Embed Size (px)
Citation preview
RENAL REPLACEMENT THERAPY
Speaker – Nagarjuna Moderator – Dr. Roopa vani
Definition :
• Renal replacement therapy is a term used to encompass life-supporting treatments for renal failure.
• It includes a variety of treatment modalities.
History :
• First hemodialysis in human being was done by Dr. HASS in 1924.
• First to construct a working dialyzer was Dr . WILLIAM KOLFF in 1943.
AKI :
• Most current consensus diagnostic criteria for AKI is abrupt ( 48 hrs ) reduction in kidney function , defined as :
absolute increase in S. Cr of >0.3mg/dl.
a % increase in S. Cr > 50% . reduction in urine output –
documented oliguria of <0.5ml/kg/hr for >6hrs.
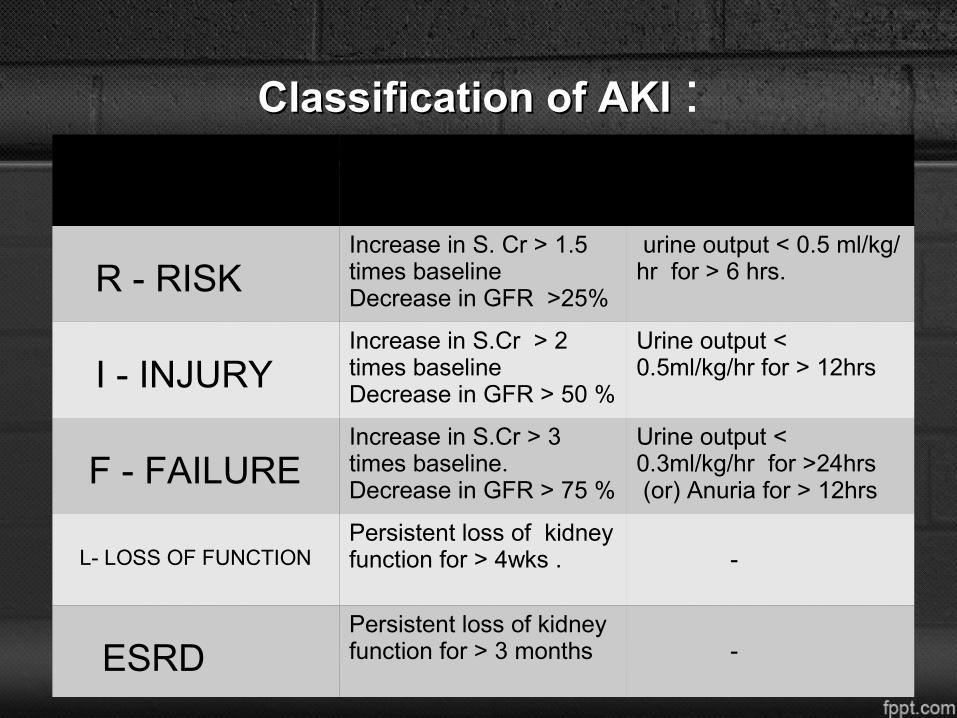
Classification of AKI Classification of AKI :
R - RISKIncrease in S. Cr > 1.5 times baselineDecrease in GFR >25%
urine output < 0.5 ml/kg/ hr for > 6 hrs.
I - INJURYIncrease in S.Cr > 2 times baselineDecrease in GFR > 50 %
Urine output < 0.5ml/kg/hr for > 12hrs
F - FAILUREIncrease in S.Cr > 3 times baseline.Decrease in GFR > 75 %
Urine output < 0.3ml/kg/hr for >24hrs (or) Anuria for > 12hrs
L- LOSS OF FUNCTIONPersistent loss of kidney function for > 4wks . -
ESRDPersistent loss of kidney function for > 3 months
-
INDICATIONS FOR RRT :
• RENAL : Symptomatic uremia Nephrogenic pulmonary edema Persistent hyper-kalemia(>6.5) Metabolic acidosis.(pH< 7.2 ) Relatively high urea and creatinine
NON – RENAL NON – RENAL :
• SIRS / sepsis.• Fluid imbalance.• Rhabdomyolysis.• Drug overdosage.• Temperature control.• Plasmapharesis.• Severe acute liver failure as a bridge to
transplant.
PrinciplesPrinciples :
• Whatever be the technique of RRT, the fundamental principle is the removal of unwanted SOLUTES & WATER through a semi-permeable membrane.
• WATER : Removal of water occurs through a
process of ULTRAFILTRATION.
