Embed Size (px)
Citation preview

Mohammed Abdulqader SuwaidMohammed Abdulqader Suwaid
Egyptian Fellowship Board Egyptian Fellowship Board CandidateCandidate
Medical OncologyMedical Oncology
RENAL IMPAIRMENT IN RENAL IMPAIRMENT IN MULTIPLE MYELOMAMULTIPLE MYELOMA

INTRODUCTIONINTRODUCTION

Introduction
Multiple myeloma (MM) is a clonal B-cell disease of slowly proliferating plasma cells, accompanied by monoclonal protein production and lytic bone lesions.
Common complications of MM include hypercalcemia, renal impairment, infection, skeletal lesions, and anemia. Less common complications include venous thromboembolism and the hyperviscosity syndrome.
Renal impairment affects 20-40% of new cases. Most cases are mild and easily reversible, but it may manifest as severe acute renal injury requiring dialysis.
• Advances in Chronic Kidney Disease: Volume: 19, Issue: 5, Pages: 342-35, Sep 2012
• Treatment of the complications of multiple myeloma, UpToDate 19.3

Introduction
• Advances in Chronic Kidney Disease: Volume: 19, Issue: 5, Pages: 342-35, Sep 2012
Renal impairment is associated with a large tumor mass and consequently confers a poor prognosis.
The prognosis of MM has been improved with the introduction of novel agents and autologous stem cell transplantation.
These improvements appear to apply equally to patients with renal impairment, although the risk of complications is usually higher in this group of patients.
In addition to improved overall survival, there is some evidence that novel therapies have improved the renal prognosis.

ETIOLOGY

Etiology
Nephropathy is one of the serious adverse complications that can be observed at the time of clinical presentation of MM.
The etiology of renal failure can be multifactorial.
It is usually the result of monoclonal immunoglobulin light chains.
In rare occasions, monoclonal heavy chains or the entire immunoglobulins may be involved.
Non-monoclonal protein-related renal injury may also occur.
• Devita, Hellman & Rosenberg's Cancer: Principles & Practice of Oncology, 8th Edition
• Types of renal disease in multiple myeloma, UpToDate 19.3

Etiology
• Types of renal disease in multiple myeloma, UpToDate 19.3
The types of kidney disease can be classified by the primary site of injury into: Glomerular
Primary (AL or rarely AH) amyloidosis Monoclonal immunoglobulin deposition (light chain
deposition disease, heavy chain deposition disease, and light and heavy chain deposition disease)
Miscellaneous (monoclonal cryoglobulinemia, proliferative glomerulonephritis due to monoclonal IgG deposition)

Etiology
• Types of renal disease in multiple myeloma, UpToDate 19.3
The types of kidney disease can be classified by the primary site of injury into: Tubular
Light chain cast nephropathy (myeloma kidney)
Distal tubular dysfunction Proximal tubule dysfunction
or acquired Fanconi's syndrome Interstitial
Plasma cell infiltration Interstitial nephritis
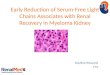
Myeloma kidney. Dense intratubular casts are shown, with accompanying tubular cell atrophy (H&E, x200).

Etiology
Additional factors exacerbating renal failure in myeloma patients include: Volume depletion Use of nonsteroidal anti-inflammatory drugs for
pain control Hyperuricemia Nephrotoxic chemotherapeutic agents Intravenous contrast for radiographic studies Bisphosphonate therapy Calcium deposition and stones in the kidney
• Devita, Hellman & Rosenberg's Cancer: Principles & Practice of Oncology, 8th Edition
• Rodgers & Young: Bethesda Handbook of Clinical Oncology, 2nd Edition

MANAGEMENT

Diagnosis
While in some patients, renal failure is the only isolated sign of MM, other patients have further simultaneous symptoms (signs of bone destruction, hypercalcemia & cytopenia).
Therefore, differential diagnosis of renal failure should always include monoclonal gammopathy-associated nephropathy.
Early diagnosis at the time when renal impairment is still reversible is extremely important for the patient's prognosis.
• The Treatment of Renal Failure in Multiple Myeloma: Vnitr Lek. 2009 Jun; 55(6): 570-82.

Diagnosis
• Types of renal disease in multiple myeloma, UpToDate 19.3
The diagnosis must be suspected in the older patient presenting with acute or subacute renal failure, particularly if the urine dipstick is negative for protein, whether or not the patient has a previously diagnosed MM or monoclonal gammopathy.
The diagnosis can only be made definitively with a kidney biopsy. However, the diagnosis is often established in cases of acute renal failure by identifying the presence of large amounts of monoclonal free light chains in the serum and the presence of a monoclonal protein in the urine, by protein electrophoresis and immunofixation.

Treatment
• The Treatment of Renal Failure in Multiple Myeloma: Vnitr Lek. 2009 Jun; 55(6): 570-82.
Reversible causes (Dehydration, ↑ Ca++, NSAID-induced, IV contrast) should always be excluded or corrected accordingly.
Treatment regimens with high-dose glucocorticoids form the basis of treatment.
Combined treatments with new, highly effective drugs (bortezomib or thalidomide) with high-dose glucocorticoids and an alkylating cytostatic agent, or with doxorubicin, have the fastest onset of action and thus provide the highest likelihood that hematological treatment response will be followed by improved renal function.

Treatment
• The Treatment of Renal Failure in Multiple Myeloma: Vnitr Lek. 2009 Jun; 55(6): 570-82.
High-dose chemotherapy is recommended in patients with persisting renal failure, particularly in the subgroup of patients with chemotherapy-sensitive disease.

No Yes
Yes
No
No
No Yes
Yes
No Yes
Algorithm to approach renal failure in MM•Approach to acute renal failure with multiple myeloma: role of plasmapheresis. Ther Apher Dial. 2005 Oct;9(5):417-22.

SUMMARY

Summary
Renal impairment is a common complication of MM.
The most important causes include: light chain tubular casts (myeloma kidney). Hypercalcemia. light chain deposition disease (associated with kappa
light chain). AL amyloidosis (associated with lambda light chain). Others (e.g. NSAIDs, hyperuricemia, chemotherapy, IV
contrast, etc.)

Summary
It was generally associated a poor prognosis but with introduction of novel therapies renal prognosis have been improved.
Treatment depends on: good hydration correction of hypercalcemia or any contributing
condition use of effective agents which are safe in renal
impairment (e.g. steroids, melphalan, cyclophosphamide, bortezomib, and thalidomide)
Plasmapheresis &/or dialysis (in certain situations)

January 20January 20thth, 2013, 2013
TT h a nh a n k Y ok Y o uu