Embed Size (px)
DESCRIPTION
power point presentation from BSN 3 FISHER of FILAMER CHRISTIAN COLLEGE, ROXAS CITY CAPIZ.
Citation preview

Diseases of the Reproductive OrganDiseases of the Reproductive Organ
A presentation by Group 6A presentation by Group 6
Azarcon,Raymond PaulAzarcon,Raymond PaulBlances, LorgieBlances, Lorgie
Dayao, MildaleneDayao, MildaleneFaelangco, JoywilineFaelangco, Joywiline
Ferrer, Ma GressiaFerrer, Ma GressiaPimentel, RoselynPimentel, Roselyn

Female Reproductive OrganFemale Reproductive Organ

ENDOMETRENDOMETRIOSISIOSIS

EndometriosisEndometriosis
Video Presentation

Schematic DiagramSchematic Diagram
(During menstrual period)Endometrial cells are stimulated by the ovarian
hormones
Some of the endometrial debrisexits the uterus
passing the fallopian tube
attach to peritoneal surface
invade tissues
endometriosis

Assessment FindingsAssessment Findings
• pelvic pain• dysuria
• dysmenorrhea • dyspareunia• diarrhea or constipation
• Fatigue• heavy or irregular
bleeding• Infertility
DiagnosticsDiagnostics
•Pelvic exam shows pelvis abnormalities such as cyst on the reproductive organs or scar behind the uterus.
•Ultrasound shows cysts associated with endometriosis.
•Laparoscopy shows signs of endometrial implants.
•Blood test shows positive in Cancer Antigen (CA 125) also used to detect a certain protein found in the blood of women with endometriosis.

Nursing DiagnosisNursing Diagnosis
•Pain related to dyspareunia and pelvic pain.•Disturbed self-esteem disturbance related to difficult management of the disease.•Knowledge Deficit related to surgical procedure and possible outcomes of the surgery•Risk for Dysfunctional Grieving related to loss of reproductive capacity and perceived loss of feminity.•Risk for infection related to surgical intervention
ComplicationsComplications
•Internal scarring
•Adhesions
•Pelvic cysts
•Chocolate cysts
•Ruptured cyst
•impaired fertility

Medical InterventionsMedical Interventions
Pain medications help ease painful menstrual cramps.(NSAIDS)
Hormonal contraceptives. Using hormonal contraceptives — especially continuous cycle regimens — can reduce or eliminate the pain of mild to moderate endometriosis.
Gonadotropin-releasing hormone (Gn-RH) agonists and antagonists. blocks the production of ovarian-stimulating hormones. Prevents menstruation and dramatically lowers estrogen levels.
Danazol. blocks the production of ovarian-stimulating hormones, preventing menstruation and the symptoms of endometriosis, is danazol
Medroxyprogesterone (Depo-Provera). This injectable drug is effective in halting menstruation and the growth of endometrial implants, thereby relieving the signs and symptoms of endometriosis.

Surgical InterventionsSurgical Interventions
>Conservative surgery>Hysterectomy
a total hysterectomy and the removal of both ovaries may be the best treatment. Hysterectomy alone is also effective, but removing the ovaries ensures that endometriosis will not return.
Nursing InterventionsNursing InterventionsPROMOTIVEProper diet
Daily exercise
Monthly check-up
Good lifestyle
CURATIVEAdminister pain
medications as orderedAdminister hormone
therapy as prescribedIn severe cases, prepare
patient for surgery
REHABILITATIVEFollow up check-up with the physician

OVARIAN OVARIAN CYSTSCYSTS

It is any collection of fluid, surrounded by a very thin wall, within an ovary. Any ovarian follicle that is larger than about two centimeters is termed an ovarian cyst. An ovarian cyst can be as small as a pea, or larger than a cantaloupe.
Ovarian CystOvarian Cyst

Types and CauseTypes and Cause
>Corpus luteum cystThis type of functional cyst occurs after an egg has been released from a follicle.
>Hemorrhagic cystIt occurs when a very small blood vessel in the wall of the cyst breaks, and the blood enters the cyst.
>Endometrioid cystformed when a tiny patch of endometrial tissue bleeds, sloughs off, becomes transplanted, and grows and enlarges inside the ovaries.
>Dermoid cyst
This cyst is similar to those present on skin tissue and can contain fat and occasionally bone, hair, and cartilage. >Cystadenoma A cystadenoma is a type of benign tumor that develops from ovarian tissue.