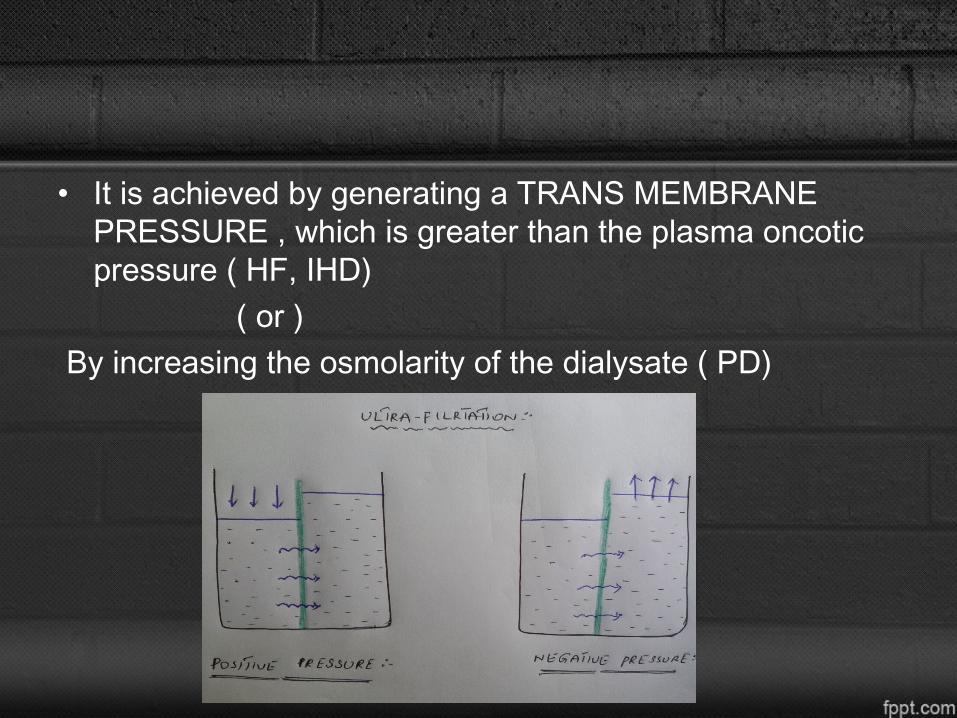
• It is achieved by generating a TRANS MEMBRANE PRESSURE , which is greater than the plasma oncotic pressure ( HF, IHD)
( or ) By increasing the osmolarity of the dialysate ( PD)
SOLUTE REMOVAL :SOLUTE REMOVAL :
• It occurs by either DIFFUSION or by CONVECTION ( SOLVENT DRAG ).
• In diffusion an electro-chemical gradient is created across the membrane with a dialysate solution.
Modes of RRT Modes of RRT :
• EXTRACORPOREAL : Intermittent Hemodialysis Slow low efficiency dialysis (SLED) Continuous Hemo-filtration o CAVHo CVVHo CAVHDFo CVVHDF INTRACORPOREAL : Peritoneal dialysis
Hemo dialysis Hemo dialysis ::
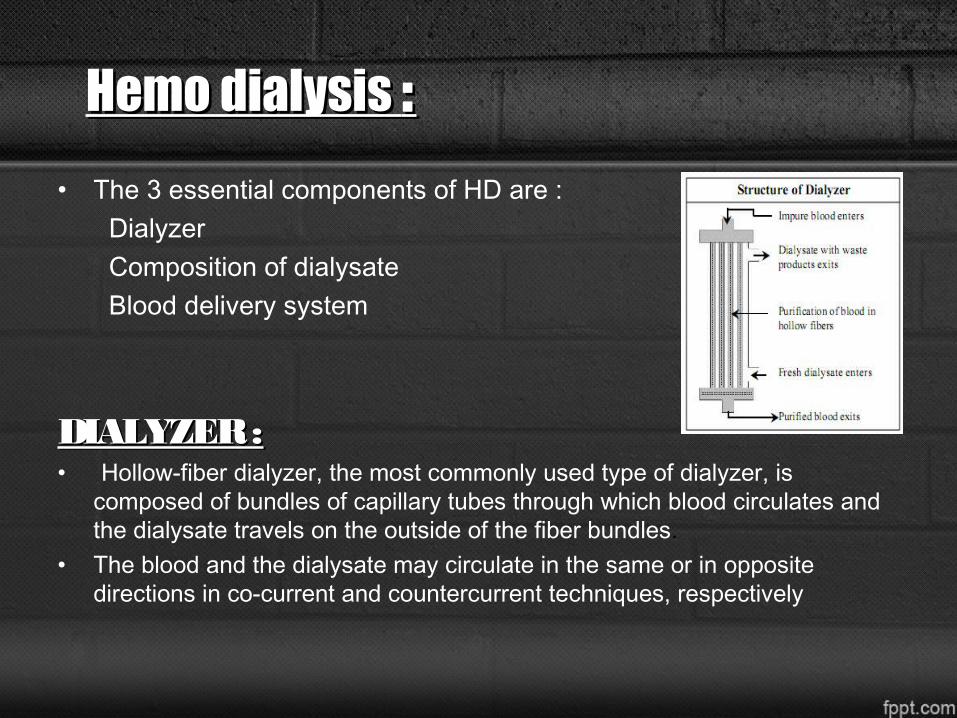
• The 3 essential components of HD are : Dialyzer Composition of dialysate Blood delivery system
DIALYZER :DIALYZER :• Hollow-fiber dialyzer, the most commonly used type of dialyzer, is
composed of bundles of capillary tubes through which blood circulates and the dialysate travels on the outside of the fiber bundles.
