Embed Size (px)
Citation preview

الرحيم الرحمن الله بسمRenal Failure
St: khalil shawamri
Major : Nursing
Ibn Sina Collage * Palestine

Out Line: Glossary Definition of ARF Etiology Risk Factor Symptoms of ARF Phases of ARF RIFLE Criteria Diagnoses

Lab Finding Treatment Indication for Dialysis Nutrition therapy Prevention Complication NSG . management & NSG. Diagnosis Conclusion

Glossary-:
Urea : waste product of protein.
Creatinine : waste product of muscle energy.
Azotemia : abnormal concentration of nitrogenous waste in blood.
Uremia : excess of urea and other nitrogenous waste in blood.
GFR : total rate of filtration of blood by the kidney
Creatinine Clerance : rate of filtration of creatinine by the kidney.
ESRF : end stage renal failure, uremia requiring transplantation or dialysis.
Anuria – no urine output or less than 100mls/24 hours
Oliguria - <500mls urine output/24 hours or <20mls/hour
Polyuria - >2.5L/24 hours

ACUTE RENAL FAILURE
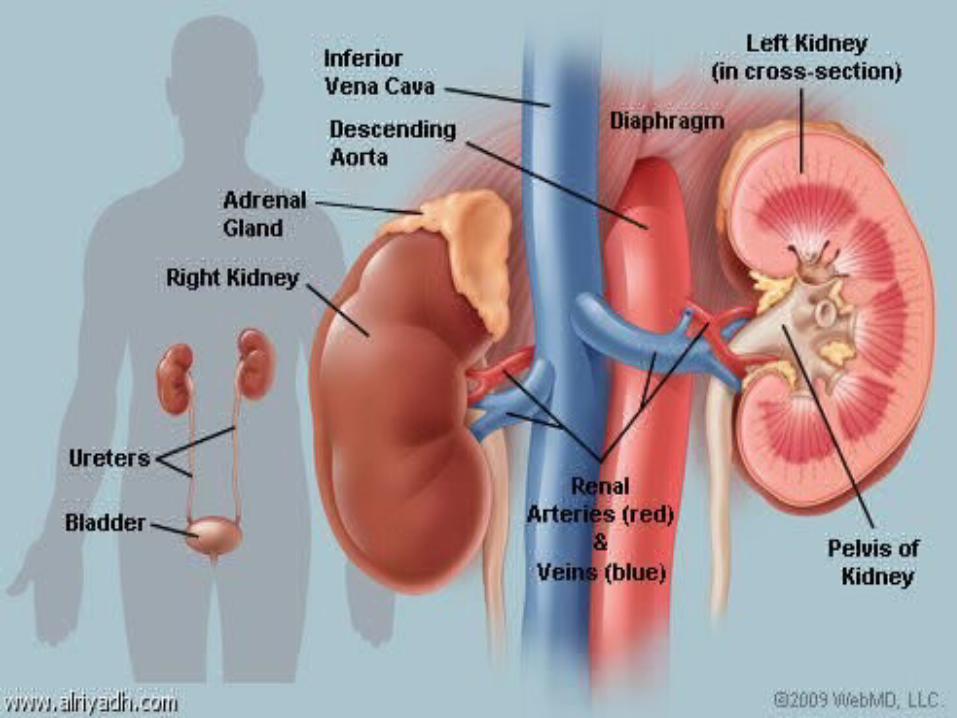
FiltrationReabsorbtionSecretion

DEFINITIONS
Different to renal insufficiency where kidney function is deranged but can still support life
Acute renal failure is a sudden reduction in kidney
function that results in nitrogenous wastes accumulating in the blood.