AssessmentAssessment
• May be asymptomatic or cause minor pelvic pain
• Possible menstrual irregularity.
• Tender, palpable mass.
• Rapture cause acute pain and tenderness, may mimic appendicitis or ectopic pregnancy.
Nursing diagnosisNursing diagnosis
• Acute pain related to abnormal growth,
• Risk for deficient Fluid Volume related to rupture of cyst or post operative changes in intra abdominal pressure
• Anxiety related to infertility.
• Knowledge Deficit related to surgical procedure and possible outcomes of the surgery
• Disturbed self-esteem disturbance related to difficult management of the disease.

DiagnosticsDiagnostics
Ultrasonography• help define morphologic characteristics of ovarian cysts.
Doppler flow studies • help identify blood flow within a cyst wall and adjacent areas, including
tumor surface, septa, solid parts within the tumor, and peritumorous ovarian stroma.
• helpful in diagnosis purposes.
CT scan • allows examination of the abdominal contents and retroperitoneum in
cases of malignant ovarian disease.
Pregnancy test. • A positive pregnancy test may suggest that your cyst is a corpus luteum
cyst, which can develop when the ruptured follicle that released your egg reseals and fills with fluid.

Laboratory StudiesLaboratory Studies
Culdocentesis: • This test involves taking a fluid sample from the pelvis with a needle
inserted through the vaginal wall behind the uterine cervix.
Hormone levels: • A blood test to check LH, FSH, estradiol, and testosterone levels may
indicate potential problems concerning these hormone levels.

>Oral contraceptives: Birth control pills may be helpful to regulate the menstrual
cycle, prevent the formation of follicles that can turn into cysts, and possibly reduce
the size of an existing cyst.
>Pain relievers: Anti-inflammatories such as ibuprofen (for example, Advil) may help reduce pelvic pain. Narcotic pain medications by prescription may relieve severe pain caused by ovarian cysts.
Surgical InterventionsSurgical Interventions
Cystectomy (can be removed without removing the ovary in
a procedure).
Oophorectomy (removing the affected ovary and leaving the other intact in a procedure ).
Hysterectomy (removal of both ovaries and your uterus ).
Medical InterventionsMedical Interventions

PromotiveEat proper diet
Regular check upRegular exercise
PreventiveRegular pelvic examinationRegular check up with the
physicianRehabilitative
Follow up check upCheck for bleeding

CurativeAdminister pain reliever as ordered
Advise to void as soon as the urge present itselfAdvise to eat high fiber diet to avoid constipation
Advise to limit strenuous activitiesEliminate caffeine and alcohol containing food
Advise to reduce intake of sugar containing foodsAdminister hormonal contraceptive as ordered
In severe cases, prepare patient for surgery

DYSMENORRDYSMENORRHEALHEAL

DYSMENORRHEALDYSMENORRHEAL
Dysmenorrhea refers to the syndrome of painful menstruation..Dysmenorrhea is
severe, frequent cramping during menstruation. Pain occurs in the lower abdomen but can
spread to the lower back and thighs.
2 types:
Primary dysmenorrhea. Secondary dysmenorrhea.