• The blood and the dialysate may circulate in the same or in opposite directions in co-current and countercurrent techniques, respectively
Dialysis membrane :
• It can be synthetic or biological.
Cellulose : .has low flux .poor in removing middle MW molecules. . More complement and leucocyte activation. . Not desirable in ICU patients. . Worsening of the organ damage.
• SYNTHETIC : High flux membranes.
Made up of PMMA, PAN, Polyamide, Polysulphone (PS).
Allows convective therapy and removal of middle MW substances.
Better biocompatibility, less leucocyte/complement activation and end organ dysfunction.
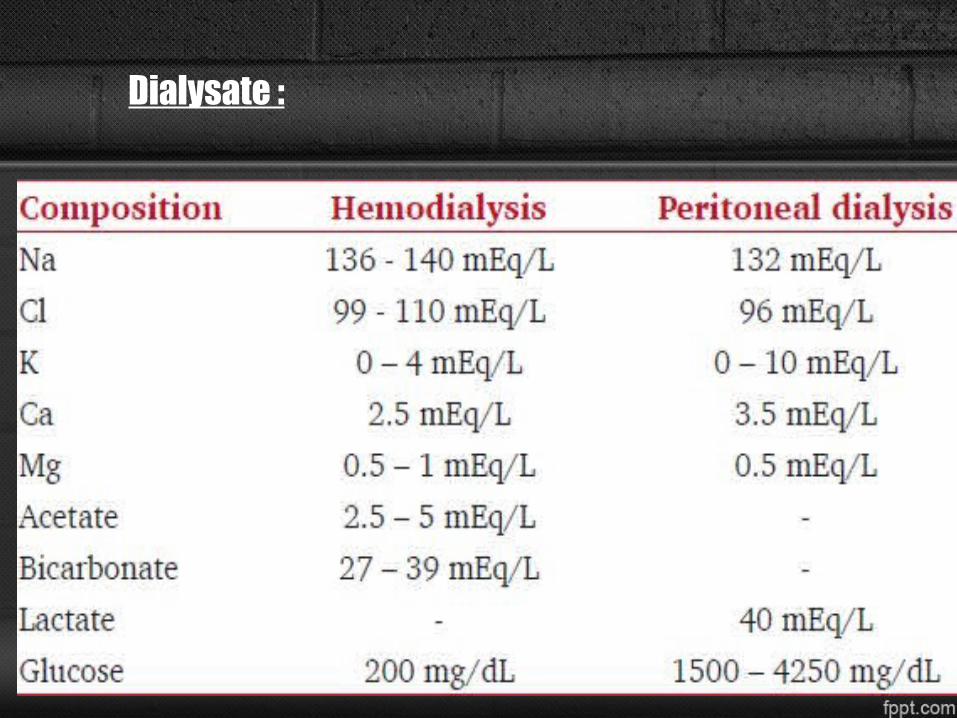
Dialysate :
Blood delivery system Blood delivery system :
• Consists of the extracorporeal circuit in the dialysis machine and the dialysis access .
• Types of vascular access can be Venous access
External shunt
AV fistula Internal shunt AV graft
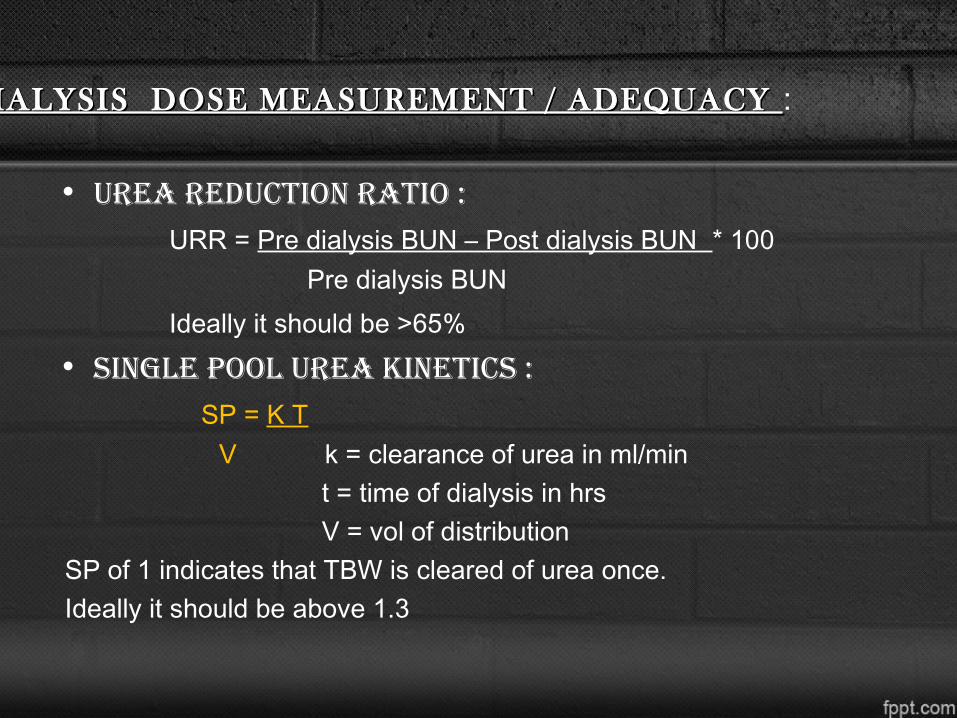
DIALYSIS DOSE MEASUREMENT / ADEQUACY DIALYSIS DOSE MEASUREMENT / ADEQUACY :
• UReA RedUCTIoN RATIo : URR = Pre dialysis BUN – Post dialysis BUN * 100 Pre dialysis BUN Ideally it should be >65%• sINgle pool UReA kINeTICs : SP = K T V k = clearance of urea in ml/min t = time of dialysis in hrs V = vol of distribution SP of 1 indicates that TBW is cleared of urea once. Ideally it should be above 1.3
CoMplICATIoNs wITh dIAlysIs :
