Embed Size (px)
Citation preview

Residual Renal Function (RRF)Thomas A. Golper, MD, FACP, FASN presiding
Program Schedule• 4:45 to 5:05--- Should volume overloaded dialysis patients
be aggressively ultrafiltered to “dry weight” even if RRF declines?– Thomas Golper
• 5:05 to 5:25--- Residual kidney function is a vital tool to improve outcomes– Bernard Canaud
• 5:25 to 5:45--- How can we preserve RRF on dialysis?– Isaac Teitelbaum
• 5:45 to 6:00 ---Discussion

Should volume overloaded dialysis patients be aggressively ultrafiltered
to “dry weight” even if RRF declines?
Thomas A. Golper, MD, FACP, FASNVanderbilt University Medical Center
Nashville, [email protected]
Potential Conflict of Interest DisclosureConsultant: Baxter Healthcare, Honoraria: Baxter, Fresenius North America, Genzyme

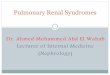
Consequences of Volume Overload
Volume Overload
Hypertension
↑ Pre-Load ↑After-Load
Left Ventricular Hypertrophy and abnormal remodeling Atherosclerosis
Inflammation
Congestive Heart Failure
↑ Cardiovascular Morbidity and Mortality
↓ RRF
Courtesy of Dr Raj Mehrotra

Should volume overloaded dialysis patients be aggressively ultrafiltered
to “dry weight” even if RRF declines?
Thomas A. Golper, MD, FACP, FASNVanderbilt University Medical Center
Nashville, [email protected]
Potential Conflict of Interest DisclosureConsultant: Baxter Healthcare, Honoraria: Baxter, Fresenius North America, Genzyme
No

Hold it right there.Doesn’t excess volume kill?

Hold it right there.Doesn’t excess volume kill?
It sure does.

NT-Pro-Brain Naturetic Peptide Levels Predict Survival in PD
Paniugua et al CJASN 3:407, 2008ADEMEX trial baseline levels prior to randomization; independent of dialysis intensity

NT-Pro-Brain Naturetic Peptide and CV Outcomes in PD Patients
Wang et al, JASN 18: 321, 2007230 prevalent PD patients, followed for 3 years

B-Type Naturetic Peptide In HD PtsKoch et al Clin Nephrol 73:21, 2010
• Background– Plasma levels of hormone released predominantly by
LV myocytes as result of pressure or volume loading (stretch)
– Plasma levels not influenced by renal dysfunction • Tagore et al CJASN 3:1644, 2008
• Prospective Observations 255 Dialysis Patients, stratified by < 340 pg/mL vs. > 340 pg/mL
• Higher BNP at baseline was associated with shortened survival
• The co-morbidity severe CHF over rides BNP• In absence of severe CHF, BNP is predictive

Hold it right there.Doesn’t excess volume kill?
It sure does.But it doesn’t have to.

Trade OffVolume Excess vs. Loss of RRF
• Very few patients have malignant hypertension from mild volume overload
• Very few incident dialysis patients initiate for pulmonary edema or malignant hypertension
• Gentle initiation or incremental dialysis is feasible in most initiates

What we know about RRF

RRF Better Preserved in PD vs. HD• Rottembourg, 1982. 25 pts on each followed for 18
months with GFR going from 4.4 to 4.0 in CAPD and from 4.3 to 1.3 in HD (p < 0.01). Updated in 1993 with more diabetics, same result.
• Cancarini et al, 1986. The PD pts slower decline of RRF but not for all diagnoses.
• Feber, 1994. Children on PD preserve urine output better on PD, but GFR not preserved.
• Park, 2000. PD pts having HD treatments for a month lost GFR faster than PD pts not needing HD (confirmed X 1)

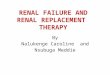
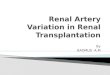
RRF Better Preserved in PD vs. HDLysaght MJ, et al, ASAIO Trans 37:598, 1996
0
1
2
3
4
5
6
0 6 12 18 24 30 36 42 48
Months on dialysis
RR
F C
r C
l (m
L/m
in)
HDPD
N = 57
N = 58The difference persists after adjustment for age,sex, hypertensive status and the use of ACEI

RRF Better Preserved in PD vs. HDMoist et al. JASN 11:556, 2000
*
.
0
0.2
0.4
0.6
0.8
1
PD Univariate Analysis
PD Multivariate Analysts
HD
Adjusted Odds Ratios
p = 0.0001p = 0.001
Wave 2 DMMS of USRDS 811 HD pts and 1032 PD ptsPD pts had a 65% lower risk of losing RRF compared to HD ptsAt each time interval, HD pts were 3X more likely to have lost RRF