Risk FactorsRisk Factors
•Primary dysmenorrhea •Early age at menarche ( <12 y) •Nulliparity •Heavy or prolonged menstrual flow•Positive family history •Obesity
•Secondary dysmenorrhea •Endometriosis •Adenomyosis •Leiomyomata (fibroids) •Intrauterine device •Pelvic inflammatory disease •Endometrial carcinoma •Ovarian cysts •Congenital pelvic malformations •Cervical stenosis

Schematic DiagramSchematic Diagram
During Menstrual Cycle
Sloughing endometrial cells
Release of Prostaglandins
Strong myometrial contraction
Constrict blood vessels (uterus)
Ishemia and pain
DYSMENORRHEA

AssessmentAssessment
Primary dysmenorrhea •Onset within 6-12 months after menarche •Lower abdominal/pelvic pain begins with onset of menses and lasts 8-72 hours •Low back pain •Medial/anterior thigh pain •Headache •Diarrhea •Nausea/vomiting
Secondary dysmenorrhea •Onset in 20s or 30s, after relatively painless menstrual cycles in the past •Infertility •Heavy menstrual flow or irregular bleeding •Dyspareunia •Vaginal discharge •Lower abdominal or pelvic pain during times other than menses •Pain unrelieved by nonsteroidal anti-inflammatory drugs (NSAIDs)

>Oral contraceptives, which block monthly ovulation and may decrease menstrual flow, may also relieve symptoms.
>Nonsteroidal anti-inflammatory agents:
These drugs are highly effective in treating
dysmenorrhea, especially when they are started before the
onset of menses and continued through day 2.
>Acute pain related to severe muscle spasms>Impaired comfort related to pain>Ineffective role performance related to severe discomfort>Risk for situational low self-esteem related to pain->Impaired social interaction related to severe discomfort-
Medical InterventionMedical Intervention Nsg. DiagnosisNsg. Diagnosis

Exams and TestExams and TestLaboratory studies may be indicated to elucidate the cause of secondary dysmenorrhea:.
•Complete blood count (•Urinalysis, •Quantitative human chorionic gonadotropin level, •Gonococcal/chlamydial cervical swabs, •Stool guaiac, •Erythrocyte sedimentation rate (ESR),
Imaging Studies
•abdominal and/or transvaginal Ultrasonography.
•MRI

Nursing InterventionsNursing Interventions
PROMOTIVE •Health education ( provide information about dysmenorrhea)•Encourage adequate nutrition•Decreased caffeine intake•Appropriate rest and sleep
PREVENTIVE•Decreased intake of sodium•avoidance of caffeine•avoidance of alcohol•avoidance of sugar•quitting smoking•taking daily multi-vitamin and mineral supplements
CURATIVE•acupuncture•aromatherapy•transcutaneous electrical nerve stimulation•NSAIDs•IUD
REHABILITATIVE•exercise•yoga

PRE-PRE-MENSTRUAL MENSTRUAL DYSPHORHIC DYSPHORHIC
DISORDERDISORDER

Premenstrual Dysphoric Disorder
Premenstrual dysphoric disorder (PMDD) is a diagnosis used to indicate
serious premenstrual distress with associated deterioration in functioning.
PMDD is characterized by depressed or labile mood, anxiety, irritability, anger,
and other symptoms occurring exclusively during the 2 weeks
preceding menses.

AssessmentAssessment•Depressive symptoms
Markedly depressed mood, feelings of hopelessness, self-depreciation
Suddenly feeling sad or tearful, with increased sensitivity to personal rejection Decreased interest in usual activities Lethargy, fatigue, marked lack of energy Accompanying depressive symptoms there is always the danger for suicidal ideation and behavior. Marked changes in appetite and cravings for certain foods Insomnia or hypersomnia
•Anxiety symptoms Marked anxiety, tension, feeling of being keyed-up or on-edge Persistent or marked irritability, anger, increased interpersonal
conflicts Feeling overwhelmed or out of control
•Cognitive symptoms - Subjective sense of having difficulty concentrating
•Physical symptoms - Breast tenderness or swelling, headaches, joint or muscular pain, weight gain, bloated feeling