• Hypotension ( mc complication).• Muscle cramps.• Dialysis dysequilibrium syndrome.• Dialyzer reactions.• Arrhythmias.• Cardiac arrest.• Intra-dialytic hemolysis.• Hypoglycemia.• Complications with water.• Infections .
ChroniC CompliCations ChroniC CompliCations ::
• Anemia
• Cardiovascular disease.
• Calciphylaxis .
• Vascular calcification .
• Nephrogenic systemic fibrosis .
• Nutrition & Infection .
SLOW LOW- EFFICIENCY DIALYSIS : ( SLED )SLOW LOW- EFFICIENCY DIALYSIS : ( SLED )
• Conventional dialysis treatment .
• Uses dialysate flow rates of 300 ml/min & low blood flow pump speeds of 200ml/min for 6 – 12 hrs a day.
• Excellent small molecule detoxification.
• Reduced anticoagulant requirement.
• 11 hrs SLED is comparable to 24 hrs of CHD .
• Decreased costs compared to CRRT.
CRRT :• Treatment occurs 24 hrs a day .
• Blood flow of 100-200ml/min .
• Dialysate flow of 15-40 ml/min .
• Membranes are of high flux .
• Useful in hemodynamically unstable patients with ARF , CRF, life threatening electrolyte imbalances , major burns and drug overdose.
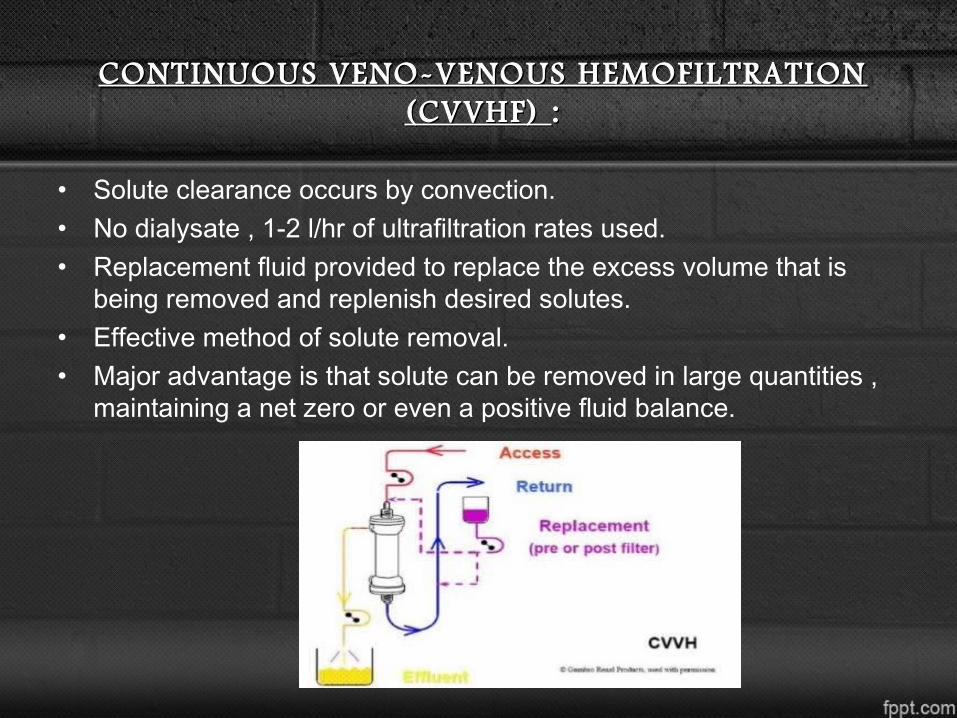
CONTINUOUS VENO-VENOUS HEMOFILTRATION CONTINUOUS VENO-VENOUS HEMOFILTRATION (CVVHF) (CVVHF) ::
• Solute clearance occurs by convection.• No dialysate , 1-2 l/hr of ultrafiltration rates used.• Replacement fluid provided to replace the excess volume that is
being removed and replenish desired solutes.• Effective method of solute removal.• Major advantage is that solute can be removed in large quantities ,
maintaining a net zero or even a positive fluid balance.
