Embed Size (px)
Citation preview

Renal tumours
Andrew PotterRegistrar
Radiation OncologyRoyal Adelaide Hospital

2004 WHO classification - kidney tumours
Renal cell tumours Metanephric tumours Nephroblastic tumours Mesenchymal tumours
Children Adults
Mixed mesenchymal and epithelial Neuroendocrine Haematopoietic/lymphoid

Renal cell carcinoma
(Renal adenocarcinoma)

Renal cell tumours
Malignant Clear cell RCC - 70% Multilocular & papillary RCC 10-15% Chromophobe RCC - 5%
Benign (5%) Oncocytoma Papillary adenoma

Familial RCC Von Hippel Lindau VHL gene 3p25-26
Multiple bilateral clear cell RCC Hereditary papillary RCC MET oncogene 7q31
Multiple bilateral papillary RCC Hered leiomyomatosis and RCC FH gene 1q42
Solitary unilateral tumours Birt Hogg Dube syndrome BHD gene 17p11
Multiple oncocytoma, chromophobe RCC Tuberous sclerosis TSC1 gene 9q34 TSC2 gene 16p13
Multiple bilateral AML

Clear cell RCC <5% multicentric or bilateral 50% stage I & II at
presentation <5% stage IV Organ involvement with
metastases 40% bone 22% adrenals 15% brain 14% kidney
Late mets up to 10+ years

Papillary RCC
70% stage I More commonly
bilateral and multifocal

Oncocytoma
Benign tumours when accurately defined 33% appear to have central stellate scar Acceptable features
Mitoses Necrosis Small foci of clear cell change
EM - numerous mitochondria “Oncocytosis”

Fuhrman Grade Assigned a Grade 1 - 4 Based on nuclear size, shape and prominence of
nucleoli Tumour is given the highest pattern present Nuclear grade 5 yr survival
1 65% 2 35% 3 30% 4 10%

TNM stagingT - primary tumourT - primary tumour
TXTX Primary tumour cannot be assessedPrimary tumour cannot be assessed
T0T0 No evidence of primary tumourNo evidence of primary tumour
T1T1 Tumour confined to kidney, <7cmTumour confined to kidney, <7cm
T1aT1a ≤≤4cm, confined to kidney4cm, confined to kidney
T1bT1b >4cm but <7cm, confined to kidney>4cm but <7cm, confined to kidney
T2T2 Tumour >7cm, confined to kidneyTumour >7cm, confined to kidney
T3T3 Tumour extends into major veins or adrenal or perinephric tissue but not Tumour extends into major veins or adrenal or perinephric tissue but not beyond Gerota’s fasciabeyond Gerota’s fascia
T3aT3a Direct invasion of adrenal gland, perirenal and/or sinus fatDirect invasion of adrenal gland, perirenal and/or sinus fat
T3bT3b Gross extension into renal vein or IVCGross extension into renal vein or IVC
T3cT3c Extends into IVC above diaphragm or wall of IVCExtends into IVC above diaphragm or wall of IVC
T4T4 Invasion beyond Gerota’s fasciaInvasion beyond Gerota’s fascia

TNM stagingN - regional lymph nodesN - regional lymph nodes
NXNX Nodes cannot be assessedNodes cannot be assessed
N0N0 Regional lymph nodes not involvedRegional lymph nodes not involved
N1N1 Metastasis in a single regional lymph nodeMetastasis in a single regional lymph node
N2N2 Metastases in >1 regional lymph nodeMetastases in >1 regional lymph node
M - distant metastasesM - distant metastases
MXMX Metastases cannot be assessedMetastases cannot be assessed
M0M0 No distant metastasesNo distant metastases
M1M1 Distant metastasesDistant metastases

Stage groupingsII T1T1 N0N0 M0M0IIII T2T2 N0N0 M0M0
IIIIIIT3T3 N0N0 M0M0T1T1 N1N1 M0M0T2T2 N1N1 M0M0
IVIV
T4T4 N0N0 M0M0T4T4 N1N1 M0M0Any TAny T N2N2 M0M0Any TAny T Any NAny N M1M1

Prognostic factors for RCC Pathologic stage 5 yr survival
T1 - 2 organ confined 70-90% T3 50-70% N+, M1 5-30%
Tumour size < 4 cm > 90% 4 - 10 cm 50% > 10 cm 0%
Histological type Clear cell 70% Papillary, Chromophobe 85% Multilocular cystic 100% Medullary, Collecting duct 0%