30
40
50
60
70
80
90
100
0 6 12 18 24 30 36 42 48 54
CAPD/CCPD
HD
Follow-up months
Prob
abili
ty (%
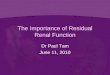
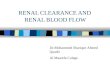
)Patient Survival Probability for Patients Initiating
Dialysis with PD Compared to HD (1990-94)Fenton et al, AJKD 30:334, 1997
Period of
Preserved RRF on PD

30
40
50
60
70
80
90
100
0 6 12 18 24 30 36 42 48 54
CAPD/CCPD
HD
Follow-up months
Prob
abili
ty (%
)Patient Survival Probability for Patients Initiating
Dialysis with PD Compared to HD (1990-94)Fenton et al, AJKD 30:334, 1997
Period of
Preserved RRF on PD
Not controversial as similar findings confirmed in numerous other data sets

Does PD Slow the Rate of RRF Loss?Ramon et al PDI 22:239, 2002
• 14/36 PD pts had Q 1-2 month Cr Cl studies for > 12 months prior to PD and started this period with Cr Cl > 20, then followed on PD for > 6 months
• Mean rate of loss of RRF was less on PD for all pts
• Consistent with at least two rat model studies
p < 0.0005

Why Would This Be?
• Volume overload at initiation portends a poor outcome• Is this a condemnation of predialysis care?
– The damage is already done so the patient’s goose is cooked no matter what happens next
• Is this a condemnation of post dialysis care?– The patient was left volume overloaded
• Is it merely identifying multi-organ failure?

Extracellular VolumePD vs. HD
Plum et al NDT 16:2378, 2001
PD pts are overloaded

Compared To HD PatientsPD Patients……
• Are more frequently in volume excess• Have better early survival• Have better preservation of RRF

Benefits of RRF In Dialysis PatientsDr. Canaud’s talk is next
• Better BP control– Menon et al NDT 16:2207, 2001– Ates et al KI 60:767, 2001
• Higher liklihood of euvolemia– Konings et al NDT 18:797
• Normalization of LVMI– Wang et al KI 62:639, 2002
• Survival– Diaz Buxo et al AJKD 33:523, 1999– Rocco et al KI 58:446, 2000– Bargman et al JASN 12:2158, 2001

The conundrum continues because volume excess is bad for
our patients

PD

Na/Fluid Removal and Mortality in PD PtsEAPOS- Brown et al JASN 14:2948, 2003• Failure to achieve > 750 mL/day of UF in anurics, and• Regardless of RRF, Na and fluid removal predict survivalNECOSAD Jansen et al KI 68:1199, 2005• In anuric PD pts each L/day of UF reduces RR of death by 52%Ates et al., KI 60:767, 2001• 125 incident PD patients, 3-year follow up• Cox multivariate predictors of mortality in addition to hypertension
and comorbidity score:Parameter RR p
– RRF 1 mL/min 0.53 <0.05– Na removal (10 mEq/d) 0.90 <0.001– Total Fluid removal 0.90 <0.01
(100 ml/d)

Increased Peritoneal UF Is Associated With Lower BP
Tonbul et al PDI 23:46-52,2003
• Baseline:– 25 PD patients, Mean time on PD 22.9 mo’s, 13/25 HTN – All patients on same regimen 3 x 1.5% & 1 x 4.25%– Attempt to increase UF with F/U at 1 month– 13/25 had HTN (BP>180/110) and an increase in RX
• Results:– UF increased (1086+259 to 1493+225 mL, p<0.001)– Systolic BP (145+13 vs. 128+5 mmHg) – Diastolic BP (96+10 vs. 81+3 mmHg, p<0.001)– Weight decreased (67.3+8.9 to 65.5+8.7 Kg)– BP meds discontinued in 6/13

Strict Volume Control Normalizes BP, But At What Price?
Gunal et al AJKD 37:588, 2001
• Aggressive dietary approach, followed by UF approach, lowered the body wt 2.8 kg in 47 hypertensive PD pts
• BP 158/96 dropped to 120/78• CTI decreased• In 19 pts with RRF, daily urine volume dropped to
28% of pre-treatment• Kt/V dropped from 2.06 to 1.85 with loss of RRF
What is the perfect balance?