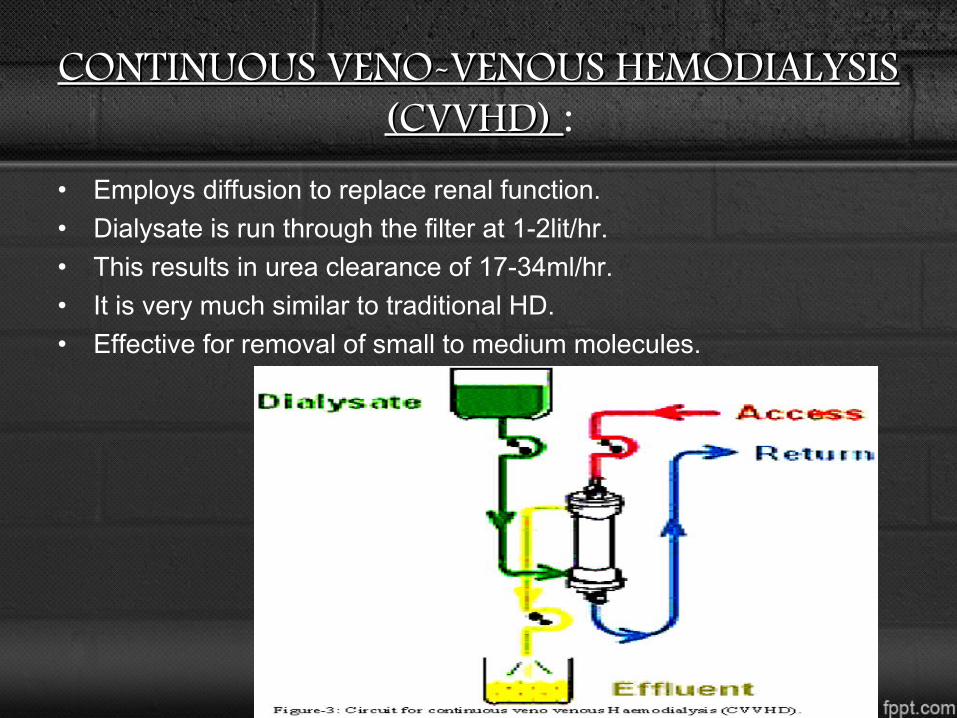
CONTINUOUS VENO-VENOUS HEMODIALYSIS CONTINUOUS VENO-VENOUS HEMODIALYSIS (CVVHD) (CVVHD) :
• Employs diffusion to replace renal function.• Dialysate is run through the filter at 1-2lit/hr.• This results in urea clearance of 17-34ml/hr.• It is very much similar to traditional HD.• Effective for removal of small to medium molecules.
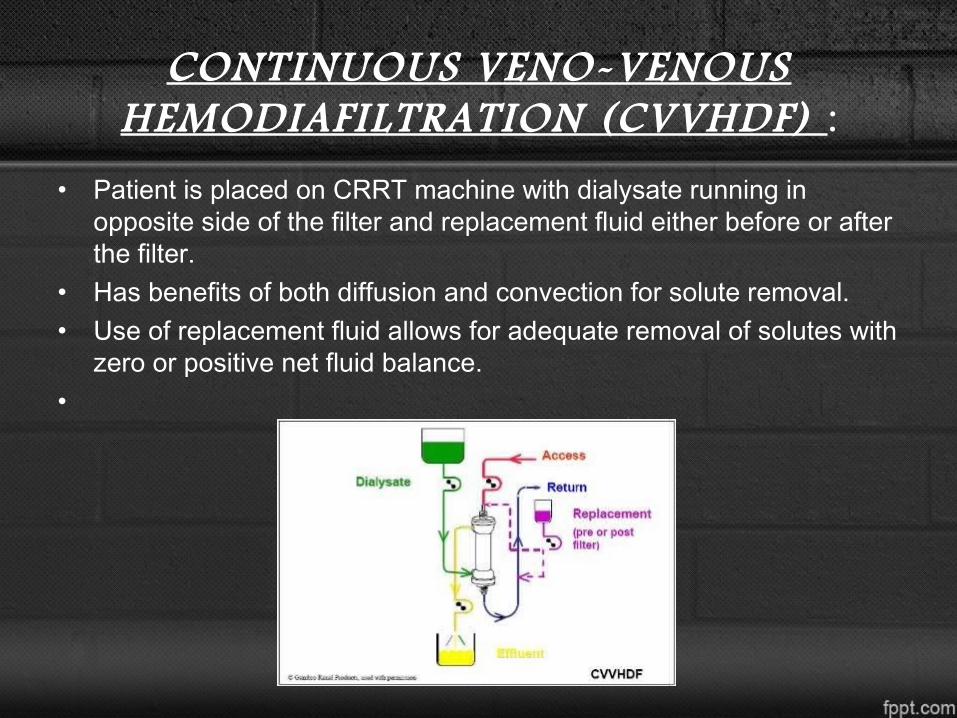
CONTINUOUS VENO-VENOUS HEMODIAFILTRATION (CVVHDF) :
• Patient is placed on CRRT machine with dialysate running in opposite side of the filter and replacement fluid either before or after the filter.