ETIOLOGY of ARF
Pre renal (functional): Decreased renal perfusion without cellular injury 70% of community acquired cases 40% hospital acquired cases
Renal-intrinsic (structural): Glomerulonephritis (GN) Acute interstitial Necrosis (AIN) Acute tubular necrosis (ATN)
Post renal (obstruction): Post renal obstruction Obstruction to the urinary outflow tract

Problems affecting the flow of blood before it reaches the kidneys
1) Dehydration vomiting, diarrhea, or blood loss.
2) Disruption of blood flow to the kidneys Major surgery with blood loss, severe injury or burns, or infection in the bloodstream.
Blockage or narrowing of a blood vessel carrying blood to the kidneys.
Heart failure or heart attacks causing low blood flow.
Pre-renal

Renal damage (intrarenal)
Renal Problems with the kidney itself that prevent proper filtration of blood or production of urine(25-40%).
Blood vessel diseases Blood clot in a vessel in the kidneys Injury to kidney tissue and cells

Glomerulo nephritis
e.g, Streptococcal bacterial infections may damage the glomeruli.
Acute interstitial nephritis 1) Medications such as antibiotics, anti-inflammatory
medicines (for example, aspirin, ibrufen), and water pills .
2) infections and immune-related diseases such as lupus , leukemia, lymphoma, and sarcoidosis.

Acute tubular necrosis

Causes include shock (decreased blood supply to the kidneys), drugs (especially antibiotics) and chemotherapy agents, toxins and poisons, and dyes used in certain kinds of x-rays.
Accidents, injuries
complications from surgeries (eg.Heart-bypass surgery)
Polycystic kidney.
produce less erythropoietin
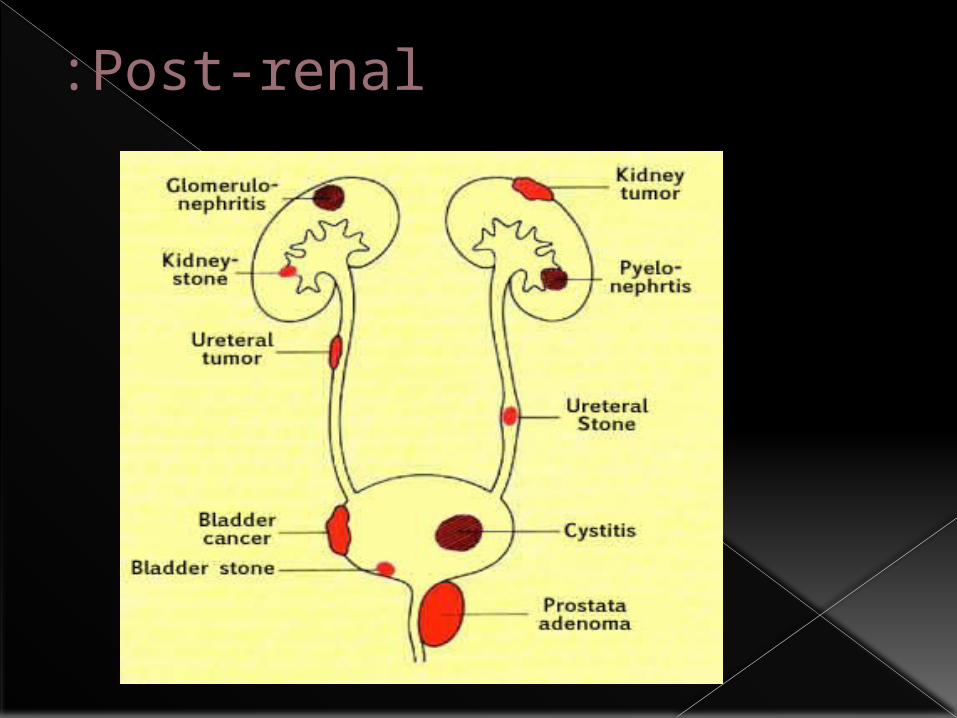
Post-renal:

RISK FACTORS
Advanced age Blockages in the blood vessels in your arms or legs Diabetes High blood pressure Heart failure Kidney diseases Liver disease

Symptoms Vomiting and/or diarrhea, which may lead to dehydration. Nausea. Weight loss. Nocturnal urination. pale urine. Less frequent urination, or in smaller amounts than usual,
with dark coloured urine Feeling tired and/or weak. Memory problems. Difficulty concentrating. Dizziness. Low blood pressure.

