Embed Size (px)
Citation preview

Reflex TutorialTemplate / concept Copyright (c) 2001, 2002 AuDStudent.com
All rights reserved.Content Copyright (c) 2002 Nova Southeastern University
Teri Hamill, Ph.D., FAAA, CCC-A

1) What muscles contract during the acoustic reflex? • Primarily, the stapedius. Most research says that the tensor tympani is not active in humans.Contraction of the stapedial muscle stiffens the middle ear system, and the added stiffness reduces the transmission of low-frequency sound.

2) When do normal hearing people have an acoustic reflex? • When a loud sound occurs a stapedial reflex occurs. Loud sounds are sounds about 70 dB HL and louder. Some normal hearers will not have a reflex until the sound is as high as 95 or 100 dB HL.You can also have a reflex to non- auditory stimuli. For example, a puff of air to the eye will cause a stapedial reflex.
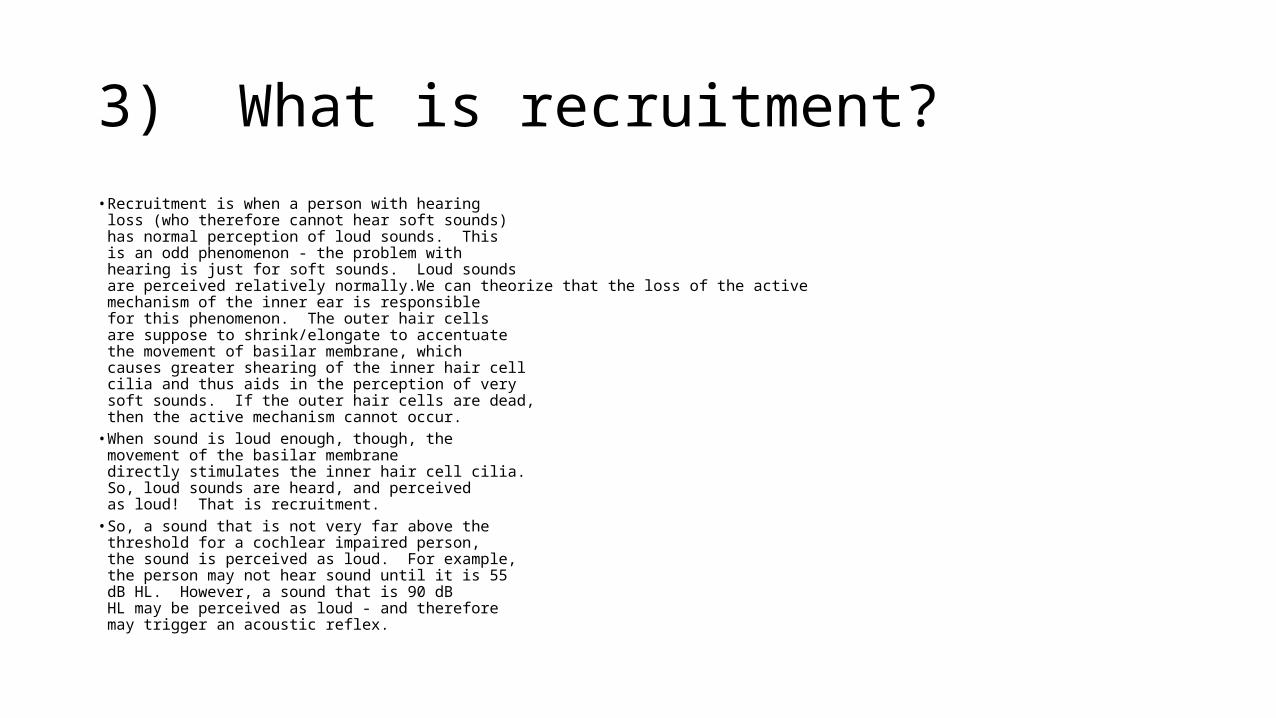
3) What is recruitment? • Recruitment is when a person with hearing
loss (who therefore cannot hear soft sounds) has normal perception of loud sounds. This is an odd phenomenon - the problem with hearing is just for soft sounds. Loud sounds are perceived relatively normally.We can theorize that the loss of the active mechanism of the inner ear is responsible for this phenomenon. The outer hair cells are suppose to shrink/elongate to accentuate the movement of basilar membrane, whichcauses greater shearing of the inner hair cell cilia and thus aids in the perception of very soft sounds. If the outer hair cells are dead, then the active mechanism cannot occur.
• When sound is loud enough, though, the movement of the basilar membrane directly stimulates the inner hair cell cilia. So, loud sounds are heard, and perceived as loud! That is recruitment.
• So, a sound that is not very far above the threshold for a cochlear impaired person, the sound is perceived as loud. For example, the person may not hear sound until it is 55 dB HL. However, a sound that is 90 dB HL may be perceived as loud - and therefore may trigger an acoustic reflex.