Nursing DiagnosisNursing Diagnosis
•Ineffective role performance related to premenstrual depression-premenstrual depression result to self-depreciation
•Impaired social interaction related to depressed mood- depressed mood develops to decreased interest in social activities
•Ineffective coping related to increased sensitivity- increased sensitivity results to personal rejection
•Knowledge deficit related to ignorance of symptoms- premenstrual mood changes as one of the risk factor might be perceived as normal until become severe.
•Anxiety related to suicidal ideation- severe depression could lead to suicidal attempt

Pharmacological treatment
•Vitamins and minerals
•Hormones
•Diuretics
•Nonsteroidal anti-inflammatory drugs
•Anxiolytics, antidepressants, and mood stabilizers:
•Hysterectomy alone also resulted in a reduction of symptoms, but the validity of these trials is questionable because conducting blinded studies was logistically difficult.
•Limited data are available on laparoscopic bilateral oophorectomy and endometrial ablation in the treatment of PMDD.
Medical InterventionsMedical Interventions Nursing DiagnosisNursing Diagnosis

Nursing InterventionsNursing Interventions
PROMOTIVE
•Patient Education•Educate women to seek help for PMDD. Emphasize the following reasons for the need to seek help:
•Problems tend to recur each cycle. •Problems may become more severe over time. •Problems can be quite disabling to women and their families. •Problems may not go away if ignored. •Problems can be readily diagnosed and effectively treated.
•Educate both the patient and the family/spouse as this disorder impacts on the entire family context.

Nursing InterventionsNursing Interventions
PREVENTIVE •Diet•Restricting sodium intake may reduce bloating. Activity moderate aerobic exercise improved premenstrual symptoms; In addition, aerobic exercise has not been consistently beneficial in alleviating the symptoms of PMDD
CURATIVE•vitamins and minerals•hormones•diuretics•NSAIDs•anxiolytics,antidepressants,mood stabilizers•surgical care
REHABILITATIVE•regular exercise•balance diet•adequate rest

VAGINAL VAGINAL FISTULASFISTULAS

Vaginal FistulaVaginal Fistula
A vaginal fistula is an abnormal passage that connects the vagina to other organs, such as the bladder or rectum, resulting in leakage of urine or feces into the vagina.
Vaginal fistulas are classified into
four types; treatment varies for each:
a) Vesicovaginal fistulas,
b) Uterovaginal fistulas
c) Urethrovaginal fistulas
d) Rectovaginal fistulas,

Schematic DiagramSchematic Diagram
Ureterovaginal Fistula
Dissection around the infundibulopelvic ligament/ ligation of the uterine vessels
The ureter may become injured
Unexpected pelvic hemorrhage
Ureteral injury
Ureterovaginal fistula

AssessmentAssessment
Clinical manifestations:
• urine or flatus and feces leak into the vagina• rectovaginal fistula may cause an offensive/unpleasant odor• client experiences wetness and a sensation of feeling unclean• painless unremitting urinary incontinence. • may experience constitutional symptoms of fever, chills, malaise, flank pain, and gastrointestinal symptoms in association with continuous urinary incontinence. • If the Foley catheter is still in place, the first sign of fistula formation is the presence of hematuria.

Exams and TestsExams and Tests
• Putting dye in the vagina (and maybe the bladder or rectum) to find all signs of leakage.
• Urinalysis •Blood test (complete blood count) • X-ray •Barium enema•Computed tomography (CT)•Flexible Endoscopy
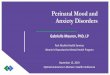
Sigmoidovaginal fistula in a woman with a history of hysterectomy. Vaginogram shows a fistula involving the vaginal cuff (arrow). The vagina (V), sigmoid colon (S), and rectum (R) are highlighted by the contrast material.

Diagnostic ProceduresDiagnostic Procedures Vesicovaginal, Ureterovaginal and Urethrovaginal Fistulas
Preoperative-Informrd consent should be obtained
Intraoperative- Place the patient in a dorsal lithotomy position- Insert a percutaneous suprapubic tube and urethral catheter
Postoperative- Continue intravenous antibiotics until the patient is able to tolerate
an oral diet- To prevent bladder spasms, give anticholinergics as prescribed by
physician- Remove pelvic drains when the output becomes minimal, usually
prior to discharge.
Cont.