• Has benefits of both diffusion and convection for solute removal.• Use of replacement fluid allows for adequate removal of solutes with
zero or positive net fluid balance.•
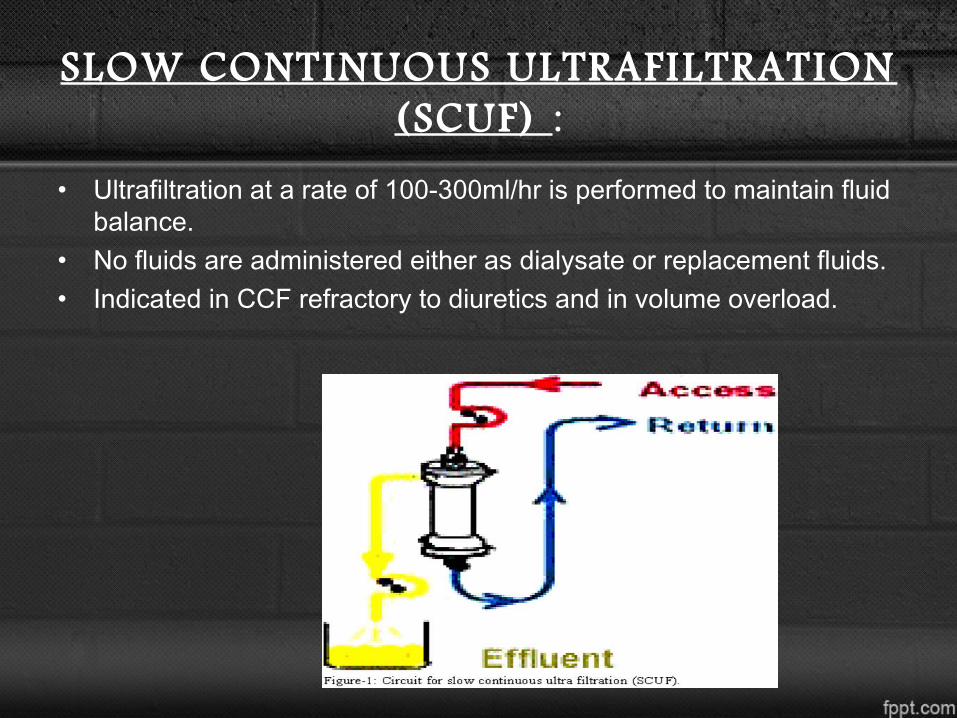
SLOW CONTINUOUS ULTRAFILTRATION (SCUF) :
• Ultrafiltration at a rate of 100-300ml/hr is performed to maintain fluid balance.
• No fluids are administered either as dialysate or replacement fluids.• Indicated in CCF refractory to diuretics and in volume overload.