Does Improved Fluid Status Hurt RRF?
Davies et al JASN 14:2338, 2003
• Double blind randomized controlled trial of icodextrin vs. 2.5% dextrose for long dwell
• Icodextrin group lost weight, total body water and salt, dextrose group gained all three (p< 0.05)
• BP control not different• Urine volume better maintained in icodextrin
group– 89 mL/d (p <0.04)

High BP and Survival on PDJust How Bad Is It?
• Jager et al KI 55:1476, 1999– NECOSAD Prospective observational muti-
center cohort study of 118 consecutive incident PD pts
• RR of death of 1.42 for each 10 mmHg BP• Merkus AJKD35:69, 2000
– Post Hoc analysis– 8.6 greater risk if MAP > 107 than if less
• Goldfarb-Rumyantzev et al NDT 20:1693, 2005– Wave 2 DMMS showed that only a very low
BP was associated with high death risk

Hypertension and volume excess in hemodialysis:how aggressive should we be and at what price?
HD

Higher Mortality With Larger Interdialytic Weight Gains
Kalantar-Zedah et al Circulation 119:671,2009
• DaVita data base 2001-2003• 34,000 pts divided into 8 categories of 0.5 kg
increments in interdialytic wt gains, each treatment, each 3 months an average determined
• 1.5 -2.0 kg wt gain = reference• < 1.5 kg gain hazard ratio 0.67• > 4.0 kg gain hazard ratio 1.25• Across all subgroups

Higher Mortality With Larger Interdialytic Weight Gains
Kalantar-Zedah et al Circulation 119:671,2009
• DaVita data base 2001-2003• 34,000 pts divided into 8 categories of 0.5 kg
increments in interdialytic wt gains, each treatment, each 3 months an average determined
• 1.5 -2.0 kg wt gain = reference• < 1.5 kg gain hazard ratio 0.67• > 4.0 kg gain hazard ratio 1.25• Across all subgroups
We presume that volume mediates its mortality effects by hypertension and progressive heart failure

Observational Data Describing BP And Mortality In HD
Luther and GolperKI 73:667, 2008
U or J shaped
Counterintuitive
Reverse epidemiology

Reverse Epidemiology:Risk Factor Paradox In The Chronically Ill
Possible Causes
• Survival bias: – Only a small fraction of CKD pts survive to get to
ESRD– Survival of the most fit!
• Competitive risks have different influences over time– e.g. malnutrition will get you sooner than overnutrition
• Presence of the malnutrition-inflammatory complex reverses the risk factors itself

Relationship Between BP and Mortality Changes Over Time
Stidley et al JASN 17:513, 2006
• DCI database, 17,000 incident HD pts, 1993-2003• Covariates: gender, age, race, cause of ESRD, Kt/V,
albumin, Hct, antihypertensive drug use or not in first 90 days
• Modeled baseline BP (days 31 to 120) and mortality, and then time-varying BP and time-varying covariates
• Median pt f/u was 2.05 yrs, slightly more blacks in DCI set than USRDS, but otherwise similar

Stidley et al JASN 17:513, 2006

Stidley et al JASN 17:513, 2006
Early years

Stidley et al JASN 17:513, 2006
Early years
Later years

Relationship Between BP and Mortality Changes Over Time
Stidley et al JASN 17:513, 2006
• Relationship between baseline BP and mortality changes over time– Low SBP increases mortality in early yrs (<2)– Adverse effects of high SBP are later (>3) and not large
• DBP hazard in HD similar to general population• Ideal BP in HD pts not yet identified• High SBP post HD is more of a predictor for mortality than
is predialysis SBP– Raises issue of intradialytic hypertension

So now maybe we should treat hypertension more aggressively in
HD patients

Achieving BP Targets in HDDavenport et al KI 73:759, 2008
• Audit of BP control using RA GLs of 2002, 11 London Units, over one week, 2600 pts, almost 8000 dialysis sessions
• 36% of pts achieved predialysis BP < 140/90• 42% of pts achieved post dialysis BP < 130/80• 15% of pts had enough symtomatic intradialytic
hypotension to require fluid resuscitation– Failure to achieve dry wt not counted– 7% of all dialysis sessions
• Intradialytic hypotension more prevalent in centers achieving lower post dialysis BP

0
5
10
15
20
25
30
0 10 20 30 40 50 60
% of patients in dialysis centre achieving post dialysis blood pressure target
% p
atie
nts
in d
ialy
sis
cent
re w
ith
intra
dial
ytic
hyp
oten
sion
r = 0.8, p = 0.003
Complications of Aggressive BP Control Davenport et al KI 73:759, 2008

0
5
10
15
20
25
30
0 10 20 30 40 50 60
% of patients in dialysis centre achieving post dialysis blood pressure target
% p
atie
nts
in d
ialy
sis
cent
re w
ith
intra
dial
ytic
hyp
oten
sion
r = 0.8, p = 0.003
More frequent hypotension as a consequence of aggressive targets
Complications of Aggressive BP Control Davenport et al KI 73:759, 2008

Improved Volume Status Is Associated with Improved Nutrition
Cheng et al AJKD 45:891, 2005
• In absence of differences in transport status or RRF incident PD pts followed for 9 months with nutritional studies and bioimpedance
• Those who decreased their ECW – Increased their ICW (new or growing cells)– Had stronger nutritional indices– Decreased CRP
• Those who increased their ECW – Increased their ICW at first, then stopped– Had weaker nutritional indices– Increased CRP
Does ECW excess swell the bowel and lead to inflammation and poor nutrition?