ComplicationsComplications
The most common complications are bleeding and wound infection
- If bleeding occurs beneath the flap
- Infection results in a failed repair.
- postoperative pain precipitates urinary retention
- fistula recurrence

v
- drainage of abscesses- directed antibiotic
therapy to treat acute rectovaginal fistulas (RVFs) -Allow tissues to heal for 6-12 weeks.
- infliximab (Remicade)7
- Diet and fiber are the mainstays of therapy.
Local repair methods
-Transanal advancement flap repair
-Transvaginal inversion repair- Bioprosthetic repair
Medical InterventionsMedical Interventions Nursing DiagnosisNursing Diagnosis

Nursing Interventions Nursing Interventions Promotive
-encourage women to have prenatal check ups-encourge pregnany women to deliver in hospitals or clinics
Preventive-educational programs about the causes of the diseases for rural areas
Curative -may need to give medicine or wound care to heal the tissue before
surgery to client as prescribed by the physician.
Rehabilitative-Patients are seen 2 weeks after discharge for evaluation of wounds and bowel habits.-Offer sips of clear liquids to patient on the first postoperative day.- Early ambulation is beneficial for the patient-instruct patient to refrain from sexual activity or any physical activity more strenuous than a slow walk for 3 weeks.

UTERINE UTERINE PROLAPSEPROLAPSE
DD

Uterine prolapsed means your uterus has descended from its position in the pelvis farther down into your vagina.
Uterine ProlapsedUterine Prolapsed

Schematic DiagramSchematic Diagram
Menopause, multiparity, child birth trauma, chomic straining
Decrease in circulating estrogen
Lose of elasticity and ability to support of supporting structure of the pelvic floor
Relaxation and Prolapsed of urogenital organs

PathophysiologyPathophysiologyPossible risk factors
• Intrapartum variables (controversial and unproven): Fetal macrosomia
Prolonged second stage of labourEpisiotomy
Race• Family history of prolapse• Constipation• Previous hysterectomy• Menopause: a recent small study found no association between oestrogen
status and prolapse• Occupations involving heavy lifting• one or more vaginal deliveries.• Damage sustained by supportive tissues during pregnancy and childbirth,
plus the effects of gravity, loss of estrogen and repeated straining over the years

AssessmentAssessment
Symptoms
• Sensation of pressure, fullness or heaviness
• Sensation of a bulge/protrusion or 'something coming down'
• feeling of bulge/protrusion
• Difficulty retaining tampons
• Spotting (in the presence of ulceration of the prolapsed)
Urinary symptoms• Incontinence• Frequency• Urgency• Feeling of incomplete bladder
emptying• Weak or prolonged urinary stream• The need to manually reduce the
prolapse before voiding• The need to change position to
start or complete voiding
Coital difficulty• Dyspareunia• Loss of vaginal sensation• Vaginal flatus

AssessmentAssessment
Bowel symptoms
• Constipation/straining• Urgency of stool• Incontinence of flatus or stool• Incomplete evacuation• The need to apply digital pressure to
the perineum or posterior vaginal wall to enable defaecation (splinting)
• Digital evacuation necessary in order to pass stool

DiagnosticsDiagnosticsPreoperative- Ensure the patient's bladder and bowel are empty before surgery-obtain informed consent
Intraoperative-insert catheter
Postoperative- prevent bladder distension-removed catheter as ordered by the physician and as soon as client is
ambulatory-monitor bleedingInstruct and teach the patient to:-keep bladder empty by voiding every 2 hours to avoid placing pressure along
the suture line- avoid any exercise or heavy lifting-refrain from intercourse for 6 weeks after her discharge from the hospital.- avoid causes of increased intra-abdominal pressure, such as constipation,
weight lifting, and cigarette smoking, for at least 3 months.