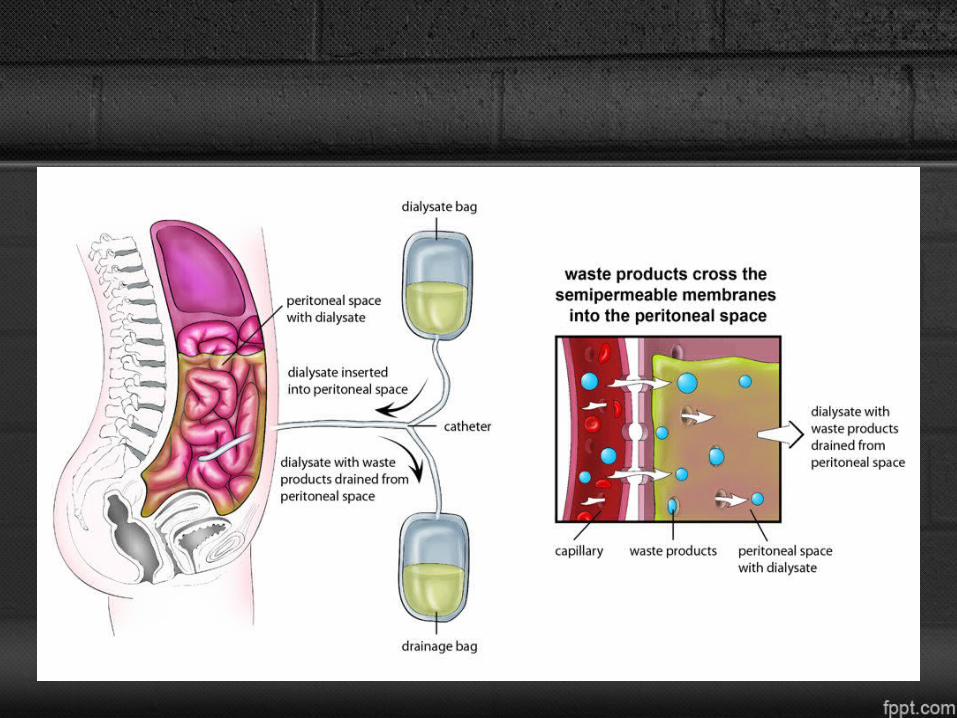
PERITONEAL DIALYSIS PERITONEAL DIALYSIS :
• In peritoneal dialysis, 1.5 – 3 L of peritoneal dialyzate solution is infused into the peritoneal cavity and allowed to dwell for a set period of time, usually 2 to 4 hours.
• The rate of diffusion diminishes with time and eventually stops when equilibration between plasma and dialyzate is reached..
• Lactate is the preferred buffer.• icodextrin, has been found to be associated with more efficient
ultrafiltration than dextrose-containing solutions.• It may be associated with the complication of ENCAPSULATING
PERITONEAL SCLEROSIS.
COMPLICATIONS COMPLICATIONS :
• Peritonitis .
• Catheter associated infections .
• Weight gain .
• unpredictable hyperglycemia .
• Protein loss .
• Interference with diaphragm function .
• Residual uremia .
• Peritoneal membrane failure.
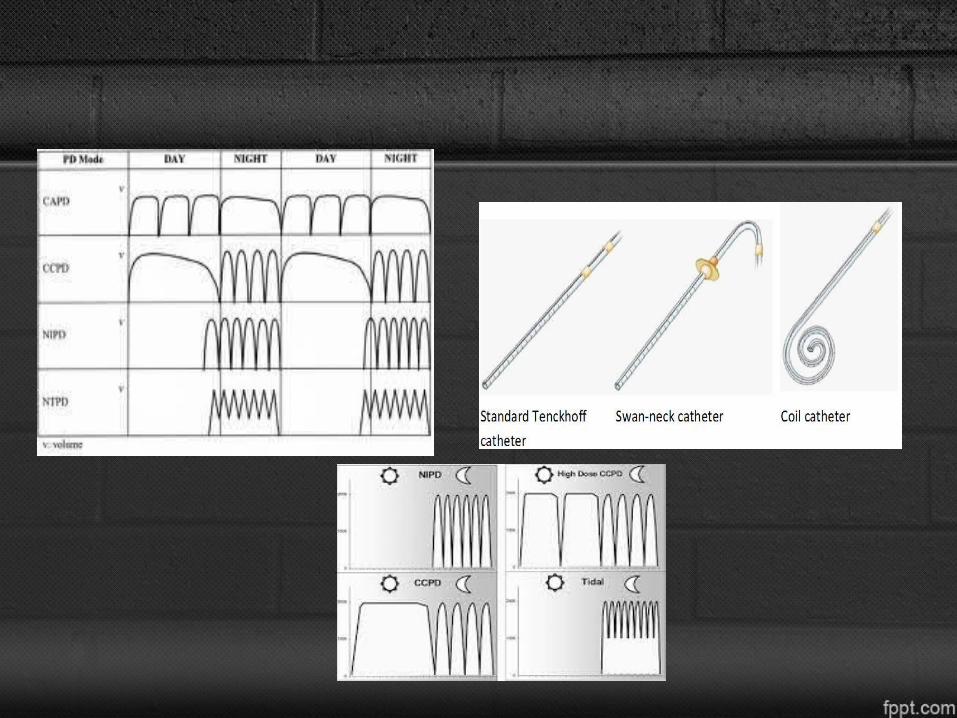
TYPES OF PD TYPES OF PD :
• Continuous ambulatory peritoneal dialysis ( CAPD ).
• Automated peritoneal dialysis (APD) : Continuous cycling peritoneal dialysis (CCPD) Nocturnal intermittent PD ( NIPD ) Tidal PD • Hybrid devices : Night exchange device PD plus
• Acute PD
ANTI-COAGULANTS IN DIALYSIS ANTI-COAGULANTS IN DIALYSIS :
• Interacting of blood with dialyzing membrane causes activation of clotting cascade – thrombosis-dysfunction.
• Commonly used anti-coagulant is HEPARIN .• SYSTEMIC ANTICOAGULATION SYSTEMIC ANTICOAGULATION : Administered in doses of 50-100u/kg at the initiation followed by
a bolus of 100u/hr.