4) Will all people with a cochlear loss have recruitment? • The easy answer is yes. The truth is, it
depends on how severe the cochlear loss is, and how you define recruitment.If you define recruitment as a dynamic range (between threshold and UCL) of 65 dB HLor less, then you could have someone with a mild cochlear loss (say a 30 dB HL threshold) who has good tolerance for loud sounds (example: 100 dB HL UCL), then the dyanmic range could be normal (70 dB HL in this example). So, that person would not have recruitment; his/ her dynamic range is 70, which is still in the normal range.
• Similarly, if you use the acoustic reflex to determine threshold, and consider the difference between threshold of hearing and threshold of the reflex as your means of identifying recruitment, you could occasionally find a patient with cochlear loss who does not have recruitment. We will explore computing sensation level of reflexes and using that to infer about recruitment below.

5) Will people with a retrocochlear or conductive loss have recruitment? • Not unless they have some cochlear damage too!

6) Will people with cochlear losses have acoustic reflexes? At what intensity? • Most people with mild to moderately severe cochlear hearing loss will have acoustic reflexes. These people have recruitment.If the loss is severe to profound, then the problem is not just loss of inner hair cells. They may not hear loud sounds normally and therefore may not have a reflex at the intensities at which we can test. (Turn it up enough above threshold, and the person should have a reflex, but the immittance device can only create sounds to 90 to 100 dB HL in many cases.)

7) What are the parts of the acoustic reflex measurement system? The device, just like the tympanometery,
has a sound generator to produce the 226 Hz probe tone. It has a pressure pump, and a manometer to measure the pressure in the hermetically (air-tight) sealed ear canal. It has a measuring microphone that measures the intensity of the sound in the ear canal.Additionally, there is a sound generator to create the loud reflex eliciting sounds, and a way to control the intensity and frequency of the reflex eliciting sounds.The reflex eliciting sounds can be channeled to the probe, or can be sent to the earphonefor the other ear. Sometimes the earphone looks like a regular earphone, sometimes itis a second probe, but the probe only has the speaker. The second probe doesn't create air pressure or measure the level of the 226 Hz tone.