ComplicationsComplications
• Ulceration and infection of organs prolapsed outside the vaginal introitus may occur.
• Urinary tract complications include stress incontinence, chronic retention and overflow incontinence, and recurrent urinary tract infections.
• Bowel dysfunction may occur with a rectocele.

Nursing DiagnosisNursing Diagnosis
• Pain • Constipation • Urinary Incontinence • Sexual dysfunction • Risk for Infection :Risk for
Infection Observe for localized signs of infection. Note for signs and symptoms for sepsis. Stress proper hand hygiene.

Pelvic exercises and pessaries are the current mainstays of nonsurgical management of patients with UP.
- Gellhorn pessaries is most often used for patients with significant UP and a large introital diameter who have not obtained relief with other pessaries
-Hysterectomy- performed by way of incisions through the vaginal wall into the pelvic cavity and supportive structure. The uterus is removed from its supporting brood, round, and uterosacral ligaments. The supprting ligaments are then attached to the vaginal cuff to maintain vaginal length.
-The 3 common vaginal procedures to suspend the prolapsed vaginal apex are sacrospinous ligament fixation, modified McCall culdoplasty, and iliococcygeus fascia suspension.
Medical InterventionsMedical Interventions Nursing DiagnosisNursing Diagnosis

Nursing CareNursing Care Prevention :
• Good intrapartum care• Pelvic floor exercises• Smoking cessation will
reduce chronic cough.• Weight loss if overweight or
obese.• Avoidance of heavy lifting
occupations.• Treatment of constipation
throughout life.• Estrogen replacement
therapy in postmenopausal women tends to help maintain muscle tone.
Promotive
-educational programs about the causes of the diseases for rural areas
Rehabilitative- teach patient how to insert,
clean, and remove the pessary herself
- If the woman is obese, attaining and maintaining optimal weight is recommended. Teach to avoid heavy lifting or straining.
- Measures to treat and prevent chronic cough, such as smoking cessation, are also recommended.

RECTAL RECTAL PROLAPSEPROLAPSE
DD

Rectal prolapsed occurs when part or all of the wall of the rectum slides out of place, sometimes sticking out of the anus.
There are three types of rectal prolapsed:
• Partial prolapsed
or mucosal prolapsed
• Complete prolapsed
• Internal prolapsed
or intussusception
Rectal ProlapsedRectal Prolapsed

AssessmentAssessment
Perianal Assessment:
•Swollen, painful, longitudinal breaks in the anal area may appear in Px with anal fissures.• Dilated anal veins appear with hemorrhoids• A red mass may appear with prolapsed internal hemorrhoids or rectal prolapsed.•Doughnut-shaped red tissue at the anal area may appear with prolapsed rectum.•Movable, soft masses may be polyps.•Hard, firm, irregular embedded masses may indicate carcinoma.

Exams and TestsExams and Tests
-A Defecogram (a test that evaluates bowel control) may help distinguish between a mucosal prolapsed and a complete prolapsed.
-It is confirmed by Sigmoidoscopy (inspection of the colon with a viewing instrument called a endoscope) - Barium Enema

ComplicationsComplications
Rectal prolapsed that is not treated can lead to complications.
• Fecal incontinence•a sore (ulcer) that may bleed. • (gangrene). • If a prolapsed rectum swells, it may prevent the passage of stools. • Rarely, a loop of the large intestine is pinched off (strangulated), causing blockage of the intestine (bowel obstruction).

Nursing DiagnosisNursing Diagnosis
•Pain related to inflamed anal tissues.
•Constipation related to dietary habits and/or delay of defecation.
•Risk for infection related to disruption of anal tissue.