Haematuria. Pressure, or difficulty urinating. Itching. Bone damage. Non-union in broken bones. Muscle cramps (caused by low levels of calcium which can
cause hypocalcaemia).: Abnormal heart rhythms. Muscle paralysis. Swelling of the legs, ankles, feet, face and/or hands. Shortness of breath due to extra fluid on the lungs Pain in the back or side

Other symptoms include
Anorexia Pruritus Seizures (if blood urea nitrogen level is very high) Shortness of breath (if volume overload is present). Decrease osmolality(A measurement of urine concentration that
depends on the number of particles dissolved in it). Increase urinary sodium. Pericarditis. Pericardial effusion. Pleural effusion. Decrease calcium and bicarbonate. Defect in platelet functionings

PHASES OF ARF
Initiating phase : period from elapse from the occurrence of disease to beginning change of U/O and may be from several hours to 2days
Maintenance phase : intrinsic renal damage is established ,
GFR 5-10ml/min , and may be 400ml/24hrs (oligurea), and may be from 8-14 day and may up to 11 month and renal complication start.
Recovery phase : renal tissue recovered & repair itself and it may up to 4-6 months


Diagnosis
History collection. Physical examination.
1 Asterixis and myoclonus
2 Peripheral edema (if volume overload is present)
3 Pulmonary rales (if volume overload is present)
4 Elevated right atrial pressure (if volume overload is present)

Lab findings
Rising creatinine and urea Rising potassium Decreasing Hb Acidosis Hyponatraemia Hypocalcaemia

Identification of precipitating cause. Serum creatinine and BUN level .(n 7-18mg/dl) Serum electrolytes. Urine analysis. Renal bladder ultra sound. Renal scan. CT scans and MRI scan (to identify lesion and
masses) The urine will be examined under a microscope. biopsy

Hydronephrosis

Normal Renal Ultrasound

Hydronephrosis

Hydronephrosis

Nephrolithiasis

Wilms tumer of the kidney
Medical and Pharmacological Treatment
correcting fluid and electrolyte balance. Correct dehydration. Correct dehydration. Keeps other body systems working properly Furosemide, Torsemide calcium gluconate Sodium bicarbonate Dialysis( it will be discussed later with Mai )

Indications for acute dialysis
AEIOU Acidosis (metabolic) Electrolytes (hyperkalemia) Ingestion of drugs/Ischemia Overload (fluid) Uremia

NUTRITIONAL THERAPY
Provide protein diet. Calori requirements are met with high
carbo-hydrate meals (carbo-hydrates have a protein-sparing effect).
Foods and fluid containing potassium or phosphorous (banana, coffee) are restricted.
Patient may require parenteral nutrition.

Prevention A careful history(nephrotoxic antibiotic agent
aminoglycosides, gentamicin, tobramicine, etc.) blood tests and urinalysis Drink enough fluids Difficulties urinating or blood in the urine should
prompt a visit Treat hypotension promptly. Prevent and treat infections promptly. Pay special attention to wound, burns and other
precursors of sepsis.

COMPLICATIONS
ARF can affect the entire body Infection Hyperkalaemia, Hyperphosphataemia, hyponatraemia water overload Pericarditis Pulmonary oedema. Reduced level of consciousness. Immune deficiency.

NURSING MANAGEMENT & NSG Diagnoses
Providing skin care Providing support Monitor weight daily Monitor lab results & Urine Out put Teach Pt about nutrition Diet
Diagnoses Excess fluid volume related to decreased Glomerular
filtration rate and sodium retention Sleep pattern disturbances related to disease condition Risk for infection related to alterations in the immune system
and host defenses Imbalanced nutrition: less than body requirements

Conclusion
Think about who might be vulnerable to acute renal failure
Think twice before initiating therapy that may cause ARF
Be a human while dealing with your Pt

لكم : تحياتي معKhalil shawamri Ibn Sina Collage
THANK YOU