What are we to do then?

Failure To Maintain Volume Homeostasis
Excessive Sodium and Water intake• The initial more liberal sodium and fluid diet for PD
patients, compared to HD patients, should be frequently reassessed, must not be abused, and maybe should be abandoned entirely– Fine et al (JASN 8:1311, 1997) in a double-blinded
study gave 60 mEq/d of extra Na to CAPD pts and BP ONLY rose 9/5 (p < 0.05)
• Clearly, as RRF decreases, patients must be advised to reduce Na and fluid intake.

Van Olden et al PDI 23:339, 2003
Change From Baseline after 2 g/day of Furosemide for 2 days
Urine volume (mL/day) 500Urine Na (mmol/day) by 54GFR (mL/min) no change
Diuretics In PD Patients in the Acute Setting

Chronic Diuretics In CAPD PtsMedcalf et al KI 59:1128, 2001
61 incident CAPD pts randomly assigned to furosemide 250 mg/day or to no diuretic
P < 0.05
Diuretic
Control
Diuretics had no effect
on either urea or creatinine
clearances

High Dose Diuretics
• Gerlag and van Meijel Arch Int Med 148:286, 1988– Refractory CHF , up to 4000 mg/d continuous intravenous
furosemide in 35 patients, those that survived the to discharge on doses changed to 2500 mg/d orally
– No observed tinnitus or ototoxicity, most frequent complication was hypokalemia (31/35)
• Kuchar and O'Rourke Eur Heart J 6: 954, 1985– Refractory CHF,up to 8000 mg/d continuous intravenous
furosemide in 24 patients, maintenance doses up to 3000 mg/d orally
– Transient tinnitus was observed in 1 patient.

High Dose Diuretics• Brown, Ogg, and Cameron Clin Nephrol 15: 90, 1981
– RCT 56 ARF patients on HD or PD to two different regimens of furosemide, (1) furosemide 4 mg/min x 4 hr, or (2) furosemide 4 mg/min x 4 h followed by 2 mg/min continuously (up to 3.4 g/d) or 1 g tid PO to maintain urine output at 150-200 mL/hr and/or SCr < 3.4 mg/dL
– 2 developed ototoxicity while on long-term furosemide therapy
– 1 developed irreversible deafness on day 11 after a clerical error led to 12 mg/min furosemide for 3 days (17.3 g/d)
– Another developed transient deafness after 11 days

Oral Furosemide Packaging in Europe

Long Term Safety of Diuretics in PD Faller and Lameire NDT 9:280, 1994
• 7 year observational study comparing two centers• At the center where diuretics were used 3 of 11 long term
pts became anuricVs.
• At the center where diuretics were not used 9 of 12 long term pts became anuric
• Diuretics routinely recommended by Lameire and Van Biesen (PDI 21:206, 2001) and Toronto (Khandelwal et al Adv PD 19:44, 2003) and my patients in Nashville

Reversal Of Target Organ DamageKonings C., et al. Kidney Int. 63:1556, 2003

Does Dry Weight Reduction Lower BP?Dry-Weight Reduction In Hypertensive Hemodialysis Patients
(DRIP)Agarwal et al Hypertension 53:on line, 2009
• RCT of sophisticated UF attack in 100 randomized to UF vs. 50 controls
• Average UF over 8 weeks was 1 kg• Systolic BP reduced 7 mmHg
– Odds ratio for systolic BP reduction in UF pts over controls was 2.24
• Increase in side effects, but Quality of Life scores were not different

6th Accord Workshop (Europe)Locatelli et al NDT 19:1058, 2004
• Target 140/90 or the lowest possible values that are well tolerated
• Pathophysiologic cornerstone to HT in dialysis pts is Na-sensitive volume
• Achieve dry wt, via diet and dialysis prescription• Then use pharmacologic intervention
– RAAS blockers first

6th Accord Workshop (Europe)Locatelli et al NDT 19:1058, 2004
• Target 140/90 or the lowest possible values that are well tolerated
• Pathophysiologic cornerstone to HT in dialysis pts is Na-sensitive volume
• Achieve dry wt, via diet and dialysis prescription• Then use pharmacologic intervention
– RAAS blockers first