Surgery
Role of renal biopsy Organ confined Locally Advanced Metastatic

Indeterminate lesions Small or indeterminate renal lesions present a
management dilemma Traditional teaching was to avoid biopsy in
fear of “seeding” biopsy tract We now know that;
Tumour seeding from biopsy is rare Tumours < 4cm 25% are benign, < 1cm 50% Core biopsy has higher PPV than FNA Need experienced Pathologist to interpret

Role of renal biopsy Definite role
Lesion may relate to a systemic disease Possible metastatic disease ie. when a +’ve result excludes surgery
Suggested role When active surveillance is considered To identify benign lesions which need no
treatment When MIT is considered, and for follow up

Organ confined disease
Active surveillance Radical nephrectomy
Open Laparoscopic Da Vinci
Nephron sparing surgery (NSS) Partial nephrectomy - open or lap Minimally invasive therapies (MIT)
Cryotherapy, RFA, HIFU, interstitial LASER

Natural history of small lesions Volpe et al, Cancer 2004
32 solid lesions < 4 cm Followed median 27.9 mths with US/CT Mean growth rate 0.2 cm/yr 9 surgically removed after average 3 yrs 8 RCC, 1 oncocytoma No mets during followup
Excision is an option, but must accept risks of surgery and possibility lesion is benign or clinically insignificant

Active surveillance Contrast CT each 3-6 mths for 2 yrs to determine
baseline kinetics, increase interval Advantages
May avoid unnecessary surgery and complications Disadvantages
Burden of follow up Small but definite risk of metastases Need dedicated radiologist to compare studies
Clinical decision must balance the risks and likely benefits of both intervention and observation in an individual patient

Nephrectomy complications
Death Adjacent organ injury
Bowel, spleen, liver, pancreas, major vessels Infection Bleeding Renal impairment

Indications fornephron-sparing surgery (NSS) Absolute
nephrectomy would render patient anephric bilat tumours, solitary kidney, familial RCC
Relative Future threat to contralateral kidney
Elective Small, exophytic, polar location Benign disease

Issues with NSS Open partial remains the gold standard Recent enthusiasm for less invasive
techniques Growing awareness of natural history
30% of small lesions are benign or indolent Metastatic potential increases > 3cm
Better imaging technology available Up to 10% risk of contralateral disease

Partial nephrectomy technique Flank incision, extraperitoneal approach Mobilise within Gerota’s fascia Access to renal vessels, control with loops Mannitol Clamp renal artery Renal hypothermia Excise tumour Close vessels and collecting system Insert drain +/- stent

Outcomes Long-term outcomes approach radical nephrectomy
5y survival 90-95% Local recurrence 4-6%
Complications Mortality <1% Adjacent organ injury <1% Infection 3% Fistula/urine leak 5-10% ARF 5-10% 2 Haemorrhage 2-3%

Complications
Mortality <1% Re-operation <3% Adjacent organ injury <1% Infection/collections 3% Fistula/urine leak 5-10% ARF 5-10% 2 Haemorrhage 2-3%

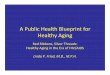
Laparoscopic partial nephrectomy Technically demanding “Softer” indications to the OPN Importance of imaging
CT with 3D reconstruction Angiography Intraoperative US
Clamping, cooling, warm ischaemic time (WIT) Difficult to reproduce open technique, often omitted Acceptable WIT 30min and longer can have
detrimental effect

3D CT reconstruction

Outcomes Similar complications, plus conversion Double the warm ischaemic time With careful selection it may approach open
technique Advantages
Decrease length of stay (2 vs 5 days) Decrease analgesia requirement
Disadvantages Increased costs and “laparoscopic” risks

Radiotherapy
Radiosensitivity of RCC is variable Animal experiments suggest a theoretical benefit
to preoperative RT (? Reduce intra-operative seeding)
Historically several series suggested clinical benefit to adjuvant (post-op) RT Limited applicability because of long time span,
improvements in staging, surgery, changing RT technology

Neo-adjuvant radiotherapy
Rotterdam study Radical nephrectomy vs neo-adjuvant RT (30Gy/15#
APPA) plus nephrectomy No overall survival or metastasis-free survival
advantage (both 50% 5-year survival) No improvement in resectability Further study to 40Gy - still no advantage
Swedish study Poorer 5-year survival with pre-op RT (47% vs 63%)!