MedicationMedication
Stool softeners, such as:
• sodium docusate (Colace)• calcium docusate (Surfak)
-may be used to reduce pain and straining during bowel movements.
Bulk agents, such as:
• psyllium (Metamucil or Fiberall)• methylcellulose (Citrucel) may also be used.
Docusate

SurgerySurgery
Surgery through the abdomen
•Typically performed in younger or healthier people• Type of abdominal surgery usually determined by severity of associated constipation• Associated with higher morbidity rate than perineal approach but lower recurrence rate of prolapsed• Performed under general anesthesia• Usually involves a hospital stay of 3-7 days
Perianal Approach
•Typically performed in elderly people or people in poor health•Approach for people who cannot tolerate general anesthesia•Associated with higher recurrence rate than abdominal approach•Usually involves short hospital stay
For people too weak for surgery, a doctor can prevent a prolapsed by inserting a wire or plastic loop to hold the sphincter closed.

A high-fiber diet and a daily intake of plenty of fluids can reduce a person's risk of developing constipation.
Straining during bowel movements should be avoided. A person with long-term diarrhea, constipation, or hemorrhoids should seek medical attention to treat these conditions in order to lessen the chance of developing a prolapsed rectum.
Self Care at Home
For infants and children, reducing the need to strain during bowel movements with stool softeners may correct a prolapsed rectum. Strapping the child's buttocks together between bowel movements may cause the rectum to heal on its own. A doctor should always be consulted before any attempt to treat this condition at home.
PreventionPrevention RehabilitativeRehabilitative

IMPERFORAIMPERFORATED HYMENTED HYMEN

►An imperforate hymen can be diagnosed at birth but sometimes the diagnosis isn't made until the teen years. An imperforate hymen is a thin membrane that completely covers the opening to a young girl's or young woman's vagina.
Imperforated HymenImperforated Hymen

Schematic DiagramSchematic Diagram
Obstruction of the vaginal tract (at the level of introitus)
Prenatal, perinatal, adolescent period
Intrapment of vaginal and uterine secretions
Becomes evident when the distensible membranes bulges in the vagina between the labia
Complications and sequelae of Imperforate hymen from the Diseases Database include:
•Haematocolpos•Amenorrhoea •Haematometra•Dyspareunia
•Hydrometrocolpos•Hematosalpinx

AssessmentAssessment
Additional TestingAdditional Testing
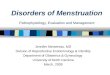
Prior to surgery, computed tomography Prior to surgery, computed tomography (CT) scanning was performed to further (CT) scanning was performed to further delineate pelvic anatomy. Hematocolpos delineate pelvic anatomy. Hematocolpos and hematometra were notedand hematometra were noted
common forms:
•imperforate: hymen completely covers vaginal orifice; will require minor surgery if it has not corrected itself by puberty to allow menstrual fluids to escape
No menstrual bleeding
Pelvic examination revealed normal labia, but
a large bulging imperforate hymen was
seen upon their separation

Nursing DiagnosisNursing Diagnosis
>Amenorrhoea
>Haematometra
>Dyspareunia
>Hydrometrocolpos
>Haematocolpos

Surgical InterventionSurgical Intervention
HymenectomyA Hymenectomy (hymenotomy) surgical removal or opening of the hymen.
Preoperative. Preoperative pelvic and abdominal ultrasound to view the kidneys and urinary tract as many patients with hematocolpos have pelvic adhesions which could lead to ureteric obstruction and hence subsequent renal failure.
PostoperativeIbuprofen or other nonsteroidal anti-inflammatory drugs (NSAIDs) may be prescribed for the cramping. Topical lidocaine jelly is recommended for the vaginal orifice.

Medical InterventionsMedical Interventions
Medical Therapy
After initial presentation and suspected diagnosis of an obstructive anomaly, the use of continually-administered oral contraceptive pills to suppress menses allows symptomatic relief and essential time needed to obtain further diagnostic studies. In addition, the use of nonsteroidal anti-inflammatories can provide pain relief.

