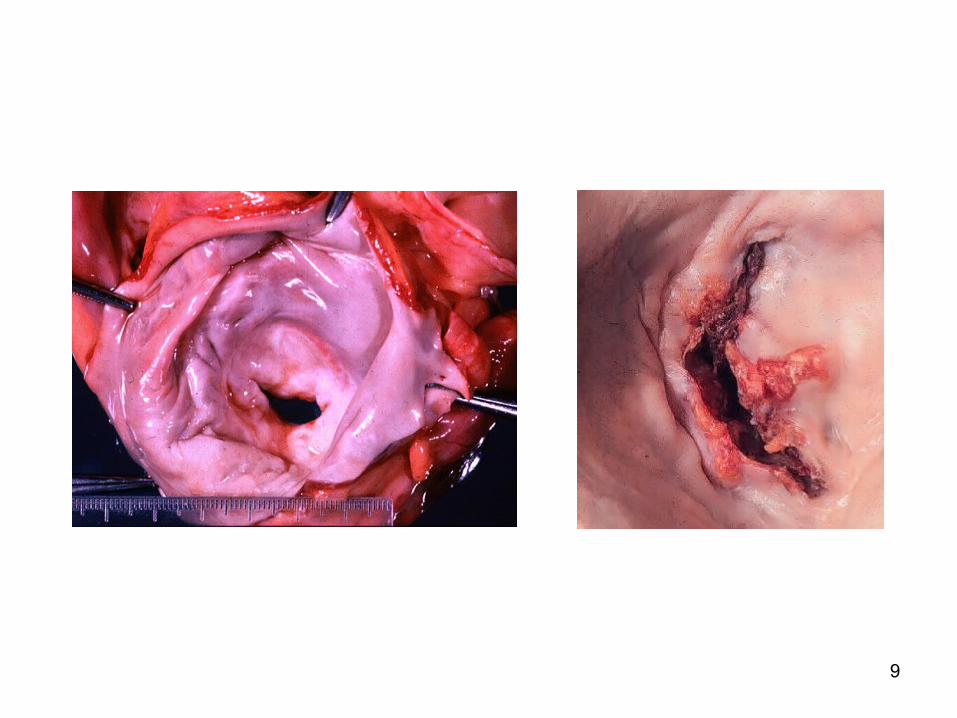
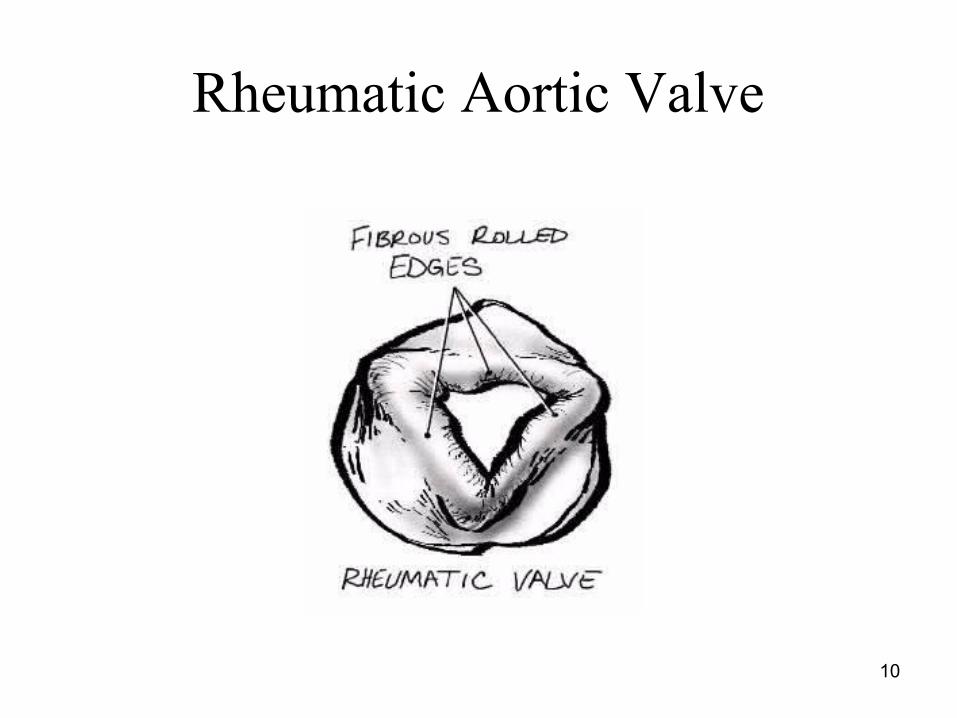
Rheumatic Aortic Valve
11
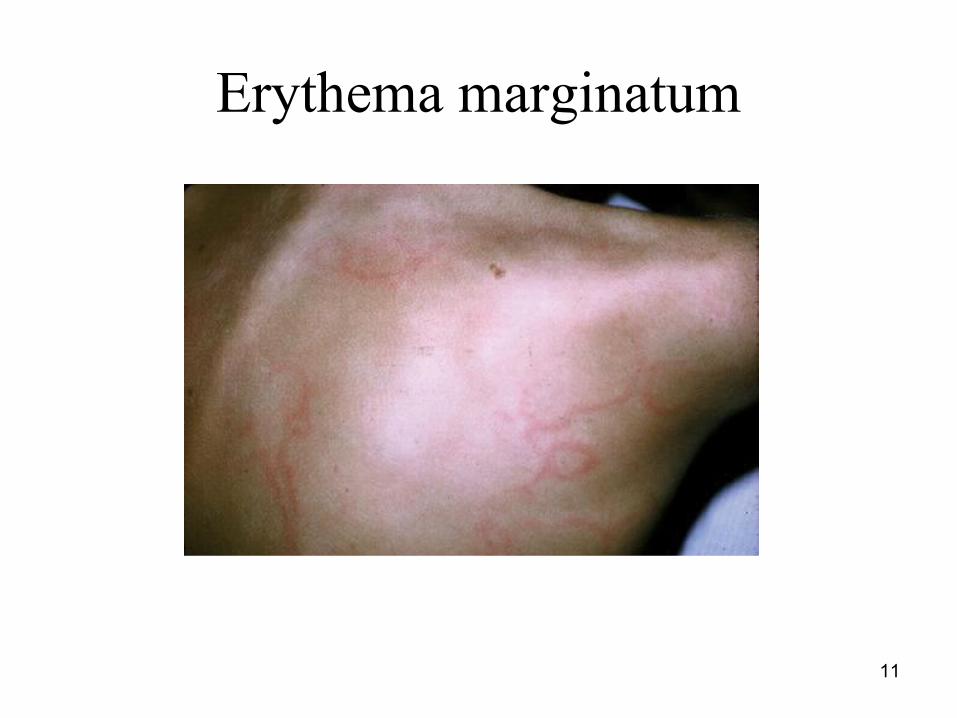
Erythema marginatum

12
13
Clinical findings in ARFCarditis
may have an insidious or subclinical onset: 40-50% incidence with first attack of ARF More common in younger children Decreased risk with increasing degree of polyarthritis Is frequently a pancarditis, may be asymptomatic. Usually appears in the first 3 weeks of an ARF attack. Suggested by presence of :
Pericarditis, cardiomegaly, CHF, new heart murmur(s) Less specific findings:
ECG changes: PR interval (>0.04), P wave contour change, inverted T waves
Resting tachycardia – even during sleep Arrythmias
14
CarditisOnset of new heart murmur(s):
Mitral regurgitation/insufficiency – high pitched blowing holosystolic apical murmur, grade 2 or higher that radiates to axilla
Aortic regurgitation – high pitched decrescendo murmur at aortic area
Mitral stenosis and aortic stenosis are classic findings of chronic rheumatic heart disease.
25% go on to develop mitral stenosis 40% will develop mitral insufficiency
15
Polyarthritis Classically is a migratory polyarthritis:
Affects large joints sequentially (knees, elbows, ankles and wrists usually) with multiple joints involved at the same time.