Adjuvant radiotherapy Some early studies suggested advantage to post-op
RT but poorly designed and reported Newcastle (UK) study
Poorer survival with adjuvant RT (55Gy) vs surgery alone Not stratified by grade or stage
Copenhagen study Stage II/III disease No difference in RCC relapse Significantly more GI complications (44%) in RT group 19% of deaths attributed to RT complications

So what is the role for RT? MSKCC and Kao retrospective series
Potential benefit of RT in selected cases where there is a high risk of local failure, ie: Pre-op RT in unresectable, locally-advanced tumours
(“downstaging”), including T3a/T3c T3b (vena cava invasion) doesn’t necessarily increase risk of local
failure Incomplete resection with positive margins Lymph node involvement
RT in these cases may improve local control but probably not overall survival
Clear role in palliation

RT techniques Pre-op RT 40-50Gy to kidney + lymphatics for
unresectable lesions may improve resectability 45-50Gy post-op
10-15Gy boost (ie. ~60Gy total) to gross residual disease Include scar to reduce chance of scar recurrence
CT-planned, multifield technique Dose limitations (fully fractionated)
Liver D30 <36-40Gy Contralateral kidney <20Gy max Spinal cord <45Gy max

Cryotherapy Cryoprobes use liquid argon/nitrogen to form an
ice ball at the probes’ tip (-180C) Shown to produce predictable and reproducible
tissue destruction Tumour necrosis at -40C Double freeze-thaw cycle
Rapid freeze and slow thaw Aim to extend ice ball 1cm beyond tumour Monitor visually and with intra-operative US Percutaneous, laparoscopic, open techniques

Outcomes
Complications Pain at probe site - Ileus Collecting system injury - Fistula Adjacent organ injury - Haemorrhage
Harmon et al J Urol 2003;169:229 76 patients with mean follow up 17 mths 3 failures Considered success if -’ve biopsy, no gad
enhancement on MRI or tumour shrinkage

Radio Frequency Ablation high frequency AC causes heat-based tissue damage T 60-100ºC
denaturation of cellular protein, melting of lipids, coagulative necrosis
2 zone of damage due to vascular thrombosis Open, laparoscopic or percutaneous Difficult to monitor procedure with imaging Exophytic lesions are most suitable
“heat sink” effect of renal hilum Impedance monitoring required

Disadvantages
Incomplete ablation Need for multiple treatments Lack of real-time monitoring Serious histological concerns about
viable tumour

Minimally invasive therapy High Intensity Focussed Ultrasound (HIFU)
Extracorporeal US focused on lesion Temperature at site increases thermal injury Nonthermal injury by cavitation and cellular oscillation ablation volumes are controlled by adjusting power, duration and
location of ultrasound pulses LASER Interstitial therapy
fibre placed directly into lesion under CT/MRI heat and tissue injury using Nd:YAG 25W, 10 - 30 min

Metastatic disease Role of nephrectomy
Palliative Therapeutic
Spontaneous regression of met’s < 1 % of cases 1969 - 2000 35 papers describing 65 cases < 50% associated with nephrectomy
Role of metastectomy ? Bisphosphonates

RT techniques
Palliation Long survival is possible, even with distant
metastases, where performance status is good Encompass metastatic deposit (or local
recurrence) with 2-3cm margins Higher doses (up to 35-40Gy) may be required
to overcome radioresistance Symptomatic relief in 64-84% of patients

Chemotherapy
Metastatic RCC remains one to the most resistant cancers
Conventional therapy has little to offer ? More effective in non-clear cell tumours
Platinum, gemcitabine, doxorubicin RCT’s < 10% response, including
vinblastine Hormonal treatment is ineffective

Cytokines
15-30% response rate for clear cell tumours Small % experience a durable, complete
remission RCT’s vs placebo or observation
IL 2 - Clark et al JCO 2003 IFN - Messing et al JCO 2003 Observation superior in both No advantage to combination IL2 + IFN

SWOG 8949 241 patients randomised Received IFN 2b - 3% response 106 of 120 pt’s underwent nephrectomy Improved survival 11.1 vs 8.1 mths (p<0.05)
EORTC 30 947 85 patients IFN 2b nephrectomy 29/42 completed surgical arm vs 40/42 Improved survival 17 vs 7 mths (p<0.05)

Tyrosine kinase receptor inhibitors
Sunitinib TK receptor inhibitor Interferes with tumour angiogenesis Partial responses up to 40% Up to 10% complete response Median time to progression ~8 months