• If a loud sound is presented to just one ear (monaural presentation), the reflex in normal hearers will occur bilaterally. Since the reflex pathway has decussations (the neural pathways cross the head), the reflex can occur in both ears, even though the stimulus was just to one ear.The reflex can be measured ipsilaterally - the uncrossed pathway is tested. The loud sound goes to the same ear where the measurement of the reflex takes place.
8) What does it mean when you say an acoustic reflex can be elicited monaurally, but measured either ipsilaterally or contralaterally?
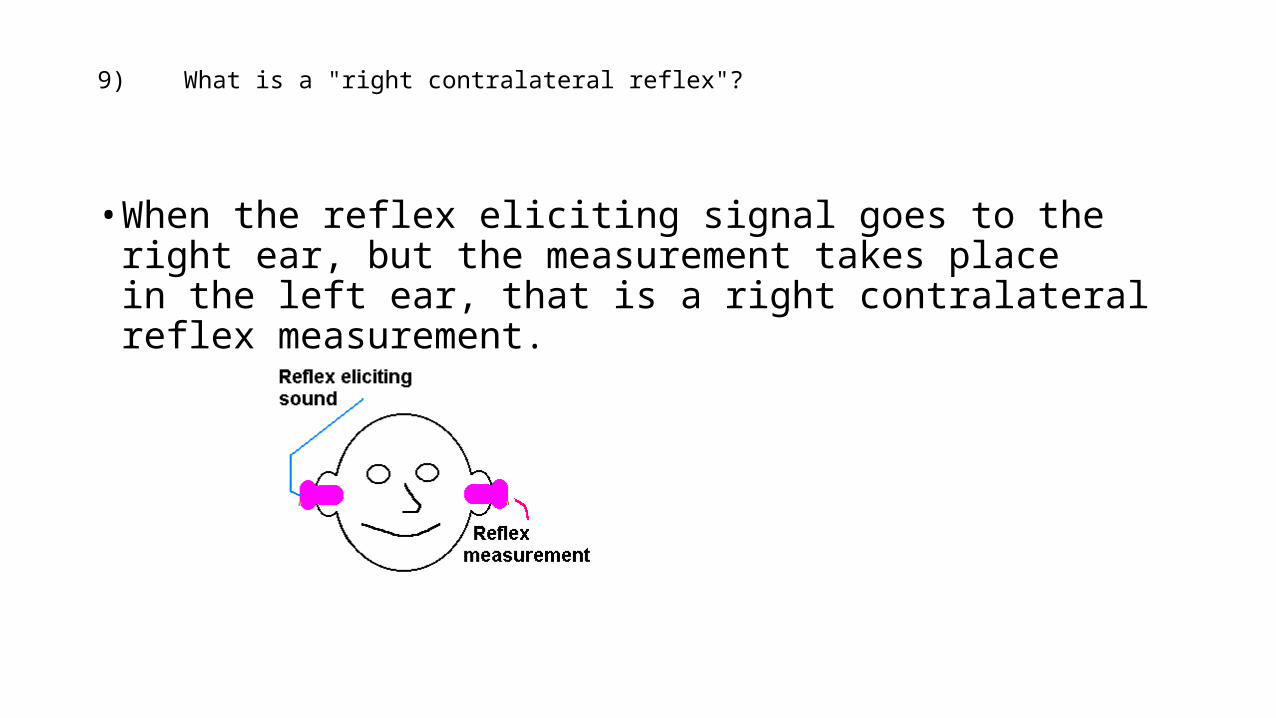
• When the reflex eliciting signal goes to the right ear, but the measurement takes place in the left ear, that is a right contralateral reflex measurement.
9) What is a "right contralateral reflex"?

10) If a person has a 50 dB HL loss at all frequencies, and the loss is cochlear in origin, and that person then has an acoustic reflex at, let's say 1000 Hz at 95 dB HL, what is the sensation level of that reflex? How do you calculate reflex sensation level?
• The difference between the acoustic reflex threshold (ART) and the hearing threshold is 45 dB, so the reflex occurred at 45 dB SL.

11) A person's hearing threshold is 30 dB HL, and the ipsilateral reflex occurs at 85 dB HL at the same frequency and ear. What is the sensation level of the reflex? • 85 - 30 = 55; the reflex occurred 55 dB above threshold, or at 55 dB SL.

12) Normal hearers have acoustic reflexes at what intensity hearing level, and what intensity sensation level?
• reflex typically occurs at around 65 or 70 dB HL on the low end, to as high as 100 dB HL. So the range of normal reflexes is 65-100 or 70-100 (depends on the text you read.)• Since a normal hearer should have thresholds of zero, then the sensation level of the reflex should be 65 to 100 or 70 to 100 also.• So, the range of normal is 65/70-100 dB HL and dB SL.