Nursing InterventionsNursing Interventions
Promotive careSafe Motherhood
Rehabilitative care-Follow-up
Schedule a postoperative office visit 1-2 weeks after the surgical procedure. At that visit, inspect the area for signs of inflammation or infection. Topical lidocaine jelly facilitates the examination and helps relieve the patient's anxiety. A 3- to 6-month course (or longer) of menstrual suppression with continuous oral contraceptive pills may be indicated and should be discussed at the postoperative visit.

TOXIC TOXIC SHOCK SHOCK
SYNDROMESYNDROME

Toxic shock syndrome (TSS) is a rare, often life-threatening illness that develops suddenly after an infection and can rapidly affect several different organ systems, including the lungs, kidneys, and liver.
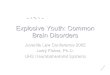
Toxic shock syndrome commonly causes a red strawberry tongue.
This woman with toxic shock syndrome developed a flat, red, sunburn-like-rash. This rash causes the skin to peel 1-2 weeks after the illness.
What is toxic shock syndrome?What is toxic shock syndrome?

Schematic DiagramSchematic Diagram
Presence of Strep/Stap
Produces Endotoxins
Binding of MNC II with T cell receptors
Polyclonal T cell activation
Cytokine storm- related to the immune system
Multi system disease (Lungs, Liver and Kidney)

AssessmentAssessment
• Fever greater than 102°F (38.9°C) • Rash Redness of the eyes, the lips, and the tongue [strawberry tongue] may also occur.) • Headache• Muscle aches • Sore Throat • Cough • Nausea and vomiting • Diarrhea Abdominal Pain• Lightheadedness or Fainting (especially on standing up)
Cont.

Exams and TestsExams and Tests
• complete blood count (CBC) of red and white blood cells, platelets, and other basic qualities of your blood.
• Cultures of blood and other body fluids and tissues for signs of strep and staph bacteria. •Chest X-ray, to look for signs of damage to the lungs (respiratory distress syndrome).

Medical interventionMedical intervention
Antibiotics. Clindamycin . Other medications, such as cloxacillin
or cefazolin, may be added. Strains of Staphylococcus aureus that
are resistant to medicines such as cloxacillin or cefazolin . vancomycin, daptomycin, linezolid, or
tigecycline.
Cont.

Surgical InterventionsSurgical Interventions
If the source of the infection is a tampon or other packing, removal of the tampon or packing is usually sufficient, and surgery is not necessary.
•If the source of the infection is in the skin, often no surgery is required. However, some instances arise when surgery is necessary to fully expose and drain a skin infection.•If the infection is found to be in deeper tissues, extensive surgery is often necessary to remove the infected and dead tissue (called debridement).

Nursing Diagnosis and InterventionsNursing Diagnosis and Interventions
Nursing DiagnosisNursing DiagnosisAnxietyAnxiety
Fluid volume deficitFluid volume deficitFatigueFatigue
HyperthermiaHyperthermia
Nursing InterventionsNursing InterventionsMonitor signs of dehydrationMonitor signs of dehydration
Increase fluid intakeIncrease fluid intake

Reference:Reference:
As
• http://www.healthline.com/images/adam/1112t.j
•6/6/2006www.nlm.nih.gov/medlineplus/ency/article/001508.htm#Definition
•© 1998-2009 Mayo Foundation for Medical Education and Research (MFMER). All rights reserved. A single copy of these materials may be reprinted for noncommercial personal use only. "Mayo," "Mayo Clinic," "MayoClinic.com," "EmbodyHealth," "Reliable tools for healthier lives," "Enhance your life," and the triple-shield Mayo Clinic logo are trademarks of Mayo Foundation for Medical Education and Research.
•www.mayoclinic.com/health/uterine-prolapse/DS00700
•www.emedicine.com/emerg/topic629.htm
Reference:Reference:
- Assessment
http://emedicine.medscape.com/
As
- Introduction- Etiology- Pathophysiology
Medical-Surgical Nursing 3rd Edition, Volume 1
By: Pricilla Lemone and Karen Burke
Copyright@2004 by Pearson Education, Inc.
Page 615
www.emedicinehealth.com/rectal_prolapse/
- Complications