Renal pelvis/ureteric carcinoma

Renal pelvis/ureteric carcinoma
Transitional cell (“urothelial”) carcinoma 7% of renal neoplasms 1.5-2% bilateral (synchronous) 6-8% bilateral (asynchronous) M:F = 2-3:1 Most common age 50-70 years Increased risk of other urinary tract malignancies
(eg. Bladder)

Natural history and presentation
Frequently multi-focal Haematogenous and lymphatic metastases Metastasis relates to histologic grade Presents with
Haematuria (70-95%) Pain (8-40%) Flank mass (10-20%) Bladder irritation(5-10%)



TNM stagingT - primary tumourT - primary tumourTXTX Primary tumour cannot be assessedPrimary tumour cannot be assessedT0T0 No evidence of primary tumourNo evidence of primary tumourTaTa Papillary, non-invasive carcinomaPapillary, non-invasive carcinomaTisTis Carcinoma Carcinoma in situin situT1T1 Tumour invades subepithelian connective tissueTumour invades subepithelian connective tissueT2T2 Tumour invades muscularisTumour invades muscularisT3T3 (For renal pelvis only) tumour invades into peripelvic fat or into (For renal pelvis only) tumour invades into peripelvic fat or into
renal parenchymarenal parenchymaT3T3 (For ureter only) tumour invades into periureteric fat(For ureter only) tumour invades into periureteric fatT4T4 Tumour invades adjacent organs or through kidney into Tumour invades adjacent organs or through kidney into
perinephric fatperinephric fat

TNM stagingN - regional lymph nodesN - regional lymph nodes
NXNX Nodes cannot be assessedNodes cannot be assessed
N0N0 Regional lymph nodes not involvedRegional lymph nodes not involved
N1N1 Metastasis in a single regional lymph node (≤2cm max)Metastasis in a single regional lymph node (≤2cm max)
N2N2 Metastases in a single regional lymph node (>2 but ≤5cm max), Metastases in a single regional lymph node (>2 but ≤5cm max), or multiple nodes (≤5cm max)or multiple nodes (≤5cm max)
M - distant metastasesM - distant metastases
MXMX Metastases cannot be assessedMetastases cannot be assessed
M0M0 No distant metastasesNo distant metastases
M1M1 Distant metastasesDistant metastases

Stage groupings0a0a TaTa N0N0 M0M00is0is TisTis N0N0 M0M0II T1T1 N0N0 M0M0IIII T2T2 N0N0 M0M0IIIIII T3T3 N0N0 M0M0
IVIVT4T4 N0N0 M0M0Any TAny T N1-N3N1-N3 M0M0Any TAny T Any NAny N M1M1

Prognostic factors
5-year survival By stage
Ta - 80% T1 - 83% T2 - 72% T3 - 51% T4 - 16%
By grade G1 - 83% G2 - 75% G3 - 52% G4 - 0%

Management
Radical nephroureterectomy Removal of contents of kidney, Gerota’s fascia,
ureter and cuff of bladder at the distal extent High loco-regional recurrence rates (30%)
with less extensive surgery Only consider local excision with small,
localised, low grade lesions or where kidney preservation is important

Adjuvant therapy Little data to support routine adjuvant RT Small series suggest improved local control with
post-op RT (40-60Gy) for T3-T4 tumours 11% vs 46% recurrence 27% vs 17% survival …in a series of 20 patients
Chemotherapy, eg. MVAC, as used in bladder protocols Again, no clear role for routine adjuvant chemo

RT techniques
For elective adjuvant RT, CTV includes renal fossa and course of ureter to bladder
CT-based planning 45-50Gy in 25# for microscopic disease 5-10Gy boost for positive nodes or gross
residual disease ? Concurrent chemotherapy

Wilms’ tumour
(Nephroblastoma)

Wilms’ tumour
Highly curable Most common renal malignancy of
childhood 7 cases per million children (<15 years) Peak incidence 3-4 years of age Sporadic or hereditary, or in the context of
genetic disorders

Associations WAGR syndrome
Wilms’ tumour, aniridia, GU malformations, mental retardation
Denys-Drash syndrome Pseudohermaphroditism, mesangial sclerosis, renal
failure, Wilms’ tumour Beckwith-Weidemann syndrome
Somatic gigantism, omphalocele, macroglossia, GU abnormalities, ear creases, hypoglycaemia, hemihypertrophy

Genetics
WT1 gene Tumour suppressor gene on chromosome 11p13 Probably has a role in glomerular and gonadal
development Seen in 82% of Wilms’ patients
WT2 Beckwith-Weidemann syndrome Maps to chromosome 11p15.5