• REGIONAL ANTICOAGULATION :
circuit alone is anti-coagulated by administering 500-750 u/hr into the arterial line and by parlalel administration of protamine 1mg/100u of heparin.
• VARIANT OF REGIONAL ANTI-COAGULANT :
uses sodium citrate with dialysate containing no calcium. used for patients with high risk of bleeding.
• DIALYSIS WITHOUT ANTI-COAGULANTS :
Uses the saline flush technique . HD is initiated at a higher rate to reduce the thrombogenicity
and dialyzer is flushed every 15-20min with 50ml of saline.
• DIRECT THROMBIN INHIBITORS :
Hirudin, lepirudin, Argatroban
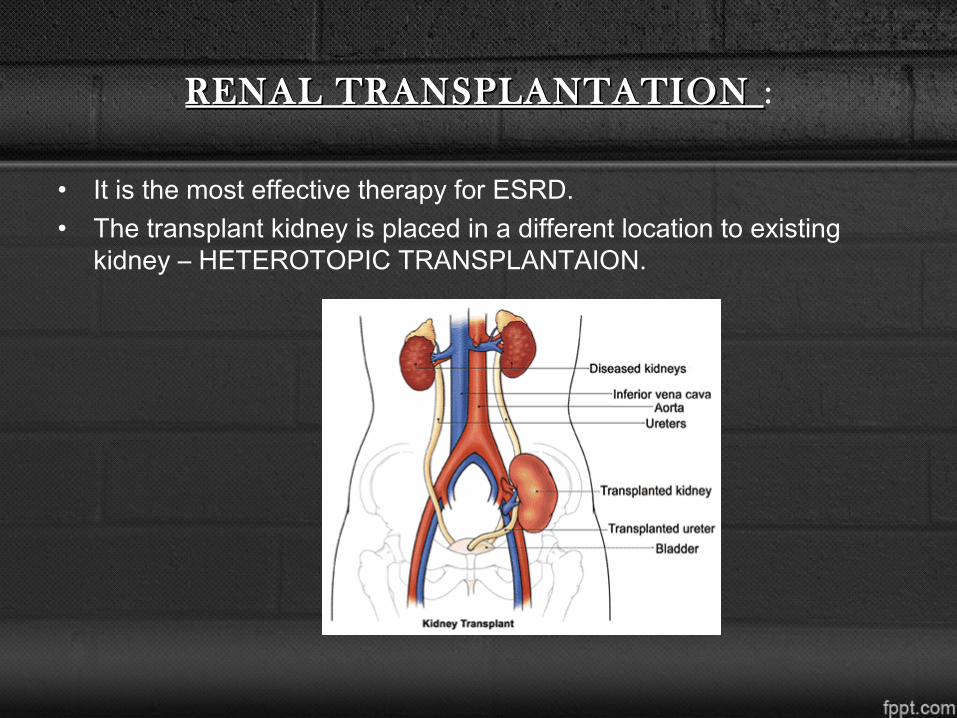
RENAL TRANSPLANTATION RENAL TRANSPLANTATION :
• It is the most effective therapy for ESRD.• The transplant kidney is placed in a different location to existing
kidney – HETEROTOPIC TRANSPLANTAION.
PLASMAPHERESIS :
• Plasma is removed from the patient and exchanged with fresh frozen plasma (FFP) and a mixture of colloid and crystalloid solutions .
• A plasma filter is used instead of hemofilter.
• Replacement (postfilter) fluid can also be a 50/50 combination of FFP and albumin.
SUMMARY :
• CRRT is now firmly established throughout the world as perhaps the most commonly used form of RRT.
• Dialysis has a century long history of pioneering physicians.• It generally works through osmosis and filtration of fluid across a
semi-permeable membrane with the use of dialysate.• There are 2 types – hemodialysis, peritoneal dialysis.• PD is often conducted in the patient’s home or extended care
facility.• The prevalence of patients with ARF requiring CRRT is high. These
patients were associated with a high ICU mortality (64%). • One of the predicting factors of better outcome is high serum
creatinine and, for worse outcome, is the requirement of MV during the ICU stay.


![THAILAND RENAL REPLACEMENT THERAPY YEAR 2011 · 2020. 8. 27. · THAILAND RENAL REPLACEMENT THERAPY YEAR 2011 ] Page 3 ACKNOWLEDGEMENTS The Thai Renal Replacement Therapy (TRT) committee](https://img.pdfslide.us/doc/110x75/6096115f208ae70f0b464852/thailand-renal-replacement-therapy-year-2011-2020-8-27-thailand-renal-replacement.jpg)









![Renal Replacement Therapy Auto Saved]](https://img.pdfslide.us/doc/110x75/577d27651a28ab4e1ea3d215/renal-replacement-therapy-auto-saved.jpg)