Diagnosis based on joint pain along with heat, swelling, redness and tenderness.
May have arthralgias –-- pain without associated findings.
Adolescent children are more likely to have only one arthritic joint
50% have 6 or more joints involved (↑arthritis = ↓carditis).
Usually lasts < 4 weeks without residual damage
16
Erythema Marginatum
The rash specific for ARF. 10% incidence
Described as a macular or raised erythematous rash in rings or crescent shapes with clear centers.
Nonpruritic and nonpainful
Lesions come and go in minutes to hours.May occur intermittently for weeks to months
Primarily seen on trunk and proximal extremities.
17
Subcutaneous Nodules
10% incidence in ARFMore likely to be present with carditis
Are only present for days to a couple of weeks
May be recurrent however
Description:Firm, painless, < 2cm nodules found over bony
prominences or tendonsCommon on elbows, knees, wrists, ankles and Achilles
tendonUsually one to a few dozen nodules
Indistinguishable from rheumatoid nodulesThere is no treatment
18
Sydenham’s Chorea
Involuntary movements of the hands, face and feet:
5-15% incidenceMay also involve muscular weakness and emotional
lability
Often there is a long latent period between antecedent streptococcal pharyngitis and the onset of chorea.Movements are suppressible with sedationFemales affected more often than males
Attacks often last for several months
19
Laboratory Findings
No definitive tests 1. If there is no recent documented
streptococcal pharyngitis, then you need to check a rapid streptococcal antigen test following by throat culture if antigen test negative
2. Acute phase reactants : ESR, CRP, 3. Serum titer of antistreptococcal antibodies
(ASO)80% will have a positive titer within 2 mths of ARF
onset
20
TreatmentPrevention of initial attack of RF (primary
prevention) eradication of streptococci
Anti inflammatory treatment aspirin, steroids
Prevention of recurrence (secondary prevention)antibiotic prophylaxis
21
Treatment of ARF with Medications:
1. Antibiotics – Benzathine penicillin G (aka bicillin LA) 1.2 million units IM for positive throat culture to prevent spread of ARF-causing streptococcal strain.
Alternatives:Alternatives: Penicillin V 250mg BID po for 10days Erythromycin 250mg QID x 10day for penicillin
allergic patients
22
Treatment of ARF with Medications:
2. Salicylates – for fever and joint pain/swelling
100mg/kg/d of aspirin for childrenShould see prompt response in joints
Treat arthralgias with analgesics NSAIDs ok for aspirin allergic/intolerant but not
studied.
23
Treatment of ARF with Medications:
3. Corticosteroids – use when salicylates fail and whenever carditis is present.
No proof of cardiac damage prevention.2mg/kg mg oral prednisone
2-3 week course with taper for arthritis and fever.
Up to 6 week course with 2 week taper for carditis.
Continue aspirin for one month after stopping steroid
24
Treatment of Carditis/Heart Failure
All carditis patients receive corticosteroids.
Strict bed rest for at least 4 weeksConventional therapies are used to treat
specific symptoms such as heart failure.
25
Treatment of Sydenham’s Chorea
Mainstay of treatment is:Quiet environment (symptoms disappear
during sleep and are are less frequent with less environmental stimulation).
Sedation:BenzodiazepinesHaloperidol for more severe cases
26
Prevention of ARF recurrences:
High risk for ARF recurrence with repeat episodes of streptococcal pharyngitis.Recurrences ↓with ↑age and with the number
of years since last attackRecurrences are more common in those with
a history of ARF carditis and in children.Children have a 20% risk of recurrence
in 1st five years.
27
Prevention of ARF recurrences
Need continuous antibiotic prophylaxis for at least 5 years or until patient at least into their early 20sPrimary recommendation:
Benzathine penicillin G (Bicillin LA) – IM every 4 weeks
May give every 3 weeks for those at highest risk
Alternative: Sulfadiazine 500mg QD for < 27#, 1000mg QD for > 27#
Erythromycin 250mg BID for PCN allergic
28
Endocarditis Prophylaxis
Patients with residual rheumatic valvular disease also need endocarditis prophylaxis
Use a different antibiotic than that used for ARF recurrence prevention
29
Prognosis
Initial mortality rate is 1-2% Persistent carditis = poorer prognosis
30% mortality within 10 years for children
80% of children affected with ARF live to adulthood
Adults – 2/3 are affected with rheumatic valvular disease after 10 years
30
Questions needing answer…..