Pathology Most are solitary, unilateral
lesions 7% bilateral 12% multifocal in single
kidney Uniform pale grey/tan
appearance, often with cysts, haemorrhage and necrosis
Pseudocaspule Extension into renal
vein/IVC

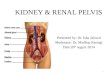
Histology
Classically 3 cell types Epithelial (tubular) (A) Blasternal
(undifferentiated, small blue cells) (B)
Stromal (C) Anaplasia is an
unfavourable histologic feature
AA
BBCC

Staging and treatment Different approaches with similar results
National Wilms’ Tumor Study Group (NWTSG), USA Nephrectomy adjuvant chemotherapy
International Society for Paediatric Oncology (SIOP) Neo-adjuvant chemotherapy nephrectomy

NWTSG staging
I - confined to kidney, completely excised II - extension beyond kidney, completely
excised III - residual tumour, confined to abdomen IV - haematogenous metastases/involved
nodes beyond abdomen/pelvis V - bilateral

NWTSG I-IV conclusions Routine post-op RT not necessary for
Stage I favourable histology Stage I anaplastic Stage II favourable histology
10 weeks vincristine + actinomycin-D sufficient Stage III favourable histology best treated with VCR/Act-
D/ADR* + 10Gy RT to flank (or 20Gy without ADR) Addition of cyclophosphamide did not improve stage IV
disease Pulse intensive actinomycin-D decreased toxicity with
equivalent efficacy
*VCR = vincristine, Act-D = actinomycin-D, ADR = doxorubicin (Adriamycin),VP16 = etoposide (don’t ask me!), CPA = cyclophosphamide

NWTSG V regimensStageStage HistologyHistology RTRT ChemoChemo DurationDuration
I-III-II FavourableFavourableNoNo VCR + ActDVCR + ActD 18 weeks18 weeks
II AnaplasticAnaplastic
III-IVIII-IV FavourableFavourableYesYes VCR + ActD + VCR + ActD +
ADRADR 24 weeks24 weeksII-IVII-IV Focal anaplasiaFocal anaplasia
II-IVII-IV AnaplasticAnaplastic YesYes VCR + CPA + VCR + CPA + VP16 + ADRVP16 + ADR 24 weeks24 weeks
I-IVI-IV Clear cell sarcoma Clear cell sarcoma of kidneyof kidney
YesYes Carboplatin + Carboplatin + VP16 + CPAVP16 + CPA 24 weeks24 weeks
I-IVI-IV Rhabdoid tumour Rhabdoid tumour of kidneyof kidney

NWTSG V radiotherapy
StageStage Favourable Favourable histologyhistology AnaplasticAnaplastic Clear cell or Clear cell or
rhabdoidrhabdoid
II No RTNo RT 10Gy to flank10Gy to flank
IIII No RTNo RT 10Gy to flank10Gy to flank 10Gy to flank10Gy to flank
IIIIII 10Gy to flank or abdomen10Gy to flank or abdomen**
IVIV12Gy whole lung12Gy whole lung##
Abdo RT if Abdo RT if operative stage IIIoperative stage III
12Gy whole lung,12Gy whole lung,Abdo RT if Abdo RT if operative stage operative stage II/IIIII/III
12Gy whole lung,12Gy whole lung,Abdo RTAbdo RT
# if lung mets on CXR * 10.8Gy/6# flank or 10.5Gy/7# abdomen

SIOP staging (at time of surgery) I - confined to kidney, completely excised II - extending beyond kidney, completely excised
Invasion beyond capsule (perirenal/perihilar fat) Invasion of regional lymph nodes (N+) Invasion of external vessels Invasion of ureter
III - incomplete excision, without haematogenous metastases Preoperative biopsy Preoperative or perioperative rupture Invasion of extra-regional lymph nodes
IV - distant metastases V - bilateral renal tumours

SIOP studies
Staging and histological diagnosis delayed until after neoadjuvant chemo and surgery completed
SIOP-1 - pre-operative RT reduces intra-operative tumour rupture
SIOP-2 - 6 months post-op chemo produced same DFS and OS as 15 months chemo
SIOP-5 - pre-op chemo gave similar results to pre-op RT (in terms of tumour spill and staging)

SIOP studies
SIOP-6 - no difference in OS for stage I receiving 17 vs 38 weeks post-op chemo, post-op RT prevents local recurrence where nodes are involved
SIOP-9 - optimum pre-operative chemo 4 weeks (no advantage to 8 weeks). Epirubicin overcame local recurrence in stage II disease