13) Why does a reduced sensation level reflex indicate cochlear pathology?
• Since a person with a mild to moderately severe cochlear loss hears loud sounds normally, the reflex threshold will probably stay in the range of 65 to 100 dB HL.Since threshold is elevated, the gap between hearing threshold and the reflex threshold narrows. This means the person has recruitment.• Recruitment can be demonstrated by having reduced sensation level acoustic reflexes.• (Reread answers for 3 and 4 if this is still not sinking in!)

14) Does a person with a conductive loss typically have an ipsilateral acoustic reflex in the ear with the conductive problem?
• Most likely, no.The weight and stiffness of the pathological substance in the ear with a conductive loss creates a situation where the acoustic reflex can't be measured. The stapedial muscle may be contracting if a loud sound was perceived, but the contraction of the reflex can't create a measurable increase in the stiffness of the already unmoving middle ear system.

15) What if the person has a slight conductive loss in the right ear, but normal middle ear function in the left ear. You are measuring a right contralateral reflex. Do you think you will see a reflex? At what levels?
• Looking at the figure below, a sound is input to the right ear. The sound is attenauted sligthly by the pathology (illustrated with the red squiggle in the middle ear), but it is still a loud sound when it reaches the cochlea. A nerve signal is created, coding that as a loud sound. The reflex path is activated, including the orange, suggesting the crossed pathway. A signal to the left stapedial muscle is sent (green). The stapedius contracts (pink). The 226 Hz probe tone in the left ear monitors the sound bouncing off the eardrum, and sees the change (the increase in reflection) when the reflex occurs.

16) What reflex threshold findings are typical of retrocochlear involvement? Why?
• With a retrocochlear pathology, there are two reasons you may not see a reflex.There is non-recruiting hearing loss. Loudsounds just aren't all that loud due to the loss of sensitivity for all sounds with the nerve damage.
• Plus, the nerve damage may create a change in the stapedial muscle signal when that pathway is damaged as well. The VII nerve runs through the internal auditory meatus, and a tumor in that area can damage the stapedial reflex directly.
• Early in the pathology, the reflex may be present. We would look for other signs forthe presence of a smaller tumor.
17) What is tone decay? What is reflex decay? • Tone decay is the perception of a gradual decrease in the loudness of a tone, which is held at a constant frequency and intensity. The tone fades to inaudible.Reflex decay is the gradual reduction in the strength of a reflex even though the reflex eliciting signal remains on. The reflex fades away.
18) What pathologies have abnormal reflex decay?
• Retrocochlear pathologies are associated with reflex decay.

19) What does a reflex decay trace look like? What is the criterion for abnormal decay, since normal hearers can have some decay. • Reflex decay testing is conducted with the
tone set 10 dB above the reflex threshold. The person is presented with the tone for 10 seconds. However, some decay of the reflex occurs in normal hearers. We are only concerned if the reflex decay happensat frequencies 1000 Hz and lower, and if the decay happens in the first 5 seconds. Further, the decay has to be "significant", that is, it has to reduce to half strength.
• Here is a perfect reflex, that hardly decays at all.
• This reflex decays away more than half theway back - the decay amount is significant, but it happened after the 5 second mark, so it is not considered significant decay.
• This illustrates significant decay; the decay occurs in the first five seconds.

• Cochlear losses tend to have acoustic reflexes present at normal hearing levels (< 100 dB HL).Calculating the sensation level of the reflex shows the reflex occurred at a reduced sensation level - it is less than 65 dB abovethe hearing threshold for the same ear and frequency.
• Significant reflex decay is not expected with a cochlear loss.
• Conductive loss patients will be expected to have absent ipsilateral acoustic reflexes.The contralateral reflex could be present ifthe loss is unilateral and not too severe, and if the probe is an ear without pathology.
• If a reflex is found, it will be at a normal sensation level, but the conductive loss will probably elevate the hearing level at whichthe reflex occurred.
• Retrocochlear loss ears may have absent reflexes, or ones present at elevated hearing and/or sensation levels. Early in the disease the reflex may be present, but reflex decaywould be found.
20) To recap, what are the reflex findings anticipated with a cochlear loss? With a conductive loss? With a retrocochlear loss?