Should we treat all sore throat with antibiotics to prevent rheumatic fever ?
What is the best anti inflammatory drug in carditis to prevent RHD?Aspirin? Steroid?
What is the best mode of administration of penicillin in secondary prophylaxis?
Should we use echocardiographic finding as a major/minor criterion in diagnosis of carditis in ARF ?
31
Antibiotics for sore throat ?
Del Mar CB, Glasziou PP, Spinks AB. Antibiotics for sore throat. The Cochrane Database of Systematic Reviews 2010, Issue 2. Art. No.: CD000023Objectives: To assess the benefits of antibiotics in the
management of sore throat Search of the literature from 1945 to 2003 Selection: Trials of antibiotic against control with
either suppurative complications & non-suppurative complications of sore throat
Twenty-six studies
32
Results & Conclusion:
Antibiotics confer relative benefits in the treatment of sore throat. However, the absolute benefits are modest
Protecting sore throat sufferers against suppurative and non-suppurative complications in modern Western society can be achieved only by treating with antibiotics many who will derive no benefit
In emerging economies where rates of acute rheumatic fever are high, the number needed to treat may be much lower
33
Anti-inflammatory treatment for carditis in ARF
Cilliers AM, Manyemba J, Saloojee H. Anti-inflammatory treatment for carditis in acute rheumatic fever. The Cochrane Database of Systematic Reviews 2009, Issue 2. Art. No.: CD003176Objectives: To assess the effects of anti-inflammatory
agents (aspirin, corticosteroids & immunoglobulin) for preventing or reducing further heart valve damage in patients with ARF
Literature search from1966 to 2005Eight RCT
34
Results & Conclusion:
No significant difference in the risk of cardiac disease at one year between the corticosteroid-treated and aspirin-treated groups (relative risk 0.87, 95% confidence interval
0.66 to 1.15) Use of prednisone (relative risk 1.78, 95% CI 0.98 to 3.34) or
intravenous immunoglobulins (relative risk 0.87, 95% CI 0.55 to
1.39) when compared to placebo did not reduce the risk of developing heart valve lesions at one year
CONCLUSION: No benefit in using corticosteroids or intravenous immunoglobulin to reduce the risk of heart valve lesions in patients with ARF
35
Penicillin for secondary prevention of ARF
Manyemba J, Mayosi BM. Penicillin for secondary prevention of rheumatic fever. The Cochrane Database of Systematic Reviews 2000, Issue 3. Art. No.: CD002227Objectives: To assess the effects of penicillin
compared to placebo and the effects of different penicillin regimens and formulations for preventing strept.infection and rheumatic fever recurrence
Nine studies
36
Four trials (n=1098) compared IM with oral penicillin and all showed that IM penicillin reduced RF recurrence and Strept. throat infections compared to oral penicillin
One trial (n= 249) showed 3-weekly IM penicillin inj. reduced strept. throat infections (RR 0.67, 95% CI 0.48 to 0.92) compared to 4-weekly dose
Conclusions: IM penicillin more effective than oral penicillin in
preventing RF recurrence and strept. throat infections Two-weekly or 3-weekly injections appeared to be
more effective than 4-weekly injections
Results & Conclusion:
37
Should Echocardiography used as a criterion in diagnosing rheumatic
carditis? Ferrieri P et al. Proceedings of the Jones Criteria
workshop. AHA scientific statement. Circulation 2002;106:2521-2523Echocardiography should only be used as an
adjunctive technique to confirm clinical findings and to evaluate chamber sizes, ventricular function & valvar morphology
It should not be used as a major/minor criterion for establishing the diagnosis of carditis of ARF in the absence of clinical findings
38