SIOP 93-01
Pre-operative chemo: vincristine weekly for 4 weeks, 2 courses of Act-D (days 1,2,3 and 14,15,16)
Post-op chemo based on stage and pathological response to chemo - tumour graded as low, intermediate or high risk

SIOP 93-01
Stage I intermediate or stage I high risk - all received Further weekly vincristine for 4 weeks Act-D days 8-12 Randomised to further chemo (weeks 10,17) or
no therapy No difference in survival at 2 years (88.8% vs
91.4%)

SIOP radiotherapy
RT limited to post-op only Indications
Favourable histology stage II (N+) and stage III receive 15Gy
Anaplastic stage II/III and clear cell sarcoma stages I-III receive 30Gy
Stage IV receive whole lung RT only where lung mets still seen on post-op CXR

Important RT considerations Open lines of communication with paediatric oncologists,
surgeons, pathologists Book planning session & machine time (can always cancel)
prior to surgery Is an anaesthetic required?
(<4-5yo, but individualise) Allow time for discussion with parents Child must be stable post-op, free of ileus or diarrhoea,
ANC >1000, Hb >10, plats.>75,000 Interaction with chemotherapy agents (Act-D &
doxorubicin)

Flank RT (1)AT PRESENTATION
Favourable Histology (stage III) residual disease postop (micro/macroscopic) confined to flank* Hilar nodes Para-aortic nodes
Anaplastic Wilms tumour Indications as above , but also include Stage II
*Boost 10.8Gy to macro disease >3cm in max. diameter

Flank RT
Clear Cell Sarcoma of the Kidney All stages when abdominal disease confined to flank
Rhabdoid Tumour of the kidney As above Stage III (gross residual disease) Stage IV…+/- RT week 6 after assessment of response
to CT

Flank RT
(2) AT RELAPSE Localised intra-abdominal relapse

Flank RT TIMING
Start no later than day 9
VOLUME Determined by pre-op CT outline of the kidney and any
associated tumour with a 1cm margin (PTV) (include nodes if positive)
cross midline to cover full width of vertebral bodies at levels concerned (avoid contralateral kidney)
4-6 MV photons AP:PA

Flank RT
DOSE 10.8Gy/6fractions

Whole Abdominal RT (WART) INDICATIONS
Peritoneal seeding
Gross residual abdominal disease*
Preoperative intraperitoneal rupture
Diffuse/major operative spill
*Local 10.8Gy supplements to volumes > 3cm or more in max. diameter.

WART TIMING
NO later than day 9 VOLUME
To cover the whole intraperitoneal cavity
Diaphragmatic domes to the bottoms of the obturator foramina. Exclude femoral heads
4-6 MV photons AP:PA
DOSE 10.5Gy/7 fractions

Whole lung RT INDICATIONS
Pulmonary metastases at diagnosis(Stage IV) Pulmonary mets. at relapse.
ISSUES Remains controversial CXR detected vs “CT only” mets Pathologically confirmed solitary nodule At relapse give at end of CT Localised foci of disease persisting 2 weeks after 12Gy can be either
excised or be given additional 7.5Gy <18 months, give trial of CT alone.

Whole lung RT VOLUME From apex of lung to
posteroinferior recess of costophrenic angles (~level of L1), block shoulders
Simulate in quiet respiration (image intensifier)
AP:PA 6 MV photons Dose: 12Gy/1.5Gy per
fraction

Metastases BONE
field includes obvious disease with a 3cm margin 30.6Gy
BRAIN Whole brain 30.6Gy (1.8Gy/#)
LIVER RT only if unresectable 2cm margin if localised Dose 19.8-30.6Gy, depending on volume

Criticisms
NWTSG Higher intra-operative
tumour spillage (reduced DFS but equivalent OS)
SIOP No up-front
histological diagnosis (5% incorrect)
“True” pre-op staging not known
? Under-treatment by down-staging

OutcomesSIOP-9SIOP-9 NWTSG VNWTSG V
DFSDFS OSOS DFSDFS OSOS
2 years2 years
I-IIII-III 89%89% 93%93% 86%86% 96%96%
IVIV 70%70% 85%85% 72%72% 86%86%
4 years4 years
I-IIII-III 87%87% 90%90% 86%86% 95%95%
IVIV 65%65% 81%81% 69%69% 81%81%